
Abstract
Abstract
Purpose
The aim of this study is to report the safety and eff-cacy of soft-tissue surgery incorporating split transfer of tibi-alis anterior to peroneus brevis (SPLATT-PB) for children with hemiplegic spastic equinovarus.
Methods
This was a retrospective case series of children and adolescents with spastic hemiplegia who had a novel combination of SPLATT-TB, intramuscular tenotomy of tibialis posterior and either spasticity management or gastrocsole-us lengthening as the index surgery. The principal outcome measures were changes in pain and difficulty with shoe wear and radiological parameters obtained from weight-bearing anteroposterior and lateral radiographs of the affected foot before and after surgery.
Results
A total of 63 patients with symptomatic spastic equinovarus met the inclusion criteria. Mean age at surgery was 9.8 years (6 to 18) and the mean follow-up was seven years (range 3 to 10 years). Foot pain and problems with shoe wear improved after surgery. Seven radiological criteria showed a clinically and statistically significant improvement at follow-up, the majority being in the normal range. There were 11 surgical adverse events, all classified as Modified Cla-vien-Dindo Grade II. Three patients required further surgery for recurrent equinus, eight patients required further surgery for valgus deformities and four patients required bony surgery for residual varus deformities.
Conclusion
Soft-tissue surgery for spastic equinovarus was successful in the majority of children with spastic hemiplegia, particularly between ages eight and 12 years, resulting in a plantigrade, flexible foot with minimal pain or limitations in shoe-wear. Children younger than 8 years at index surgery were more prone to overcorrection into valgus. Children older than 12 years had persistent varus deformities requiring bony surgery.
Level of evidence
Level IV, retrospective case series
Keywords
Introduction
Equinovarus affects about one-third of children with spastic hemiplegic cerebral palsy (CP).1,2 It is the second most common deformity of the foot and ankle in this group, closely following equinus.1–3 The varus component is considered to be the result of muscle imbalance between the inverters and evertors of the foot and ankle.1,2 More specifically, tibialis anterior (TA) and tibialis posterior (TP) overpower the peroneal muscles.4–6
In a study of gait compensations caused by foot deformity in hemiplegia, Stebbins et al 7 reported that the majority of patients required a combination of gastrocso-leus lengthening (GSL) lengthening of TP and split transfer of TA (SPLATT). This suggests that in hemiplegia the overactivity of the TP and TA is the dominant pattern.1,2,5–7 In a long-term follow-up study of soft-tissue surgery for equinovarus deformity in children with CP, Chang et al 2 reported that children with spastic hemiplegia had the most predictable results but that both over-correction and under-correction were prevalent at long-term follow-up.
The choice of soft-tissue surgical procedures for equinovarus deformity in CP is extensive and includes lengthening of the gastrocsoleus and TP, as well as split transfers of TP (SPOTT) and SPLATT.1,2,6–8
Descriptions of the surgical technique for SPLATT include transfer of the lateral half of the split tendon to a bony tunnel in either the cuboid or the base of the fifth metatarsal.9, 10 Tendon to bone may require suturing over a plantar button or felt pad and may result in skin ulceration, plantar sensitivity and failure of the tendon transfer. Other techniques include the use of interference screws or a suture anchor.11,12
The peroneus brevis (PB) is a widely recognized recipient for transfer for TP for SPOTT procedures but there are few reports of PB being used as a recipient for SPLATT.5,8,13 We considered that the PB would be a good recipient due to its anatomical consistency in both substance and length providing reliable tendon to tendon healing. The lateral insertion of PB also provides a large moment arm. Given that the lateral half of tibialis anterior was transferred to PB during SPLATT, we considered that SPOTT was not indicated and we selected intramuscular tenotomy of Tibialis Posterior (IMT-TP), as described by Ruda and Frost, with SPLATT to reduce muscle imbalance between the inver-tors and evertors. 14 The aim of this study is to report the safety and efficacy of soft-tissue surgery, incorporating split transfer of TA to PB (SPLATT-PB), for children with hemiplegic spastic equinovarus.
Patients and methods
Inclusion criteria
Children with spastic hemiplegia who were registered on the Statewide Cerebral Palsy Register, who had soft-tissue surgery, as described above, between 1995 and 2015 at the Royal Children's Hospital, Melbourne were included. Equinovarus deformity was recognized by the typical clinical appearance, confirmed by physical examination and weight-bearing radiographs of both feet. Children were excluded if they did not have > 36 months clinical and radiographic follow-up.
Patients
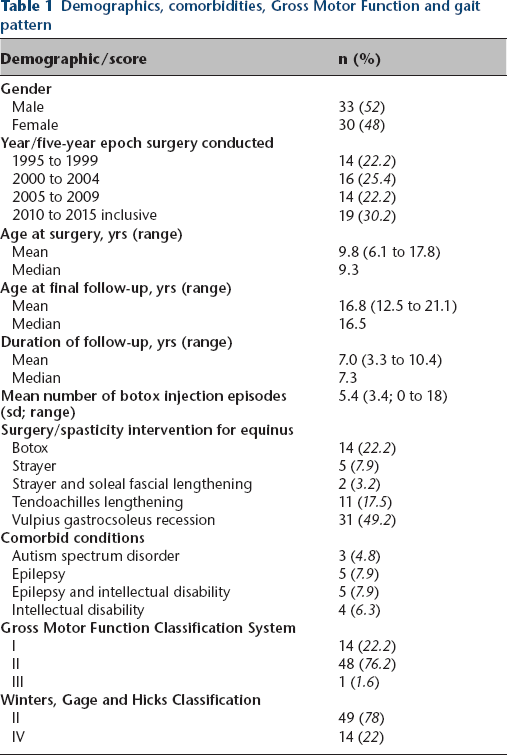
A total of 63 patients fulfilled the inclusion criteria (Fig. 1). Demographics and comorbidities are summarized in Table 1. Patients were followed every three months for the first year after surgery and every one to two years until transition to adult-care facilities between the ages of 16 and 20 years.
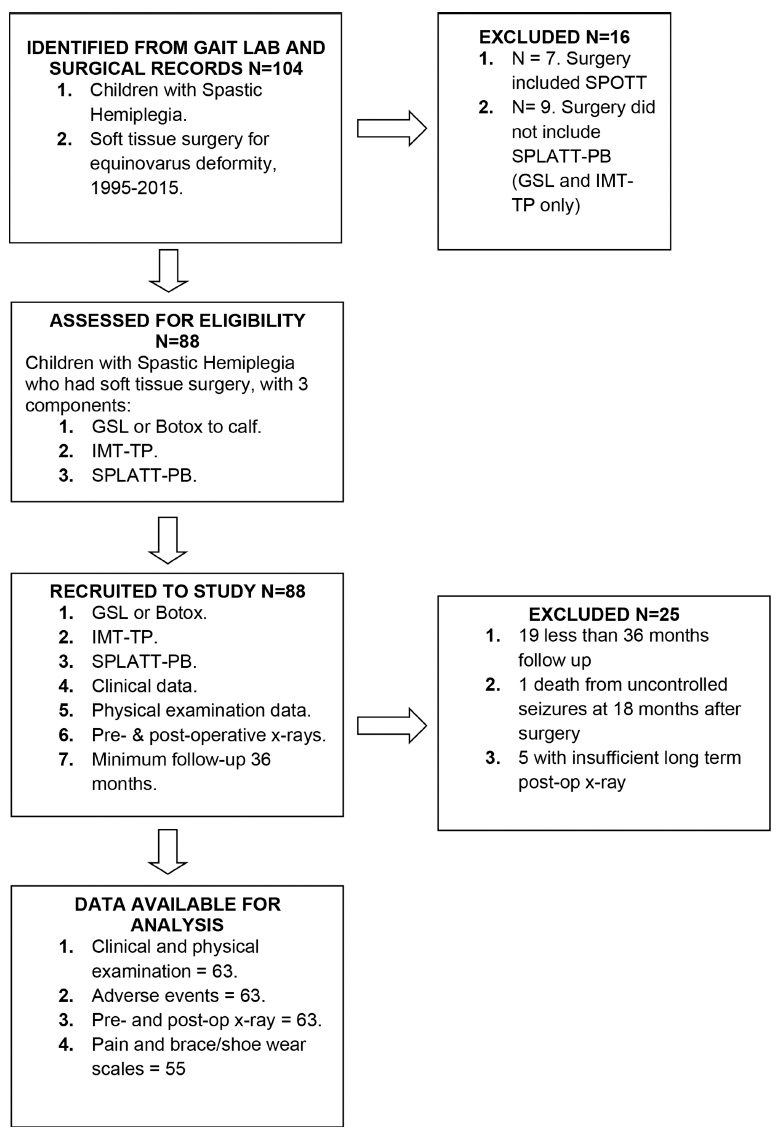
Flow diagram summarizing patient numbers, surgical exposure and follow-up in accordance with Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) (SPLATT-PB, split transfer of tibialis anterior to peroneus brevis; SPOTT, split posterior tibialis transfer; GSL, gastrocsoleus lengthening; IMT-PL, intramuscular tibialis posterior lengthening. 14
Demographics, comorbidities, Gross Motor Function and gait pattern
Measures
Operative notes and surgical records were reviewed to determine age at surgery, the type of surgery performed and length of follow-up. Preoperative data and latest available postoperative data or data prior to revision surgery were used.
Symptoms related to pain and difficulties with brace or shoe-wear were assessed using a nine-point Likert Scale, with 0 indicating no pain or no difficulties with shoe-wear or brace-wear and 9 indicating either severe pain or being unable to use a brace or regular shoes (see Appendix 1).
Radiological parameters were measured from digital radiographs using the Patient Archive Communication System (PACS, Fujifilm Medical System USA, Lexington, Massachusetts, United States) and associated online tools. The radiographic criteria were chosen to permit assessment of the hind foot, midfoot and forefoot. The measures were: hindfoot: tibiocalcaneal angle and lateral tibiocalcaneal angle; midfoot: navicular cuboid overlap and talonavicular coverage angle; forefoot: lateral talo-1st metatarsal angle, anteroposterior talo-1st metatarsal angle and the metatarsal stacking angle. All angles were measured by two observers (AK, HKG) using tools on the PACS and all radiographic measures were performed as described by Davids et al. 15 These have been shown to be reliable and have convergent validity with pedobarography. 16 Adverse events were classified using the Clavien-Dindo system, modified for children with CP. 17
Indications and surgical techniques
To qualify for surgery, a consistent equinovarus deformity was present, refractory to injections of botulinum toxin and serial casting. Varus of the hindfoot and adduction/ supination of the forefoot were present throughout stance and swing phases of gait on both clinical examination and video recording of gait using slow motion playback.1,2,5,18 TP was examined in the ‘Figure 4’ position using a fast stretch into eversion for spasticity and a slow stretch for contracture.3, 19 Gastrocsoleus length was examined using the Silfiverskiöld test.1,2,19
Botulinum toxin A (BoNT-A) was used for gastrocsoleus spasticity without contracture, defined as the presence of a spastic catch combined with ankle dorsiflexion > 10° after intramuscular tenotomy of TP (IMT-TP). 19 For a gas-trocsoleus contracture of 0° to 20° a Strayer distal gastrocnemius recession was performed with additional soleal fascial lengthening (SFL) as required. For a contracture > 20° a modified Vulpius gastrocsoleus recession (GSR) was performed. 20 For equinus > 30° a White slide lengthening of the Achilles tendon was used (see Appendix 2 for descriptions and illustration). 3 The goal of surgery for equinus was dorsiflexion of 10°, to allow the SPLATT-PB to work effectively. IMT-TP was performed from a medial incision, with an attempt to titrate the amount of lengthening to the severity of the clinical and radiographic deformity (Fig. 2).14,21
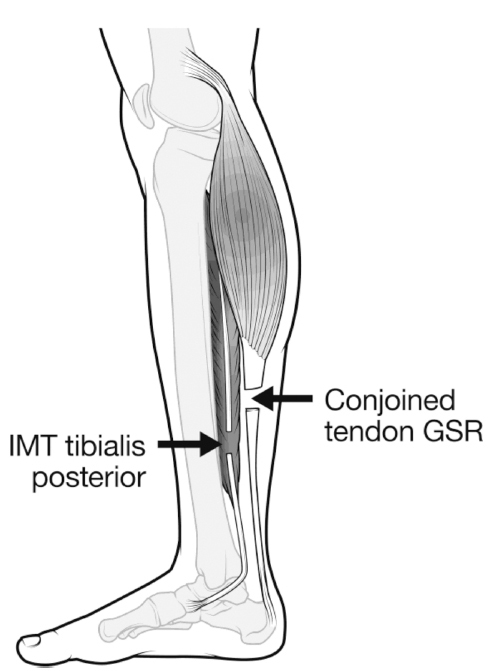
Intramuscular tenotomy (IMT) of tibialis posterior was performed in the distal third of the leg and the most common surgery for equinus in this cohort was a modified vulpius gastrocsoleus recession in Zone 2. These two procedures were performed through a single posteromedial incision, with retraction anteriorly to reach tibialis posterior, followed by retraction posteriorly to reach the conjoined tendon of the gastrocsoleus.
SPLATT was prepared in a standardized fashion using a three-incision technique.5,6 The lateral half of the SPLATT was attached to the anterior two-thirds of the PB, by direct side-to-side suture in all patients (Fig. 3). Postoperative care and rehabilitation are described in more detail, in Appendix 2.
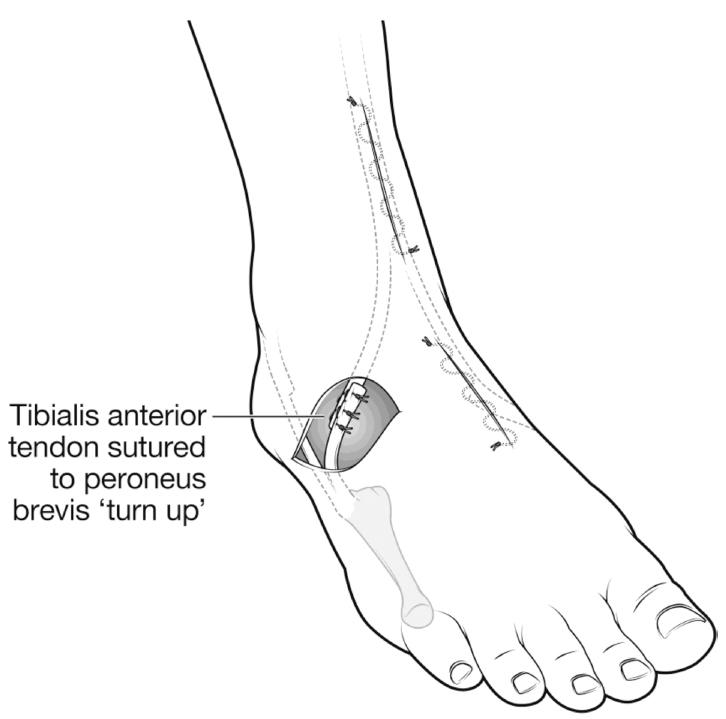
After intramuscular tenotomy of tibialis posterior and gastrocsoleus recession, split transfer of tibialis anterior to peroneus brevis was performed through three incisions as shown. The lateral half of tibialis anterior was mobilised and secured with a Bunnell suture and passed under the intact skin bridge, to be sutured to the anterior two-thirds of the peroneus brevis. NB: all skin incisions are closed prior to suturing tibialis anterior to peroneus brevis, under tension.
Patients were followed every 12 to 24 months in a dedicated outpatient setting with review in the gait laboratory as required. Additional and bony surgery was utilized when recurrent or new deformities arose. Indications for bony surgery for both varus and valgus deformities followed accepted recommendations from the literature.1, 13 Given that radiographic assessment was the primary outcome measure, the seven chosen radiographic parameters were compared from radiographs before the index surgery and at the last available assessment, prior to transition or prior to bony surgery in the sub-set of patients who required these procedures. See Figures 4 to 6 for examples.

Ten-year-old boy with severe equinovarus deformity right foot. Pain was graded as 4, difficulties with shoes, shoe wear/braces as 5. Surgery consisted of White slide lengthening of the Achilles tendon and intramuscular tenotomy of tibialis posterior and split transfer of tibialis anterior to peroneus brevis. He achieved a plantigrade foot and no additional surgery was required.

Right hemiplegia in a six-year-old girl. The varus of the hindfoot and supination of the forefoot are extreme but there was no fixed equinus. Despite the young age, surgery was indicated because of pain (4 on the Likert Scale) and difficulties with shoes (6 on the Likert Scale) and consisted of injections of BoNT-A to the gastrocsoleus, intramuscular tenotomy of tibialis posterior and split transfer of tibialis anterior to peroneus brevis.

This is the ten-year follow-up, of the patient in Figure 5. The right foot was pain-free, and flexible at ten-year follow-up. Clinically there was mild heel valgus and the radiographic analysis showed both a correction in to valgus on several of the indices. An internal rotation, supramalleolar osteotomy for external tibial torsion was performed, five years after the index soft-tissue surgery.
Statistical analysis
Data was examined to determine if the data deviated substantially from a normal distribution. For all statistical tests comparing pre- and post-measures we report the difference and the 95% confidence interval to address the uncertainty of the estimate, p values are also reported.
Preoperative and postoperative pain and function scores were compared using the paired t-test. There were 12 cases with missing data on either pre- or postoperative data for the pain measure and 13 for the shoe wearing difficulty measure. These cases were omitted from this analysis.
Preoperative and postoperative angles were compared using the paired t-test. The normal range for the seven radiographic outcome measures are from Davids et al. 15 See as examples Figures 7 to 9.

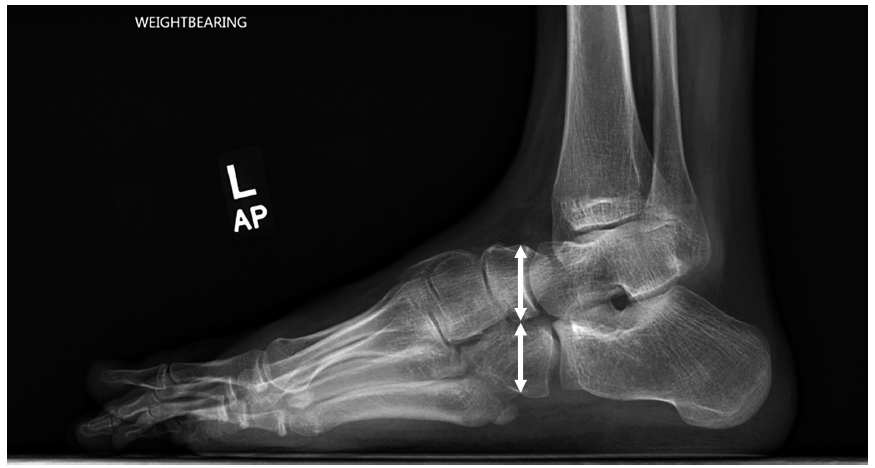
Standing lateral radiograph of an equinovarus left foot, showing the tibiocalcaneal angle which was utilized as the radiographic measure for equinus.
The adverse events and/or additional surgery numbers are reported as raw data and as a proportion of the sample.
All the analysis was performed with Stata 16.1 (Stata Corp, College Station, Texas, US).
Results
Demographics, comorbidities gross motor function and gait patterns are described in Table 1.22,23 A total of 19 patients were excluded for follow-up because they had between 12 and 36 months follow-up. All patients had IMT-TP and SPLATT-PB. In addition, 14 patients had injections of toxin ABoNT to the gastrocsoleus; five had Strayer, two had Strayer with SFL, 31 had GSR and 11 had a White slide lengthening of the Achilles tendon. 5 A total of 11 patients with Winters, Gage and Hicks Classification 22 Type IV hemiplegia had an external rotation osteotomy of the proximal femur, following the indications described by Rodda et al 23 and the technique described by Dobson et al. 24
Pain and function
The change in pain scores as measured by the Likert scale, on mean shifted by one unit (95% confidence interval (CI) 0.5 to 1.4; p < 0.001) from 2.7(SD=1.3)to 1.7(SD=0.9). For shoe wearing difficulty the mean difference between pre-and post-scores was 2.5 (95% CI 2.1 to 2.9; p < 0.001; pre-score 4.2 (SD=1.3), post-score 1.7(SD=0.9). The changes on both measures are considered clinically important.
Radiographic outcomes
The mean pre- and post-values for the seven radiographic measures are compared with previously published normal data in Table 2. The mean preoperative values differ substantially compared with normal. There is an overall trend towards normal for postoperative means with a tendency toward mild overcorrection into valgus.15, 16
Comparison of normal, preoperative and final postoperative radiographic measurements
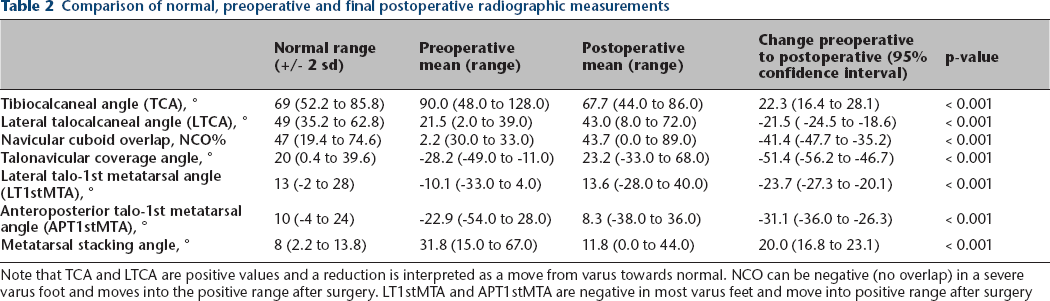
Note that TCA and LTCA are positive values and a reduction is interpreted as a move from varus towards normal. NCO can be negative (no overlap) in a severe varus foot and moves into the positive range after surgery. LT1stMTA and APT1stMTA are negative in most varus feet and move into positive range after surgery
Surgical adverse events
In total, 11 (17.4%) patients had a surgical or medical adverse event. Three patients had a superficial infection related to a suture. Four patients had superficial cast sores, two had pain and spasm after surgery which was poorly controlled with analgesia and one patient had severe constipation which prolonged their inpatient stay. One patient had a urinary tract infection. All adverse events were Grade II according to the Modified Clavien-Dindo System. 17
The SPLATT-PB was intact and functional according to clinical examination in all patients according to a standardized examination protocol which included a ‘confusion test’. 19 There were no dehiscences or ruptures of the tendon transfer recorded.
Further surgery
Those in the oldest age group > 12 years, were more likely to have under-correction, with the talonavicular coverage angle moving towards but not into the normal range (Fig. 10). In this age group 4/10 (40%) required additional surgery all due to persistent varus. This was predicted from preoperative evaluation of stiffness and the severity of radiographic deformity. Bony surgery was planned at 12 months after soft-tissue balancing.13,25 For the patients aged 10 to 12 years, 3/18 (17%) patients required additional surgery. From eight- to ten-year-old patients, 3/17 (18%) had further surgery. In the youngest group aged six to eight years, 5/18 (28%) had further surgery all due to over-correction into valgus and/or external tibial torsion, uncovered by the correction of equinovarus.24,26 In total, 15 patients (24%) needed additional surgery and this was performed at a mean of 3.5 years (1.1 to 6.4) after the initial surgery. The procedures and the timing are described in Table 3.
Further surgery
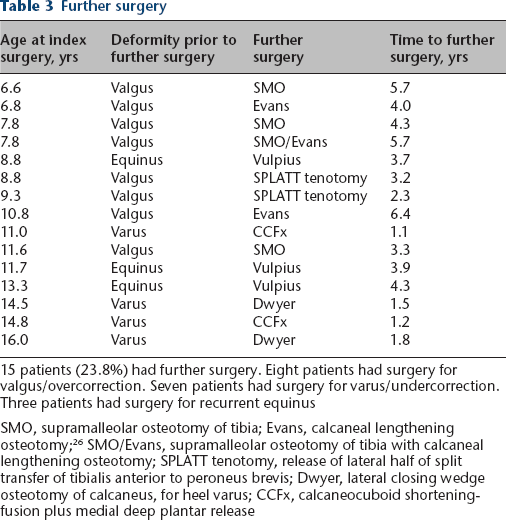
15 patients (23.8%) had further surgery. Eight patients had surgery for valgus/overcorrection. Seven patients had surgery for varus/undercorrection. Three patients had surgery for recurrent equinus
SMO, supramalleolar osteotomy of tibia; Evans, calcaneal lengthening osteotomy; 26 SMO/Evans, supramalleolar osteotomy of tibia with calcaneal lengthening osteotomy; SPLATT tenotomy, release of lateral half of split transfer of tibialis anterior to peroneus brevis; Dwyer, lateral closing wedge osteotomy of calcaneus, for heel varus; CCFx, calcaneocuboid shortening-fusion plus medial deep plantar release
Discussion
We limited our report to children with spastic hemiplegia to have a more homogenous study. Our inclusion criteria with respect to index surgery are also restrictive, with all patients having intramuscular lengthening of TP, SPLATT-PB and either spasticity management or lengthening of the gastrocsoleus.3,5,12–14
Soft-tissue surgery for equinovarus deformity in children with spastic hemiplegia is accepted as the first line surgical approach but the number of procedures, and the combinations used, are variable.1–9 Deformities are usually flexible in younger children and little pain may be reported, as in this study.1,2 With time, deformities become stiffer, more fixed and more symptomatic as the tarsal bones change in shape under the deforming forces. Determining the relative contributions of TA and TP to the combined deformity is challenging although combinations of clinical examination, slow motion video analysis, dynamic electromyography, pedobarography and the use of a multisegmental foot model kinematic analysis all make useful contributions to a fuller understanding of the deformity and the impact on gait and function.1–8 A combination of patient-reported outcomes (PROMs) and standardized radiology was considered to be more reliable and valid than older, but commonly used clinical scoring systems, such as those described by Kling et al. 27 Radiographic criteria that we have used have been found to correlate well with pedobarographic findings. 16 Given the widespread attachment of TP in the midfoot and because of the phenomenon of ‘segmental linking’ it is likely that deforming effects of TA and TP overlap with effects on the hindfoot, midfoot and forefoot.15, 16 Not all children in this study had access to these investigations and surgical decisions were made on the basis of a detailed clinical examination, video recording of gait and weight-bearing radiographs.1–5,6–9,15,16
SPLATT-PB is a simple, safe and effective procedure, in combination with IMT-TP and GSL.3,5,9,14 SPLATT-PB is effective because the PB has an excellent moment arm for the correction of both plantar flexion, inversion and forefoot adduction. It is effective in relieving symptoms of pain and difficulties with shoe-wear and brace-wear. It improves the morphology of the foot, particularly in younger children, as seen in our results using radiological criteria for hind-foot, midfoot and forefoot (Figs 5 and 6, Table 2).
Soft-tissue surgery in the management of spasticity in a growing child has known limitations in that a significant number of children require further surgery.1, 2 There were no failures of SPLATT-PB that required early revision surgery. Two patients had a percutaneous release of the lateral arm of the SPLATT because of persistent overactivity, with progressive pes valgus (Table 3).
On balance, the radiographic parameters have suggested a shift towards a mild valgus alignment and it is possible that this surgical approach, particularly in younger children, is too large a ‘surgical dose’ (Figs 5, 6 and 10). Mild valgus is better tolerated in the long term than varus in terms of pain, degenerative change and problems with ankle instability and foot-wear.1,2 For the younger patient with overcorrection, further surgery was effective. Our subjective opinion was that this was mostly related to TP insufficiency rather than overactivity in the SPLATT-PB.
In older children, we performed the same index surgery to balance forces on the foot. We agree with Dreher et al 25 that soft-tissue balancing is essential either before or with bony surgery when there is fixed deformity. 18 We staged our surgical approach in the older children as we felt it would be safer and we were unsure how much correction the soft-tissue surgery would achieve. Surgery was effective in arresting progression of the deformity but did not reverse the bony deformity already present, which was managed later (Fig. 8). 25 The delay in the older patients accessing surgery was related to delayed referral to our service with repeated and prolonged cycles of injections of BoNT-A, a significant contributor. 19
Standing lateral radiograph of the foot, in an 18-year-old boy, six years after soft-tissue surgery for spastic equinovarus. The sinus tarsi is open, and all the radiographic indices were in the varus alignment range. Note the lack of any overlap of the navicular on the cuboid, indicating a cavovarus foot with no correction of the midfoot or forefoot. Because of the residual varus, an oblique view of the ankle seen. This patient went on to bony surgery for correction of symptomatic cavovarus.
Follow-up < 36 months can be misleading as few patients will show recurrent varus or overcorrection to valgus. 4 Between 12 and 36 months follow-up in some children lapsed. The majority were known at 12-month follow-up to be functioning highly. They had given up the use of orthotics and their parents were reluctant to bring them back for repeat clinical or radiographic evaluations. Using a state-wide CP register, we confirmed that no children had been registered as having revision surgery in the 19 patients who had short-term follow-up. These children may have had better outcomes than the main cohort who were followed for a longer period.
Most studies of spastic equinovarus in hemiplegia have reported small numbers, with short-term follow-up and some lack either a PROM or objective criteria of foot morphology. In this study we included radiographic criteria which can assess the static morphology of the hindfoot, midfoot and forefoot (Figs 7 to 9). These criteria described by Davids et al 15 have been shown to have convergent validity with dynamic pedobarography by Lee et al. 16 It is reassuring to know that these criteria which are easily available, are useful both for surgical planning and as outcome measures.1,2,13,15,16,25

Standing anteroposterior radiograph of both feet, in a ten-year-old girl, before surgery. The landmarks for measuring the talo-navicular-coverage angle are indicated. On the left side, the value is positive indicating mild abduction of the forefoot. On the right/ spastic equinovarus side, the angle is negative, indicating marked abduction of the forefoot. The marked difference in anteroposterior talo 1st metatarsal angle is also obvious but not marked with arrows, in the interest of clarity.
We were surprised by the low levels of pain reported in our series despite the severity of the deformity.1, 2 Patients and parents reported greater difficulty wearing off the shelf shoes than pain, before surgery. Both outcomes improved after surgery, with the notable exception of the teenagers with stiff, under-corrected feet.
Our data suggests that there is an optimum age for this combined surgical soft-tissue approach. There is a higher risk of valgus deformity if surgery is performed under the age of eight years (Fig. 10).1,2 However, surgeons and patients may be faced with little option when the deformity is severe and symptomatic in the younger child. The six-year-old girl, illustrated in Figure 5, is one example. Given that no surgical trials have been published, we lack evidence to make alternative recommendations. SPOTT might be preferable in the younger child or an isolated lengthening of TP.1, 2, 11,14
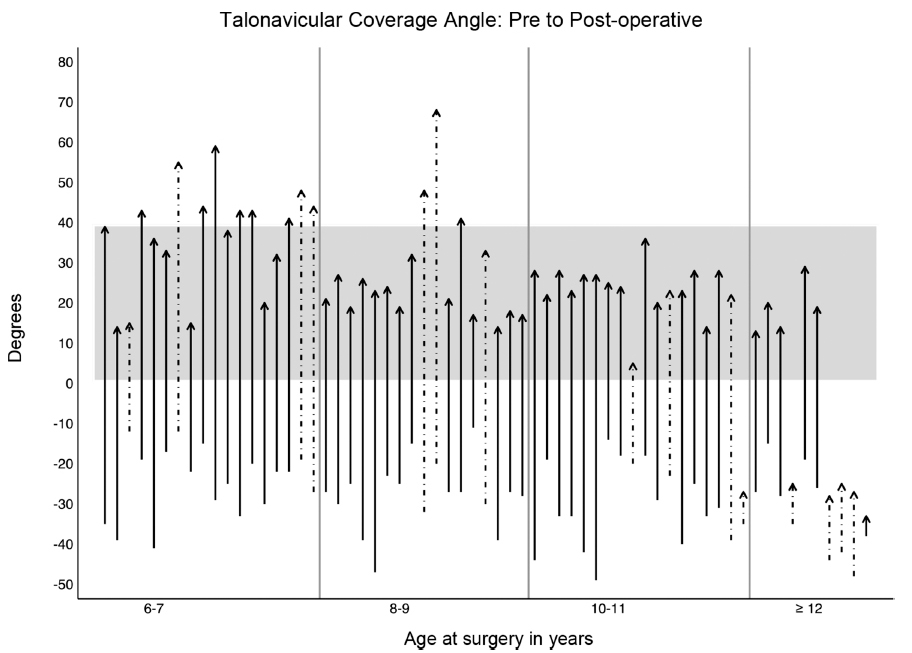
Each arrow shows an individual subjects’ talonavicular coverage angle. They are ordered by age increasing from left to right. The start of the arrow represents the preoperative angle and the arrowhead represents postoperative angle. The grey band shows normal values to two standard deviations. All subjects start outside of this normal range. A number of younger patients ‘overshoot’ into the valgus range. A number of older patients remain uncorrected in the varus range. A dotted line indicates that this subject had further surgery.
The strengths of our study included a relatively uniform approach to surgical prescription, dose-based surgery for GSL, medium-term follow-up and a combination of patient-reported and objective radiological outcome measures. Study limitations include lack of a validated PROMS such as the Oxford Foot and Ankle Scale, and investigations such as a segmental foot model for motion analysis, pedobarography and dynamic electromyogra-phy EMG.1,2,5–7,28 These have been added over the time this data was obtained.
A potential confounder was the utilization of an external rotation osteotomy of the femur in children with Type IV hemiplegia. 23 When the lateral border of the foot is inside the line of progression, ‘rollover varus’ may compound spastic equinovarus. 23 Correction of this proximal rotational deformity seems logical and supported by previous studies.23,24
Many of the outstanding questions regarding optimum surgical management of spastic equinovarus in children with hemiplegia may require randomized surgical trials. This study may be useful to inform trial protocols because of the findings of the utility of weight-bearing radiographs, the relationship between age and varus-valgus outcomes and confirmation of the length of follow-up required for the development of symptomatic valgus over-correction.2,4,26
Footnotes
SF: Study conception and design, Drafting of the article, Critical revision of the article for intellectual content, Final approval of the article.
CG: Study conception and design, Drafting of the article, Critical revision of the article for intellectual content, Final approval of the article.
KF: Statistical analysis, Interpretation, Drafting of the article, Critical revision of the article for intellectual content, Final approval of the article. AK: Study conception and design, Drafting of the article, Critical revision of the article for intellectual content, Final approval of the article.
ER: Study conception and design, Drafting of the article, Critical revision of the article for intellectual content, Final approval of the article.
HKG: Design of the split transfer of tibialis anterior to peroneus brevis concept, Study conception and design, Drafting of the article, Critical revision of the article for intellectual content, Final approval of the article.