
Abstract
Abstract
Purpose
This article prospectively examines the functional outcome measures following management of vascular insult secondary to paediatric supracondylar humerus fractures (SCHFX) using validated outcome measures.
Methods
The three-year, prospective, IRB-approved study consecutively enrolled operative SCHFX patients. Clinical data included presence and symmetry of the radial pulse in injured and uninjured extremities, Doppler examination of non-palpable (NP) pulses and perfusion status of the hand. Pediatric Outcomes Data Collection Instruments (PODCI) and the Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) Measures were used to assess functional outcome at final follow-up. Multiple regression analysis was used to determine the relationship between the presence of a vascular abnormality and functional outcome while controlling for other injury parameters.
Results
A total of 146/752 enrolled patients (mean age 6.8 years; range 2 years to 13 years) completed functional outcome measures at final follow-up. Of these, 20 (14%) patients had abnormal vascular exams at presentation: nine (6%) with palpable asymmetric pulse and 11 (7.5%) with NP pulse. Of those with NP pulses, nine/11 (6%) were Dopplerable and two (1.5%) lacked identifiable Doppler signal. Patients with a symmetric, palpable pulse demonstrated better PODCI pain and comfort scores (95.2 versus 85.2) (p < 0.0001), and QuickDASH scores (10.9 versus 21.6) (p < 0.007) compared to those with any abnormal vascular examination. Patients with palpable pulses, regardless of symmetry, demonstrated significantly higher PODCI pain and comfort scores (94.6 versus 84.7) (p < 0.003) than NP pulses.
Conclusions
In children with operative SCHFX, an abnormal vascular examination at presentation is predictive of poorer outcomes in pain and upper extremity function. A palpable pulse, versus NP, is predictive of better pain and comfort at final follow-up.
Level of evidence
II
Introduction
Vascular injury is a well-known complication of paediatric supracondylar humerus fractures (SCHFX) and the management of these complications has been described in great detail.1–16 To our knowledge, however, there are no prospective studies that have correlated pre-operative vascular status to functional outcomes. In a retrospective study, Scannell et al reported on 20 patients with perfused, pulseless supracondylar humerus fractures treated with closed reduction, percutaneous pinning and observation. At a minimum of six months follow-up, they found that 13/20 patients had higher functioning in all domains of the Pediatric Outcomes Data Collection Instruments (PODCI) questionnaire compared with the general population. 2 In another retrospective study, Wang et al reported functional outcomes on 154 patients with Gartland type III injuries and how neurovascular injury impacted outcomes. They concluded that neurovascular injury did not impact functional status post-operatively. 17 The purpose of this study is to prospectively determine if pre-operative vascular examination is predictive of functional outcome following the operative management of paediatric SCHFX using validated outcome measures.
Methods
An IRB-approved prospective enrollment of consecutive patients with operative SCHFX was performed over a three-year period at a level one trauma paediatric hospital. All patients under the age of 18 years were included and the treatment of fractures was determined after the clinical and radiographic assessment by 11 attending paediatric orthopaedic surgeons. Patients were excluded if they were skeletally mature, sustained an adult-type extraarticular or intercondylar distal humerus injury requiring open reduction and internal fixation with plates and screws, or had less than ten weeks follow-up. Demographic data, radiographic diagnosis, details of the mechanism of injury and physical exam findings were entered into an IRB-approved database by the attending surgeon. Recorded data included gender, age, laterality, fracture type (flexion versus extension and modified Gartland classification), direction of displacement of the distal segment, mechanism of injury, skin and soft tissue exam findings (open versus closed, tenting, soft tissue swelling, evidence of compartment syndrome), neurological exam findings and the vascular status of the injured extremity.
Timing of surgery was determined by the attending orthopaedic surgeon on call. Doppler examinations were performed when a pulse could not be palpated. The majority of patients were treated with closed reduction and percutaneous pin fixation. Open reduction and percutaneous pinning was performed when an acceptable closed reduction could not be obtained, or vascular exploration was deemed necessary. Pin configurations were at the discretion of the treating surgeon as was the type and length of post-operative immobilization. Vascular exploration and/or repair were conducted in the setting of poor perfusion following reduction and fixation. Extremities that demonstrated adequate perfusion (e.g. pink, warm hand with brisk capillary refill) were observed post-operatively in the in-patient setting for maintenance of perfusion.
Patients were followed until evidence of clinical and radiographic healing. Formal outpatient physical therapy was not routine and was at the discretion of the treating surgeon. At the final appointment, functional outcomes were assessed using PODCI and the Quick Disability of the Arm, Hand and Shoulder Questionnaire (QuickDASH).
Patients were stratified by vascular examination as either ‘normal’ (NORM) or ‘abnormal’ (ABN). A ‘normal’ exam entailed a palpable radial and/or ulnar pulse that was symmetric to the contralateral, uninjured extremity. An ‘abnormal’ exam was further subclassified as palpable but diminished/asymmetric to the contralateral extremity (ASYM); non-palpable (NP) but Dopplerable (DOP); or NP and non-Dopplerable (avascular, AVSC). Comparisons were also made between all palpable (PALP) and all NP exams (Fig. 1). Given that vascular exams can be an evolving phenomenon, all exams recorded were those done by the attending surgeon on call in the pre-operative holding area immediately prior to surgery.
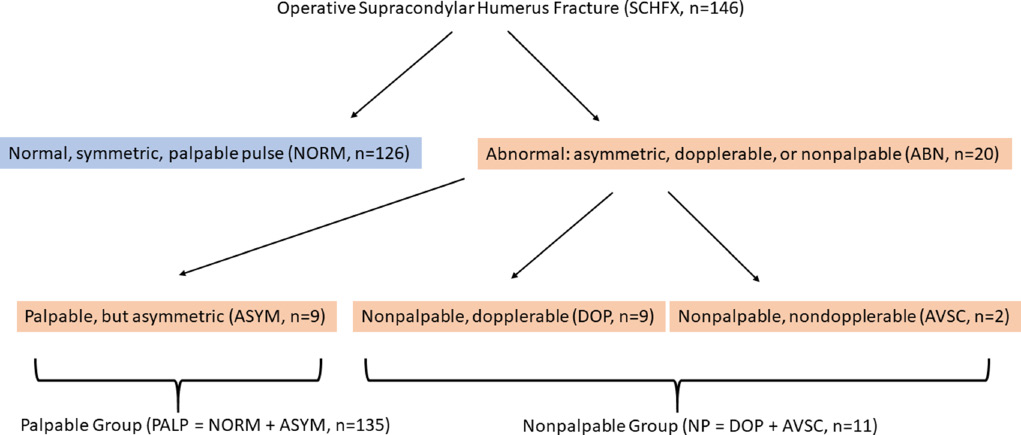
Flow diagram demonstrating vascular examination stratification.
Statistical analysis
Univariate analyses were performed to determine the differences in outcome score of various vascular examinations. p-values were considered significant at a value of < 0.05 using the non-parametric test and ANOVA analysis. When statistical significance was found, multivariate analysis was used to determine the relationship between vascular examination and functional outcome while controlling for other injury parameters. Demographic comparisons were made using the paired t-test, ANOVA, Chi-Square and Fischer exact tests where applicable. All statistics were performed by a PhD biostatistician.
This study was approved by the institutional review board and no external funding was received.
Results
In total, 752 patients were enrolled and 146 (19.4%) completed functional outcome measures at final follow-up (mean 87 days, range 70 days to 408 days). There were 76 males and 70 females at a mean age of 6.8 years (range 2 years to 13 years). Of the injuries, 59% (86/146) occurred on the left side (Table 1).
Distribution of varying vascular examinations
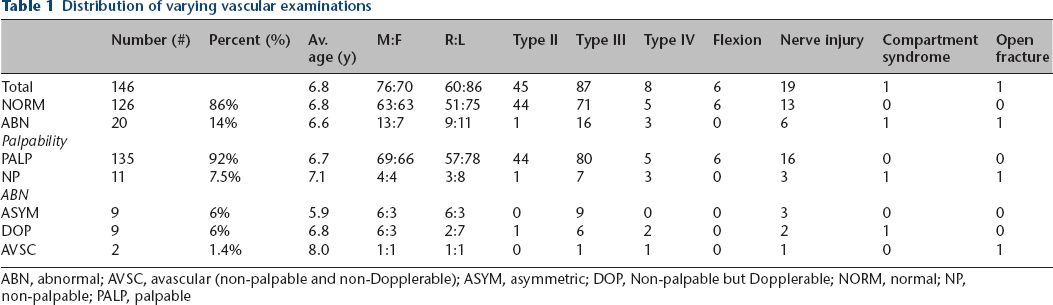
ABN, abnormal; AVSC, avascular (non-palpable and non-Dopplerable); ASYM, asymmetric; DOP, Non-palpable but Dopplerable; NORM, normal; NP, non-palpable; PALP, palpable
Fracture pattern and classification
Of the injuries, six/146 (4%) were flexion-type (FLEX) and 140/146 (96%) were extension-type (EXT) fractures. Of the EXT fractures, 45/140 (32%) were type II injuries (EXT-2), 87/140 (62%) were type III injuries (EXT-3), and eight/140 (6%) were type IV injuries (MULTI). Of the extension injuries, 45/140 (32%) were posteromedially displaced (PM), 43/140 (31%) were posterolaterally displaced (PL), 44/140 (31%) were directly posteriorly displaced (PE). The remaining eight/140 (6%) fell into the MULTI subgroup (Table 1).
Vascular examination
There were 126/146 (86%) normal vascular exams (NORM) while 20/146 (14%) of patients had an abnormal vascular exam (ABN) at initial presentation. Palpable pulses (PALP) were present in 135/146 (92%) patients. Nine/146 (6%) presented with a palpable, asymmetric/diminished pulse (ASYM) while 11/146 (7.5%) were NP. Of the NP, nine/146 (6%) were Dopplerable (DOP) while two/146 (1.5%) had no identifiable Doppler signal and were considered AVSC (Table 1). Both patients in the AVSC group and one in the DOP group had cool, poorly perfused hands.
Associated injuries
There were 19/146 (13%) patients with associated neuropraxic injuries. In patients with a nerve injury, 13/19(68%) were patients with NORM vascular exams while six/19 (32%) had ABN exams. Three/19 (16%) nerve-injured patients had ASYM exams. Of the patients with nerve injuries, 16/19 (84%) were PALP while three/19 (16%) were NP. Of the NP with associated nerve injuries, two/19 (10.5%) were DOP and one/19 (5%) was AVSC. At final follow-up, all patients with nerve injuries had resolution of such. There was one case (one/146, 0.7%) of compartment syndrome in a patient with a DOP vascular examination. There was one (one/146, 0.7%) open fracture in a patient with an AVSC exam.
There were significantly more ABN exams in EXT-3 than EXT-2 (p < 0.02), and in MULTI than EXT-2 (p < 0.009). Patients with ABN exams were more likely to have an associated nerve injury than patients with NORM exams (p < 0.03). There were no other differences observed between NORM and ABN with regards to age, sex, laterality, nerve injury, compartment syndrome or open fracture (p > 0.2). MULTI injuries were more likely to occur than EXT-2 and EXT-3 injuries in NP versus PALP patients (p < 0.009 and p < 0.04, respectively). There were no other differences observed between PALP and NP with regards to age, sex, laterality, fracture type/classification, nerve injury, compartment syndrome or open fracture (p > 0.1). Comparisons were made between the varying vascular exams. Due to the small number of AVSC patients, these were combined with DOP for analysis of the NP group. NP, ASYM and NORM were compared. EXT-3 and MULTI patients were more likely to have ASYM or NP exams than EXT-2 patients (p < 0.03 and p < 0.009, respectively). ASYM and NP patients were more likely to have an associated nerve injury than NORM patients (p < 0.04). There were no other differences observed between NORM, ASYM and NP with regards to age, sex, laterality, fracture type/classification, nerve injury, compartment syndrome or open fracture (p > 0.1).
Of the patients with AVSC exams, one patient required reverse saphenous interposition grafting while the second had open exploration of a kinked brachial artery. Following detethering of the artery, there was no observed vascular defect and perfusion returned and no repair/reconstruction was performed. One patient with a NP, Dopplerable exam received a reverse saphenous interposition graft due to an inadequately perfused limb.
Functional outcomes
PODCI and QuickDASH scores were obtained at final follow-up, mean 12 weeks ((mean 87 days, range 70 days to 408 days), post-operatively. The mean PODCI global functioning and QuickDASH scores were 92.9 (range, 32.0 to 100) and 11.9 (range, 0 to 65.9), respectively (Table 2).
Outcomes as determined by vascular examination
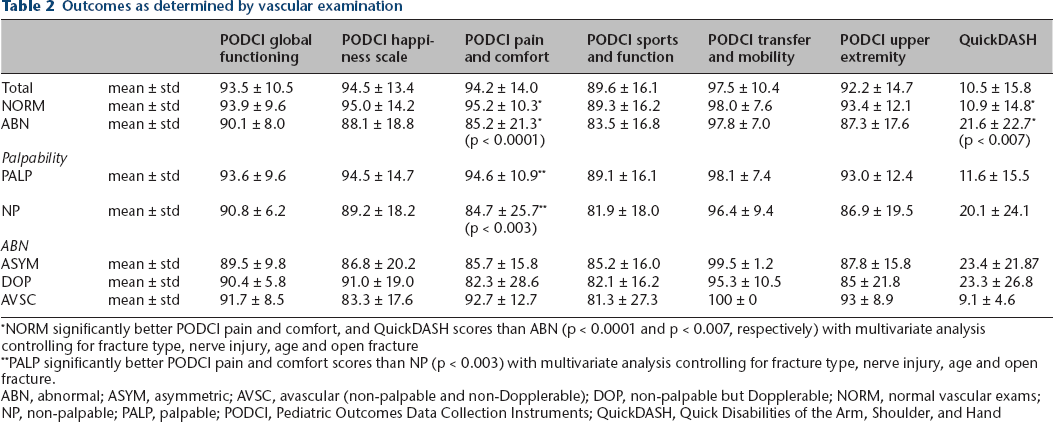
NORM significantly better PODCI pain and comfort, and QuickDASH scores than ABN (p < 0.0001 and p < 0.007, respectively) with multivariate analysis controlling for fracture type, nerve injury, age and open fracture
PALP significantly better PODCI pain and comfort scores than NP (p < 0.003) with multivariate analysis controlling for fracture type, nerve injury, age and open fracture.
ABN, abnormal; ASYM, asymmetric; AVSC, avascular (non-palpable and non-Dopplerable); DOP, non-palpable but Dopplerable; NORM, normal vascular exams; NP, non-palpable; PALP, palpable; PODCI, Pediatric Outcomes Data Collection Instruments; QuickDASH, Quick Disabilities of the Arm, Shoulder, and Hand
Multivariate analysis was performed and NORM patients demonstrated better outcomes only in PODCI pain and comfort scales (95.2 versus 85.2) (p < 0.0001), and QuickDASH scores (10.9 versus 21.6) (p < 0.007) compared to ABN when controlling for fracture type, neurologic status, age and open fracture (Table 2). PALP only demonstrated significantly better PODCI pain and comfort scales (94.6 versus 84.7) (p < 0.003) compared to NP when controlling for fracture type, neurologic status, age and open fracture. No other statistically significant differences in outcomes scores were identified between patients with other varying types of vascular examinations or outcomes scores (ASYM versus NP; ASYM versus AVSC; DOP versus AVSC; PALP+DOP versus AVSC) (p > 0.05) (Table 2).
Discussion
This is the first study to prospectively correlate functional outcomes of surgically treated supracondylar humerus fractures with pre-operative vascular status. The mean PODCI global functioning and QuickDASH scores of 92.9 (range, 32.0 to 100) and 11.9 (range, 0 to 65.9), respectively, represent generally excellent outcomes at an mean of 12 weeks (range, 10 to 58 weeks) follow-up.
Compared to patients with a normal pulse exam, those with abnormal exams (asymmetric/diminished, Dopplerable only or avascular) have greater discomfort as determined by the PODCI pain and comfort score and greater levels of disability as determined by QuickDASH scoring. The presence of a pulse (normal or diminished) predicts better outcomes as measured by the PODCI pain and comfort score than when a pulse is not palpable (Dopplerable only or avascular). There were no other significant differences observed when comparing other various vascular exam patterns.
The American Academy of Orthopedic Surgeons’ PODCI is a validated scoring system designed to evaluate physical and psychosocial health status in the paediatric population. It has been tested in many orthopaedic conditions and has minimal floor and ceiling effects compared to other outcomes measures.18–20 The PODCI has previously been used to assess the outcome at intermediate follow-up for operatively treated perfused, pulseless SCHFX. Scannell et al retrospectively demonstrated these patients have high PODCI scores after closed reduction, pinning and observation of their vascular status at an mean of 20 months (range, six months to 56 months) follow-up. 2 In their study, 13/20 patients had higher functioning in all domains of the PODCI questionnaire when compared to the general population. Only two patients had lower values on PODCI global functioning scores – one of which had an occluded brachial artery and another with a patent artery. Another study by Wang et al utilized functional outcomes to retrospectively compare patients presenting with normal versus abnormal neurovascular exams. They determined that neurovascular injury pre-operatively had no effect on functional outcomes as measured by PODCI and QuickDASH scores at a final follow-up of 38 months. Ultimately, the majority of patients returned to high levels of function. 17
As mentioned above, we have found significant differences in PODCI pain and comfort scores when comparing normal vascular exams to abnormal vascular exams. This was also true when comparing palpable to NP pulses. Interestingly, patients with NP but Dopplerable pulses demonstrated the lowest pain and comfort scores (82.3) while those with avascular exams demonstrated rather high scores (92.7). This difference was not, however, statistically significant, which is likely due to the low number of patients in each of these categories.
The QuickDASH is an 11-item, shortened version of the DASH questionnaire (30 items) that is routinely used in research involving upper extremity musculoskeletal disorders. The QuickDASH has been proven to be as precise, consistent and valid as the DASH questionnaire in the paediatric population.21,22 While the QuickDASH has been validated in children above the age of eight years, other authors have reported functional outcomes with the QuickDASH in children of varying ages with SCHFX, specifically.23,24
In the present study, we identified differences in the QuickDASH when comparing patients with normal vascular exams to abnormal exams pre-operatively (10.9 versus 21.6). Other notable differences in QuickDASH scores were observed between those with palpable and those with NP pulses (11.6 versus 20.1), however, these did not reach statistical significance and this is likely due to the lower number of patients in the NP group. Interestingly, patients in the avascular group had the best QuickDASH scores in the cohort (9.1) while patients with asymmetric pulses and Dopplerable pulses had the poorest scores (23.4 and 23.3 respectively). Again, the lack of differences observed when comparing among these groups is most likely due to the lower number of patients in each of these categories. The excellent scores in the avascular group are consistent with what has been previously reported in the literature for pulseless injuries. Schoenecker et al reported on seven children with pulseless arms requiring vascular exploration after closed reduction and percutaneous pinning. 12 They noted that at a mean follow-up of 30 months (range, 6 months to 79 months), all patients had normal circulatory status in conjunction with a normal carrying angle and normal elbow motion. Outcomes measures were not recorded, however. It is also important to note that the minimally clinically important difference of the QuickDASH has been reported to range from 20 to 15.9 points.25,26 Thus, regardless of whether statistical significance was achieved, none of the comparisons in our current study reach the minimally clinically important difference.
We found that patients with abnormal exams (asymmetric or NP) were more likely to present with a concomitant nerve injury. Mangat et al found that patients with Gartland type III fractures, a pre-operative median or anterior interosseous nerve injury, and a pink pulseless hand were very likely to have a vascular injury that would benefit from early exploration. 13 In the current study, we did not note a ‘pink, pulseless’ exam, but rather stratified NP patients as Dopplerable, or avascular, thus we could not draw any comparisons to Mangat's study regarding median/anterior interosseous nerve injury and vascular compromise. We do note that of the six patients with nerve injuries and abnormal vascular exams, four presented with AIN injuries, and one with an AIN/median nerve injury. The one patient requiring exploration and grafting had an AIN injury. In the present population, however, all patients with nerve injuries had resolution of such at their final follow-up appointment.
An acknowledged weakness of this study is the relatively low number of patients who completed all outcome measures and/or the final follow-up assessment. We have found it common for families to fail to continue follow-up once the family considers the child to be healed and returned to full activity. Many patients in our population are transferred for acute care from other cities by plane, helicopter or long drives. As such, some patients request to follow-up with an orthopaedic surgeon closer to home. Patients who experience complications from the injury or procedure are more likely to continue follow-up and may represent a higher percentage of patients in our database. As such, we believe that the reported scores could be representative of the most complicated patients. Nonetheless, our study population remains one of the largest reported.
Secondly, we are unable to accurately correlate the elapsed time from injury to treatment as a possible variable affecting outcome. Studies have shown that without neurovascular injury, polytrauma or skin complications, fixation can be safely delayed without increasing the risk of complications or sacrificing good outcomes.27–31 In our study, the urgency of fracture fixation was surgeon dependent. Additionally, we do not have data commenting on the evolution of the vascular exam – whether the pulse was different in the emergency department, versus pre-operative hold, versus the operating room, and how long to resolution after fixation. To account for this, we attempted to present our data in the most reproducible way possible by classifying our pre-operative exam as that of the attending surgeon's in the pre-operative holding area. Comparing this single time point to outcomes scores is the focus of the current study. Further studies that take into consideration the evolution of the vascular exam over time are warranted.
Lastly, one may question as to whether a 12-week minimum follow-up is effective at predicting outcomes, particularly differences in pain and comfort as is potentially reflected in the PODCI scores presented. Spencer et al determined that gains in range of motion will continue to occur at up to one year post-operatively, however, about 87% of the range of motion arc is established by 12 weeks after a SCHFX. 32 As a result, this 12-week follow-up point is typically the time at which most operatively treated SCHFX are discharged from clinic. While longer-term follow-up and longitudinal assessment beyond 12 weeks might have altered results with regard to outcome measures (presumably revealing continued improvement with time as was found by Wang and colleagues), our data is nonetheless helpful in characterizing outcomes at the time children are of typically released to full activities and discharged from clinic. 17 Therefore, this study will hopefully aid clinicians in reassuring families that although their child who initially presented with an abnormal vascular exam may still not be back to ‘normal’ with regard to patient-reported outcomes at time of discharge, they may very well continue to improve with time.
Conclusion
This is the first study to prospectively correlate validated outcome scores and pre-operative vascular exam characteristics in children with operative SCHFX. The majority of patients who completed functional outcomes at final follow-up did well after treatment of their injury. An abnormal vascular exam is statistically predictive of poorer outcomes with regards pain and function at time of typical discharge from clinic, although this does not necessarily correlate with a clinically important difference in outcome. The presence of any palpable pulse predicts statistically better pain outcomes than when a pulse is absent.
Footnotes
RLW: Conception of design and acquisition of data, Analysis and interpretation of data.
CAH: Conception of design and acquisition of data, Analysis and interpretation of data, Critical revision and final approval.
AIR: Conception of design and acquisition of data, Analysis and interpretation of data, Drafting manuscript, Critical revision and final approval.