
Abstract
Abstract
Purpose
The purpose of this study was to evaluate the impact of asymmetric hip dysplasia on the outcome of hip reconstruction in patients with cerebral palsy according to preoperative migration percentage (MP).
Methods
This study was institutional review board-approved for retrospective cohort review. From 2008 to 2018, 65 patients met inclusion criteria: Gross Motor Function Scale Classification (GMFSC) III to V with spastic hips (MP > 30%) who underwent bilateral hip reconstruction, with a follow-up > 24 months. Main exclusion criteria: children with associated syndromes or chromosomal disorders. The cohort was subdivided into three groups according to preoperative MP difference between hips: Group A > 50%, group B 20% to 50% and Group C < 20%. Subsequently, the groups were analyzed individually and then compared. The asymmetry of extended abduction of the hip was also evaluated and separated into three groups: no asymmetry (< 20° difference), mild asymmetry (20° to 50° difference) and severe (> 50° difference).
Results
In total, 65 patients underwent bilateral bony reconstructive surgery (130 hips). Mean age at surgery was 10.1 years (sd 3.6; 3.6 to 18.4). Mean age at follow-up was 14.7 years (sd 3.8; 8 to 21). Preoperative GMFSC distribution was grade III (four, 6%), IV (15, 23%) and V (46, 71%). In all, 21 symmetric hips (< 20% MP difference) had a preoperative MP difference of 9% and a follow-up MP difference of 18% (p > 0.05); 32 had a preoperative MP difference of 34% and a follow-up MP difference of 16% (p < 0.0001); 12 had a preoperative MP difference of 80% and a follow-up difference of 6% (p < 0.0001). According to pre- and postoperative abduction values, the mean high hip abduction preoperatively was 34° (sd 17°), whereas low hip abduction was 23° (sd 17°).
Conclusion
Hips with asymmetrical dysplasia and/or abduction undergoing bilateral reconstructive surgery focused on symmetric abduction, and corrected dysplasia in patients with cerebral palsy has improved symmetry in hip abduction and MP. Obtaining this goal immediately postoperatively is maintained to medium-term follow-up.
Level of Evidence
IV
Introduction
Hip dysplasia is a common disorder observed in patients with cerebral palsy (CP) leading to a negative impact on quality of life for the patient. 1 Nonambulatory patients (Gross Motor Function Classification System (GMFCS) IV to V) 2 are more prone to develop hips contractures and postural deformities. 3 The severity, type and side of the acquired deformity vary widely, and can be accompanied by pelvic obliquity, scoliosis and windblown deformity. 4 Furthermore, the degree of hip dysplasia can be quite asymmetric in many patients. The main manifestations of hip subluxation and dislocation include pain or discomfort, imbalance, loss of ability to stand and decrease in hygiene specifically in the perineal area.1,5
The migration percentage (MP) developed by Reimers in 1980 6 is the benchmark for measuring hip displacement and is used in most hip surveillance programmes.7,8 Systematic hip health programmes for patients with CP try to avoid hip dislocations and severe contractures; windblown deformities are particularly important to avoid. The windblown deformity has been defined as abduction and external rotation of one hip, while the opposite hip is in adduction and internal rotation, often with subluxation or dislocation of the adducted hip. 3 The terms windblown and windswept are used synonymously but do not have clear quantitative definitions. One clear definition is from the Swedish registry where it is defined as “Children with bilateral CP and at least 50% difference in abduction, internal, or external rotation between the left and right hips”. 9 Hip surgery (either soft-tissue preventative surgery or bony reconstructive surgery) is the procedure of choice to correct hip joint deformity in spastic hip disease. 10 However, asymmetric hip management is not well understood, causing variation in its treatment; many suggest different surgical ‘dosages’ based on this asymmetry, but this concept is not completely understood. 11 Previous reports have tried to establish the relationship between associated deformities and/or asymmetrical hips12,13 without statistical significance between parameters analyzed. Nevertheless, the goal continues to be the same: to contain the femoral head in the acetabulum, decrease pain, improve hip movement and have a relatively symmetric hip posture.
The aim of this study was to evaluate the impact of asymmetry of hip MP and abduction on the radiographical outcome of surgical management of dysplastic hips in patients with CP with medium-term outcome. The second goal is to evaluate the relationship between asymmetrical hip dysplasia, pelvic obliquity and asymmetric hip abduction posture.
Materials and methods
This study was approved by the institutional review board for a retrospective cohort review of existing medical charts and medical images from 2008 to 2018. Inclusion criteria were children with GMFSC III to V with spastic hip dysplasia (defined as an MP > 30%) who underwent bilateral hip reconstruction, and follow-up of > 24 months. In total, 151 patients with spastic hip disease were initially identified; however, 86 were excluded based on exclusion criteria, leaving 65 patients for evaluation. Exclusion criteria were patients with associated chromosomal syndromes, congenital hip dysplasia or dislocation, GMFCS I to II diplegia or hemiplegia, hypotonic CP, syndromic disabilities (arthrogryposis, spinal cord abnormality or dystonia), unilateral surgical treatment, follow-up less than 24 months and incomplete medical records.
Hip bony reconstruction surgery was defined as a varus derotation shortening osteotomy (VDRO) with or without pelvic osteotomy. The degree of varus was 90° to 110° for GMFCS IV to V and 110° to 130° for GMFCS III. The indication for pelvic obliquity was an MP > 50% or acetabular dysplasia. This was usually combined with soft-tissue surgery such as lengthening/tenotomy of the adductor longus, brevis, gracilis and/or iliopsoas to obtain symmetric hip abduction. 14 Demographic data were collected. The GMFCS levels of function were recorded. Anteroposterior pelvic radiographs were evaluated and the MPs were measured at the preoperative, the immediate postoperative and the final postoperative period. Hip abduction relative to the pelvis was assessed by physical examination with the hips and knees in full extension.
The cohort was subdivided into three groups according to preoperative MP difference. Group A was represented by patients with a preoperative MP difference between hips > 50%. (Fig 1) Group B had an MP difference between hips from 20% to 50%. (Fig 2) Group C had an MP difference between hips < 20%. (Fig 3)
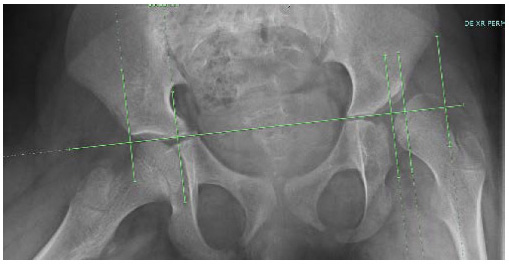
This radiograph shows an example of Group A with a difference in migration percentage (MP) of > 50%. Here, the right hip is full located into the acetabulum and the left hip has an MP of 75% for a difference in MP of 75%. Also shown are the asymmetrical hips with associated windblown deformity.
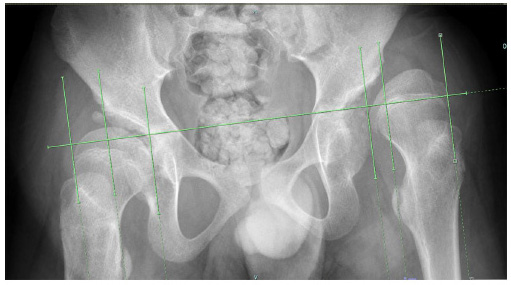
This radiograph shows an example of Group B with a difference in migration percentage (MP) of 20% to 50%. This patient has bilateral subluxated hips with MP in the right hip (45%) and left hip (80%). The difference in MP between hips is 35%.
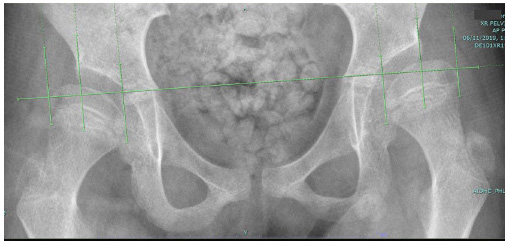
This radiograph shows an example of Group C (less than 20% difference in migration percentage (MP)) with bilateral subluxated hips with an MP in the right hip of 43% MP and 47% in the left hip with only a small difference in MP of 4% between hips.
Pelvic obliquity was measured on the supine pelvis radiograph and we considered clinical pelvic obliquity to be ≥ 10°. We considered small degrees of pelvic obliquity may be due to patient positioning and not clinically significant. Asymmetric hip was abduction defined based on physical examination of > 20° difference in hip abduction and/or a > 20 MP difference between hips. Our goal was to evaluate mild asymmetric hip abduction hips (20° to 50° difference for hip in abduction) to severe asymmetric hips (> 50° difference in hip abduction); however, we only had one severe hip so this separation was not evaluated. Data were entered into a Research Electronic Data Capture database. (REDCap, Vanderbilt, Nashville, TN, US)15,16 Frequencies and descriptive statistics were used to report the data. SPSS v. 25 (IBM Corp., Armonk, New York) was used to perform the analysis. Two-tailed paired or unpaired t-tests were used to evaluate differences between preoperative and final follow-up measures.
Results
This study included 65 patients (130 hips) with a mean age at surgery of 10.1 years (sd 3.6; 3.6 to 18.4) and age at follow-up of 14.7 years (sd 3.8; 8 to 21). Postoperative follow-up was 4.5 years (sd 1.9; 2.0 to 10.5). All patients a bilateral pattern of involvement. Preoperative GMFCS distribution was grade III (four, 6%), grade IV (15, 23%) and grade V (46, 71%). These 65 patients all had bilateral bone surgeries (130 hips). There were 11 Group A patients with severe asymmetry (> 50% MP difference), 33 Group B patients with moderate asymmetry (20% to 50% MP difference) and 21 Group C patients with mild asymmetry (< 20% MP difference).
Of the 11 Group A patients (22 hips), 55% (six patients) had asymmetric hip abduction at a mean age of 10.6 years preoperatively. All six patients had bilateral VDRO surgery and one patient had bilateral pelvic osteotomy and ten had unilateral (three right and seven left) pelvic osteotomy. The hips went from a preoperative difference in MP of 80 to a postoperative difference of 0.7 and six at final follow-up of 61 months (36 to 111) (Table 1). Of the 33 Group B patients (66 hips), 21% (seven patients) had asymmetric hip abduction at a mean age of 9.4 (range 5.8-13.8) years. All patients had bilateral VDRO surgery; five patients had bilateral pelvic osteotomy, ten on the left and 15 on the right. The group B patients went from a preoperative mean MP difference of mean 34 (SD 8.6) to a postoperative mean MP difference of 16 (SD 20) and MP difference of mean16 (SD 20) at final follow-up of 51 months (25 to 96) (Table 1). Of the 21 Group C patients (42 hips), 24% (five patients) had asymmetric hip abduction at a mean age of 11.0 (Range 4.3-16.0) years. All patients had bilateral VDRO surgery; 11 patients had bilateral pelvic osteotomy, five on the right and two on the left. The hips went from a preoperative MP difference of 9 MP (Range 0-19) (to a postoperative MP difference of 12 (Range 0-100) and 18 (Range 0-100) final follow-up of 62 months (29 to 128) months (Table 1).
Bilateral hip reconstruction surgery in 65 patients
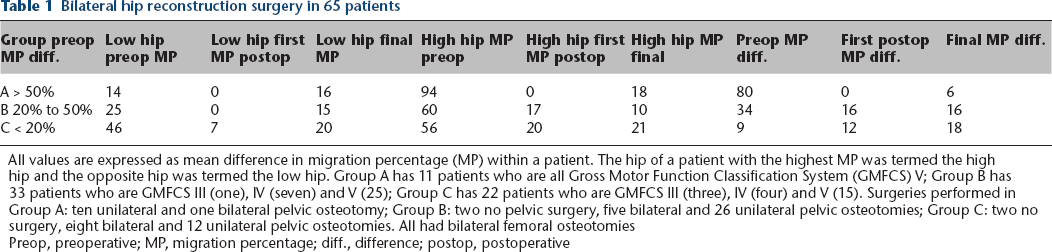
All values are expressed as mean difference in migration percentage (MP) within a patient. The hip of a patient with the highest MP was termed the high hip and the opposite hip was termed the low hip. Group A has 11 patients who are all Gross Motor Function Classification System (GMFCS) V; Group B has 33 patients who are GMFCS III (one), IV (seven) and V (25); Group C has 22 patients who are GMFCS III (three), IV (four) and V (15). Surgeries performed in Group A: ten unilateral and one bilateral pelvic osteotomy; Group B: two no pelvic surgery, five bilateral and 26 unilateral pelvic osteotomies; Group C: two no surgery, eight bilateral and 12 unilateral pelvic osteotomies. All had bilateral femoral osteotomies
Preop, preoperative; MP, migration percentage; diff., difference; postop, postoperative
The pre- and postoperative abduction values showed 28% (18 of 65 patients) had asymmetric hip abduction of ≥ 20° (mean 28°)(range 20-75) difference in hip abduction. Preoperative mean high hip abduction was 34° (sd 17°; 5° to 80°), whereas mean low hip abduction was 23° (sd 17°; 0° to 60°). At final follow-up, 9% (six patients) had asymmetry of ≥ 20° or more in hip abduction (mean 24° (20° to 30°)). Postoperative high-side hip abduction increased to a mean of 40° (sd 9°) with similar results in low hip abduction (mean 36° (sd 12°)). There was a significant increase in high hip abduction preoperatively to postoperatively (p = 0.0029), which was also true for low hip abduction (p = 0.0001). The hip with the highest degree of abduction in each patient was termed the high hip and the other hip was termed the low hip. Both the high and low hip abduction were significantly greater at follow-up than preoperatively. However, preoperative hips with ≥ 20° of abduction difference at follow-up had no remaining significant difference in amount of asymmetry (p = 0.55). There was statistical significance between the pre- and postoperative MP (p < 0.001) and the pre- and postoperative hip abduction (p = 0.007) (Table 1). There was a positive correlation between the asymmetry of hip MP and asymmetry of hip abduction (r = 0.35) (p < 0.001). However, preoperatively high MP had a nonsignificant negative correlation to preoperative low hip abduction (r = 0.14) (p = 0.27).
Based on clinical pelvic obliquity being ≥ 10°, 12 patients had pelvic obliquity a mean of 13° (10° to 20°). Postoperatively, 18 patients had a mean of 16° (10° to 36°) of pelvic obliquity. Only six of the patients who had preoperative pelvic obliquity still had a post-perative pelvic obliquity. The preoperative hip MP difference was positively correlated to degree of pelvic obliquity (r = 0.16) (p < 0.001). Preoperative hip abduction difference had a weak correlation to preoperative pelvic obliquity (r = 0.24) (p = 0.04).
Discussion
Hip dysplasia and severe contractures found in windblown postures in patients with CP lead to difficulty sitting and custodial care. 12 This is directly related to the severity of the CP. Some authors report that asymmetrical dysplastic hip deformities are not related to pelvic obliquity and scoliosis, 17 whereas another study focused on patients with asymmetric hip posture and concluded that windblown hips, pelvic obliquity and scoliosis were indeed related. 12 Patients with supra-pelvic pelvic obliquity and windblown deformity most commonly have the hip dysplasia or dislocation in the hip on the side that is most adducted and is the elevated side of the pelvic obliquity usually associated with a spine curvature in the opposite direction. 3 The asymmetric hip contractures may cause infra-pelvic pelvic obliquity by positioning the legs parallel to obtain a pelvis radiograph, the pelvis is driven up on the side with the hip adduction contracture or down the side with a hip abduction contracture. In the current study, we were not able to directly attribute the etiology of the pelvic obliquity to either the hip or the spine; however, in six of 12 patients, the obliquity resolved with reconstruction of the hips. We found weak correlations between pelvic obliquity with increased asymmetry in hip abduction and with increasing difference in hip MP asymmetry, which confirms the previously reported finding of a positive correlation between pelvic obliquity and hip asymmetry. 12
Our focus in this paper was to evaluate if hip reconstruction will correct the asymmetric hip posture, and if it remains corrected over a follow-up period in adolescence when these deformities typically become more severe. The surgical protocol used in the current study population was to do bilateral femoral osteotomies, soft-tissue lengthening if indicated by physical examination and pelvic osteotomy if acetabular dysplasia is present. Using this protocol, we found that the group with the largest asymmetry (MP > 50% difference preoperatively) had the best results with an MP difference of 6% at final follow-up. The difference in the less severe group (MP difference 20% to 59%) also improved to an MP difference of 17%; however, the initially symmetric group remained unchanged at an MP difference of 18%. There are no other reports of the radiographic outcome of symmetry, although Owers et al 18 reported improved hip abduction, flexion and containment. We also found improved hip abduction on both sides at final follow-up; however, we did not find improvement of the abduction asymmetry in the whole population.
Multiple reports found high rates of recurrent hip subluxation or dislocation on the non-operated side after unilateral hip surgery in children with CP.11,19 With our exclusion criteria, one of which was MP of > 30%, we reviewed unilateral hips to determine the impact of unilateral surgery on subsequent asymmetry in both motion and radiographic appearance. A major reason to always do bilateral femoral surgery is to prevent recurrent hip subluxation and improve symmetry. We had no subsequent hip dislocations or subluxations (MP > 30%), and we improved symmetry in the asymmetric patients, although six patients did have asymmetric hip abduction (mean value of 24° (20° to 30°)). Asymmetric hip abduction preoperatively was present in 28% (18 patients); this improved to 9% (six patients) on postoperative follow-up. Five of these six patients were initially in the group with symmetric hip abduction; therefore, it is important to continue to monitor these patients through the growth period because some may develop asymmetry in adolescence.
A limitation of this retrospective review is that we have no patient- or caretaker-reported outcomes to document comfort or functional improvement. It was also not possible to compare bilateral versus unilateral surgeries because there were no unilateral cases.
Conclusion
Asymmetrical dysplastic hips undergoing bilateral surgery in patients with CP have improved symmetry in MP and hip abduction on follow-up. By focusing on correcting the hip dysplasia and improving asymmetry of hip abduction, most hips will remain reduced with symmetric hip abduction at 4.5-year follow-up.
Footnotes
TS: Data acquisition, Analysis and interpretation of data, Final approval of the manuscript.
KJR: Design, Data acquisition, Analysis and interpretation of data, Drafting and critical revision of the manuscript, Final approval of the manuscript.
JPS: Design, Data acquisition, Final approval of the manuscript.
FM: Design, Data acquisition, Analysis and interpretation of data, Drafting and critical revision of the manuscript, Final approval of the manuscript.
MWS: Design, Data acquisition, Analysis and interpretation of data, Drafting and critical revision of the manuscript, Final approval of the manuscript.