
Abstract
Purpose
Tarsal coalitions are congenital fusions of two or more tarsal bones and can lead to foot pain and stiffness. Few studies examine the long-term reoperation rates following paediatric tarsal coalition surgery.
Methods
A population-based database, linking medical records at all medical centres to capture the entire medical history of the full population of a Midwest county, was used to identify tarsal coalitions in children between 1966 and 2018. Records were reviewed for clinical data, surgical records and followed up to identify any subsequent surgical interventions.
Results
A total of 58 patients (85 coalitions) were identified; 46 calcaneonavicular (CN) coalitions, 30 talocalcaneal (TC) coalitions and nine other coalitions (seven talonavicular, one naviculocuboid, one naviculocuneiform). In all, 46 coalitions were treated surgically (43 coalition resections, three arthrodeses) and 39 were treated nonoperatively. Patients treated surgically were less likely to report ongoing symptoms at final follow-up compared with patients managed nonoperatively (33% versus 67%; p = 0.0017). With a median 14.4 years (interquartile range 9.3 to 19.7) follow-up, there was an overall re-operation rate of 8.7% (4/46). Differences in reoperation rates by initial surgery (resection versus arthrodesis; p = 0.2936), coalition type (CN versus TC versus Other; p = 0.6487) or composition (osseous versus fibrocartilaginous; p = 0.29) did not reach statistical significance.
Conclusion
This is the first population-based study demonstrating the durability of surgical management of tarsal coalitions in a paediatric population. At final follow-up, patients treated surgically are less likely to report persistent symptoms compared with patients managed nonoperatively. Long-term reoperation rates appear to be low (8.7%).
Level of evidence
III
Introduction
Tarsal coalitions represent abnormal fibrous, cartilaginous or bony fusions between two or more tarsal bones. 1 Patients may present with foot pain, external foot progression angle or recurrent ankle sprains. 2 Conservative measures such as activity modification, non-steroidal anti-inflammatory medications, orthotics and a period of immobilization are often the first line of treatment.1,2 Surgery may become necessary and is considered for patients who have failed these conservative measures.3,4
Common surgical approaches include resection of the coalition with or without interposition of material, corrective osteotomy, arthrodesis or a combination of these strategies.1,2 These treatments have been shown to provide excellent functional outcomes and symptom relief.5–9 However, much of this data is regarding short- to intermediate-term follow-up.3,9,10 Scranton 3 reported good results in 13 of 14 feet treated with resection with no reoperations at an average of 3.9 years follow-up for talocalcaneal (TC) resection. Mubarak et al 10 reported on calcaneonavicular (CN) coalitions and noted that 5% of patients required repeat resection for recurrence or inadequate resection and an additional 9% of patients underwent subsequent osteotomy to improve persistent malalignment of the foot in patients with minimum one-year follow-up. Khoshbin et al 11 report on the results of tarsal coalitions in over 300 patients in a population-based study and found a 14% reoperation rate at an average nine years follow-up. However, this study was largely in an adult population (average age 24.2 years (sd 17.5)) and patients lost to follow-up tended to be paediatric patients (average age 15.9 years (sd 5.3)).
In the literature there has been a paucity of data on the long-term results of surgical treatment for tarsal coalitions and few reports on reoperation rates following surgical interventions in paediatric populations. Thus, the purpose of our study was to utilize a population-based study design to evaluate the patient characteristics and long-term reoperation rates following surgical intervention for paediatric tarsal coalitions.
Materials and methods
Following institutional review board approval, a population-based database derived from census and electronic medical records was used to identify all county residents assigned a diagnosis code consistent with a tarsal coalition between 01 January 1966 and 31 December 2018. This population-based database provides a medical records linkage system encompassing the full medical record of the county population since 1966. 12 Prior studies have found this database to provide reasonable estimates of the incidence of various medical conditions with good generalizability relative to the United States population.12–14 This database represents a collaboration of clinics, hospitals systems, private practices and a large academic referral centre, all treating patients within the county of interest. All surgical procedures were performed at the academic referral centre by orthopaedic surgeons with either paediatric or foot and ankle sub-specialization.
In order to capture all patients, multiple diagnostic codes and coding systems were utilized due to the long study period (see Supplementary Material). Some of these diagnostic codes were quite broad and included many paediatric foot conditions other than tarsal coalitions (e.g. congenital talipes equinovarus, accessory navicular, hallux valgus etc) and were excluded as ‘alternate diagnoses’ (Fig. 1). Only county residents with an idiopathic tarsal coalition who were 18 years or younger at the time of diagnosis were included. Patients with conditions which may affect the lower limbs (such as cerebral palsy, myelomeningocele or other congenital anomalies of the lower extremity) were excluded. Patients who were not county residents or who had treatment prior to residing in the county were also excluded from the study. Only patients with a confirmed tarsal coalition, either radiographically or intraoperatively, were included. Patients with less than two years follow-up were also excluded from the study as shorter follow-up may affect estimates of reoperation rates (Fig. 1).
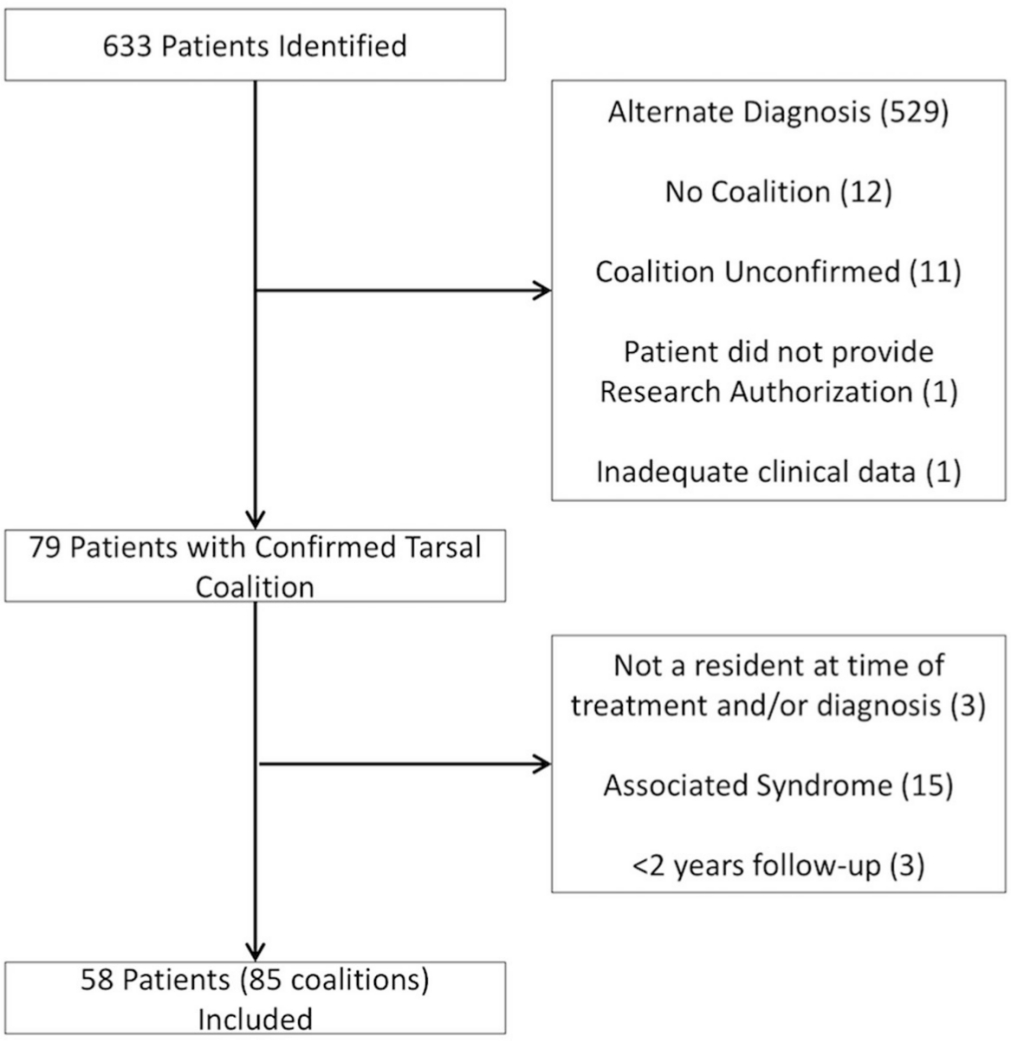
Overview of patient inclusion and exclusions.
Statistical analysis
Standard descriptive summaries (e.g. mean and sd for continuous variables such as age and percentage for categorical variables such as gender) were used to summarize demographic variables. Comparisons of categorical variables between subgroups were made using the chi-squared test or Fisher's exact test, depending on the size of the sample. Comparisons of continuous variables were completed using independent t-tests or analysis of variance for comparisons between three groups. Kaplan-Meier survival curves were constructed for the patients who required revision surgery. Alpha was set at a significance level of p < 0.05. Statistical analysis was performed using JMP software (Version 14.1.0.; SAS Institute Inc., Cary, North Carolina).
Results
Population
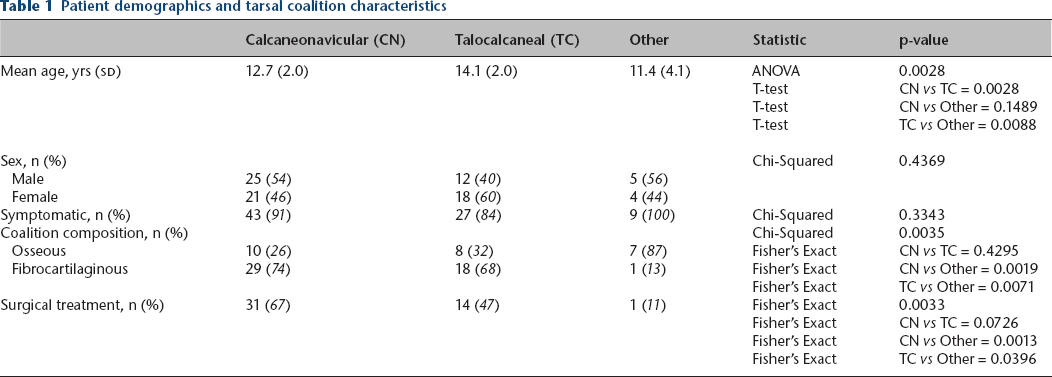
Between 1966 and 2018 there were 85 coalitions identified in 58 paediatric county residents. In all, 79 of these were symptomatic, whilst six were asymptomatic and found incidentally. There were 46 CN coalitions, 30 TC coalitions and nine other coalitions (seven talonavicular, one naviculocuboid, one naviculocuneiform). Patients with TC coalitions tended to present at an older age relative to CN and other coalitions (mean 14.1 ± 2 years versus 12.7 ± 2 years versus 11.4 ± 4.1 years; p = 0.0028). There were also differences in the composition of the coalitions with other coalitions more likely to be osseous rather than fibrocartilaginous relative to CN or TC coalitions (87% versus 26% versus 32%, respectively; p = 0.0035) (Table 1). There was a general trend towards more advanced imaging in the later decades of the study (Fig. 2).
Patient demographics and tarsal coalition characteristics
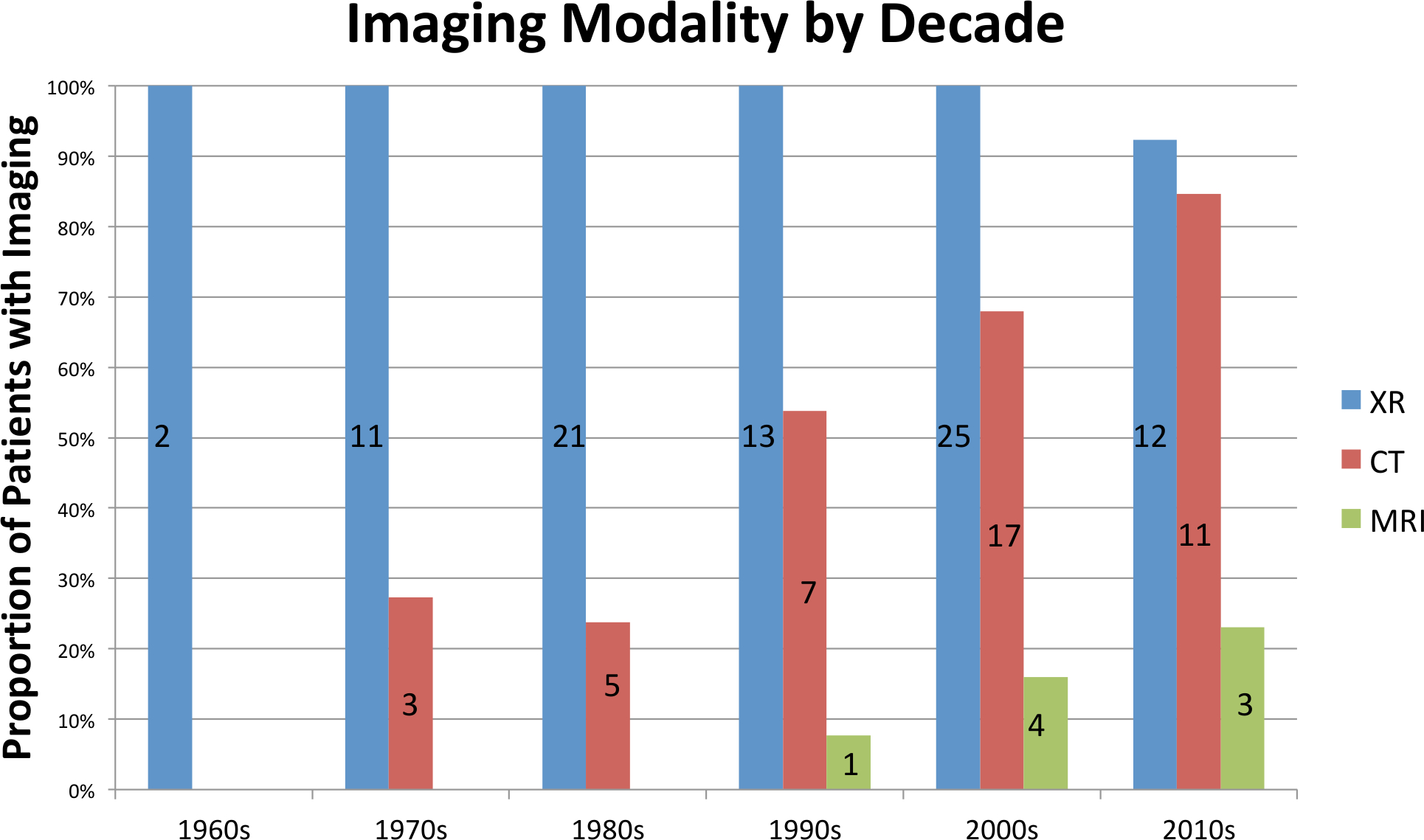
Imaging modality utilization rates per decade. Numbers indicate total number of studies obtained (XR, radiographs).
Surgical data
There were 46 coalitions treated surgically (43 coalition resections, three arthrodeses) and 39 were treated nonoperatively. Other coalitions were less likely to have surgical intervention, compared with CN or TC coalitions (11% versus 67% versus 47%; p = 0033). Patients with CN coalitions tended to be treated sooner after initial presentation compared with TC and other coalitions (mean time to surgery 0.76 ± 1.3 years versus 1.37 ± 1.3 years versus 3.97 years; p = 0.0313). There was not a statistically significant difference between the types of coalitions and whether they were treated with arthrodesis or resection (Table 2). We did not identify a significant difference in patients treated with surgery compared with patients treated nonoperatively in terms of demographic variables. At final follow-up patients treated nonoperatively were more likely to be symptomatic than patients treated surgically (67% versus 33%; p = 0.0017) as defined by patient complaints of persistent pain or stiffness in the foot or ankle (Table 3). There was no significant difference in remaining symptomatic at final follow-up based on composition (osseous versus fibrocartilaginous, 60% versus 48%; p = 0.3255). However, there was a significant difference based on type of coalition, with the other coalitions being more likely to remain symptomatic relative to CN or TC coalitions (78% versus 57% versus 37%; p = 0.0380) (Table 2).
Summary of surgical treatment of paediatric tarsal coalitions
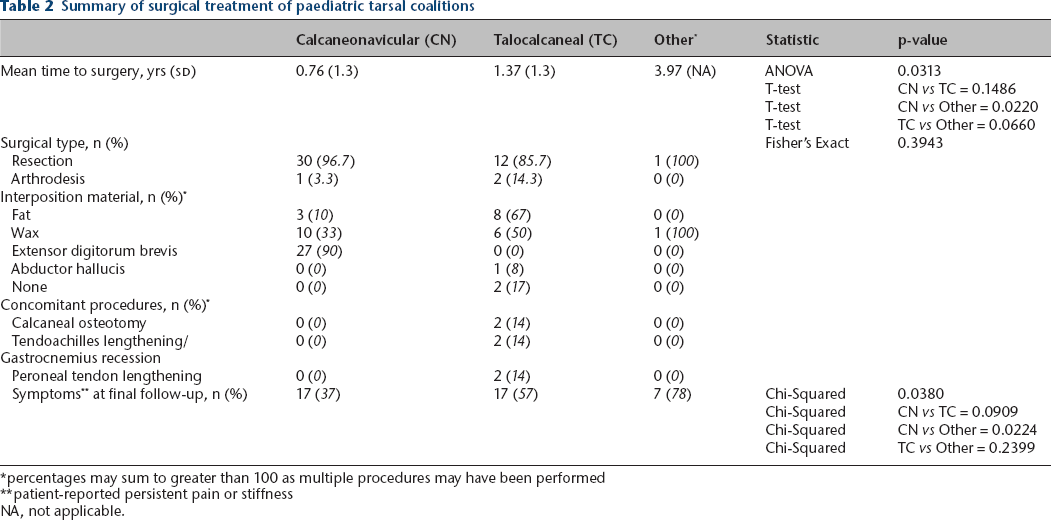
percentages may sum to greater than 100 as multiple procedures may have been performed
patient-reported persistent pain or stiffness
NA, not applicable.
Comparison of patients with or without surgical intervention
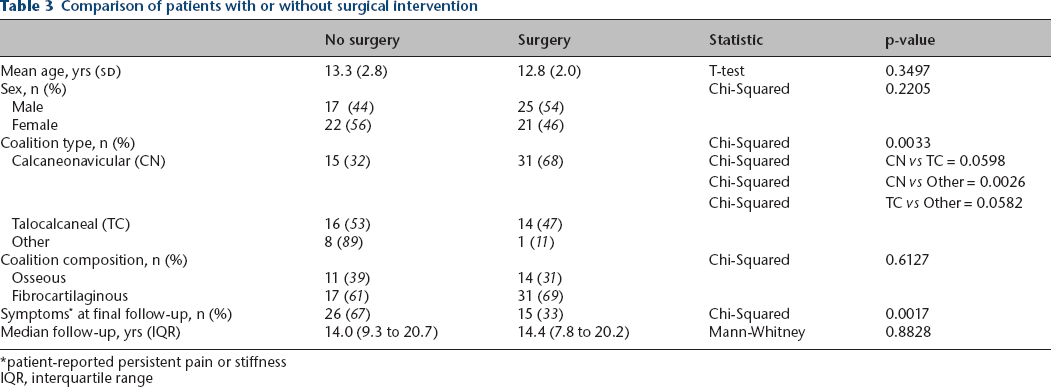
patient-reported persistent pain or stiffness
IQR, interquartile range
Reoperation rates and survival analysis
Patients were followed for a median 14.4 years (interquartile range (IQR) 9.3 to 19.7). There were six reoperations in four patients, representing an overall rate of 8.7% (4/46) for patients requiring at least one repeat operation. The median time to reoperation was 4.00 years (IQR 1.6 to 15.8). Two patients underwent repeat resection and interposition, one patient underwent excision of symptomatic osteophytes near the coalition resection site, and one patient underwent closing wedge osteotomy for persistent hindfoot deformity following primary triple arthrodesis. There was no statistically significant difference in reoperation rates by patient demographics, type of surgery, coalition type or composition (Table 4). Based on Kaplan-Meier analysis, the overall mean time to failure was 18.1 ± 117.8 years. No statistical difference was identified between the types of tarsal coalitions in terms of the overall survivorship (p = 0.6305) (Fig. 3).
Comparison of patients with or without subsequent surgical intervention
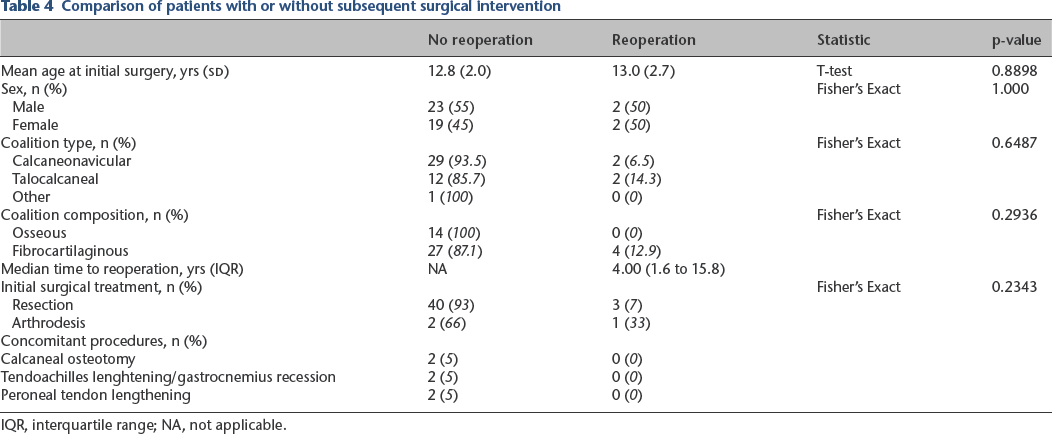
IQR, interquartile range; NA, not applicable.
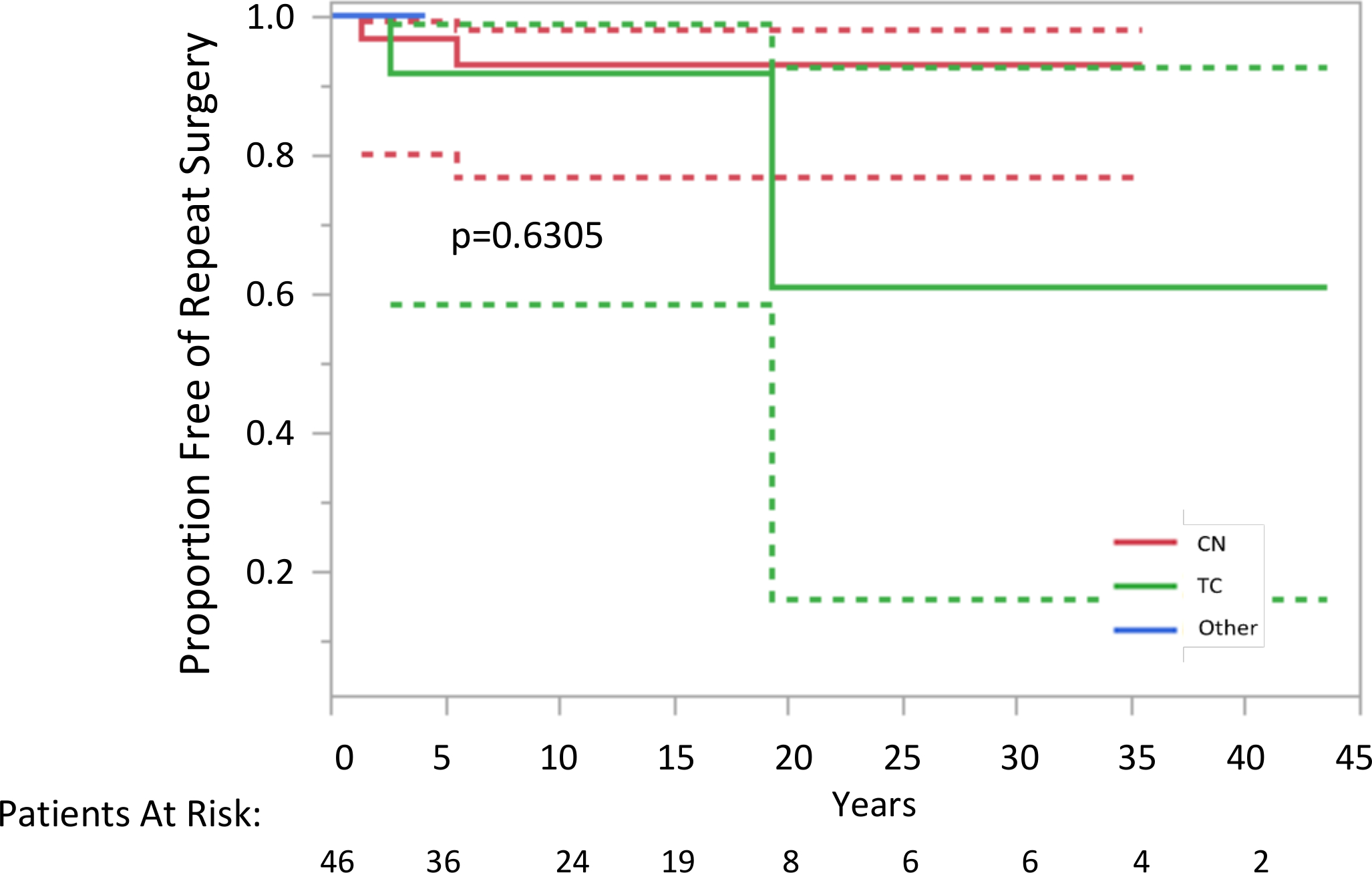
Survivorship analysis for reoperation of paediatric tarsal coalitions (CN, calcaneonavicular; TC, talocalcaneal).
Discussion
At short-term follow-up, surgical management of tarsal coalitions has shown favourable outcomes.6–8 Swiontkowski et al 6 reported overall good results in 40 patients (39 paediatric, one adult) treated with either resection or arthrodesis. They reported an overall reoperation rate of 10.5%. The reoperation rate was 9.1% at an average 4.6 years follow-up in the CN group and 15.4% at an average of 3.1 years in the TC group. Gantsoudes et al 8 also reported good results of coalition resection and fat interposition for TC coalition in 49 feet (32 patients). They report an average American Orthopaedic Foot and Ankle Society (AOFAS) Hindfoot score of 90/100. However, there was a high rate of revision surgery, one for recurrence (3%), one for incomplete excision (3%) and 11 to correct alignment of the hindfoot (22%).
There have been few studies evaluating the long-term results and incidence of revision surgery for tarsal coalition surgery in a paediatric population. Khoshbin et al 5 evaluated the long-term functional outcomes of resected coalitions at an average follow-up of 14.4 years. They were able to evaluate 24 patients (32 resections) via clinical exam and self-reported functional outcome questionnaires and found most patients had minimal symptoms and few functional limitations, with mean AOFAS scores of 75.8 (sd 30.8) and Foot Function Index scores of 20.0 (sd 18.1). However, in this study they did not comment on reoperation rates for these patients. 5 In a separate, population-based study, Khoshbin et al 11 evaluated the reoperation rates following tarsal coalition resection in all patients treated with a tarsal coalition resection in Ontario, Canada between 1994 and 2009. Mean age at the time of the initial resection was 24.2 years (sd 17.5). They found the overall reoperation rate to be 14% at a mean nine year follow-up. Interestingly, they identified primary arthrodesis as an independent factor associated with need for subsequent surgery.
The present study is the first population-based study to evaluate the reoperation rates following surgical treatment of tarsal coalitions in an entirely paediatric population. At a median follow-up of 14.4 years (IQR 9.3 to 19.7) we found an overall reoperation rate of 8.7%. This rate is slightly lower than reported in prior studies.6,8,11 The median time to reoperation was four years (IQR 1.6 to 15.8) after the index surgery. We did not identify any statistically significant differences between patients who had a reoperation and those who did not based on patient factors, coalition type or composition, or initial surgery performed. This may be limited due to the relatively small number of patients requiring revision. Others have noted higher reoperation rates in patients treated primarily with arthrodesis compared with resection and recommended against primary arthrodesis. 11 While the difference was not statistically significant in the present study, it is notable that 33% (one of three) of the patients treated with an arthrodesis required revision, compared with only 7% of the patients treated with resection (p = 0.2343). Additionally, none of the osseous coalitions required reoperation (p = 0.2936). However, this did not reach statistical significance. While validated patient reported outcomes measures were not available, it is notable that patients treated surgically were less likely to have ongoing symptoms at final follow-up, with 33% of surgical patients reporting symptoms, relative to 67% patients treated nonoperatively (p = 0.0017). Patients with other coalitions were more likely to have persistent symptoms at final follow-up. The reasons for these differences are not clear and further investigation with patient-reported outcomes would be beneficial. Additionally, it is unknown to what degree these patients would benefit from surgery. As a retrospective study the precise indications for operative versus nonoperative management may also confound these results. Patients may not have had reliable surgical options given the coalition size or location, or may have preferred to avoid surgery despite ongoing symptoms.
This study provides a population-based estimate for the rate of repeat surgical intervention for tarsal coalitions in a paediatric population. One of the strengths of the methodology of this study is that it allows for access to the entire medial record of the county residents to allow identification of the tarsal coalitions. The linkage of all the medical records allows for a robust assessment of reoperation rates as the entirety of the patient's record can be reviewed to achieve long-term follow-up, even if follow-up was not with the original provider.
There are limitations to the study, however. Notably, patient-reported outcomes and functional assessments were not available for analysis. Outcomes were limited to patient complaints of persistent symptoms and whether they eventually had a repeat operation at the time of final follow-up. While only 8.7% of patients underwent a second operation, this rate is only a surrogate for patient outcomes. With 33% of the surgical patients reporting ongoing pain or stiffness at final follow-up it is unclear what their degree of symptoms were and why only a few underwent a secondary procedure without more granular detail and formal patient-reported outcomes. Additionally, we were unable to assess other important variables, such as coalition size, precise range of movement measurements or degree of hindfoot deformity. While the overall number of patients was large compared with other similar studies, the power of the study is limited due to the small number of patients requiring a secondary surgery.
In conclusion, to our knowledge, this is the first population-based study in a paediatric population to evaluate the long-term reoperation rates following surgical intervention for tarsal coalitions. At a median follow-up of 14.4 years, patients treated surgically were less likely to report ongoing symptoms relative to patients managed nonoperatively. Reassuringly, we found reoperation rates appear to be low (8.7%) and similar to reports in the adult population. However, further research is recommended to delineate the long-term function of the foot following surgical correction of tarsal coalitions.
Footnotes
TAM reports consulting for Zimmer, Medtronic, and Orthopediatrics, is a board member of POSNA, and course director for Broadwater.
The other authors declare that they have no conflict of interest.
SEM: Study coordination, Data collection.
ANL: Manuscript editing, Vetting of research idea, Study direction.
AAS: Manuscript editing, Study direction.
TAM: Development of initial research question, Manuscript editing, Study guidance.
All authors were involved in the drafting and critical revision of the manuscript and provided final approve of the version submitted.