
Abstract
Abstract
Purpose
Calcaneus lengthening can be used in symptomatic flat foot in children, but few details on its medium-term results and complementary procedures are available.
Methods
A total of 20 flexible, symptomatic, idiopathic valgus flat feet (in 15 children; mean age 13.9 years (10 to 17)) were operated on. Complementary procedures were based on preoperative and intraoperative analyses. Radiographic measurements were obtained preoperatively and with at least four years follow-up.
Results
At a mean of 8.3 years (4 to 15) postoperatively, 13 feet had good clinical and radiological results, with significant improvement in American Orthopaedic Foot & Ankle Society Ankle-Hindfoot scale scores and radiological measurements. Seven feet had residual pain. Six of them had no osteotomy of the first cuneiform.
Conclusion
Calcaneus lengthening with adequate complementary musculo-tendinous and/or bone procedures according to preoperative and intraoperative foot deformation leads to good medium-term results. Forefoot supination is the most frequent residual defect. If present intraoperatively, first cuneiform pronation-flexion osteotomy is indicated.
Level of evidence
IV
Introduction
Valgus flat foot is common in children and adolescents, with a 12.5% incidence, but it is rarely disabling. 1 Various surgical options can be proposed when conservative management is insufficient. Soft-tissue procedures are always used in addition to bone procedures.2,3 Grice's extra-articular talocalcaneal arthrodesis induces hindfoot stiffness. 4 The horseman procedure involves temporary blocking of the talocalcaneal unit by a screw to correct subtalar valgus. 5 The screw can be removed after six months. The mid-term outcomes of subtalar arthroereisis appear to be encouraging, but medium- and long-term data are lacking.6–9 Inflammatory reactions and displacement with loss of correction have been described. 10 Calcaneus medialization osteotomy corrects only the hindfoot. 11 It can be combined with a calcaneal and cuboid osteotomy in the ‘triple C’ osteotomy. Triple arthrodesis should be used only for stiff feet. Calcaneus lengthening using the technique described by Evans and updated by Mosca could correct the main valgus flat foot disorders.2,12 Few mid- or long-term results have been published. 3 The aims of this study were to evaluate the medium-term outcomes of calcaneus lengthening in idiopathic valgus flat foot in children and adolescents, and to identify the appropriate complementary procedures that must be performed.
Materials and methods
In this retrospective study, the inclusion criteria were idiopathic valgus flat feet treated by calcaneus lengthening with a minimum follow-up period of four years. Surgery was indicated in cases of idiopathic symptomatic (painful) flexible flat foot that was resistant to conservative treatment during at least six months. Medical records of patients treated using this technique between 2000 and 2012 were reviewed. All patients were contacted for standardized follow-up examination. We excluded non-idiopathic valgus flat feet operated on using this technique, and cases with less than four years follow-up.
Surgical procedure
When triceps retraction was detected on preoperative clinical examination, the first surgical procedure was triceps elongation, achieved by sliding it in its tendon or by fasciotomy of the gastrocnemius. Intramuscular elongation of peroneus brevis muscle was also performed in cases of fibular retraction. The calcaneus was approached laterally after extra-periosteal elevation of the extensorum digitorum brevis. Constriction between the anterior and middle calcaneal articular facets was identified visually and radiographically before osteotomy. Calcaneus osteotomy was performed 15 mm to 20 mm from the calcaneocuboid joint, perpendicular to the major axis of the calcaneus. The calcaneocuboid joint was maintained temporarily with two pins to avoid subluxation during lengthening. Two trapezoidal autogenous iliac grafts (10 mm to 15 mm wide) were inserted. Their width was determined by the length needed to correct the forefoot. Two longitudinal pins were introduced successively from the distal fragment into the graft, and finally into the proximal fragment. Calcaneocuboid stabilization pins were removed after calcaneus lengthening to judge forefoot position. In case of residual supination, plantar base osteotomy of the medial cuneiform was performed with a staple, enabling pronation and flexion of the medial arch. 12 Postoperatively, cast immobilization was applied with non-weight bearing for five weeks and then with complete weight-bearing for another five weeks after pin removal.
The clinical parameters collected preoperatively and at last follow-up were walking perimeter, and discomfort or pain during sport practice or in daily life. The American Orthopaedic Foot & Ankle Society Ankle-Hindfoot scale score (AOFAS-AH) (good > 90; fair 80 to 90; poor < 80) was calculated. 13 Data on the surgical procedures associated with calcaneal osteotomy and the presence of postoperative complications were collected.
Standard weight-bearing dorsoplantar and lateral radiographs were taken of all feet preoperatively and at last follow-up. All the radiographs were analyzed by the two authors using a digital picture archiving and communication system. According to the site of deformation, feet were classified in four patterns using preoperative radiographs and Bourdet et al's 14 system: subtalar pes planus with marked subtalar valgus and longitudinal sag predominating at the talonavicular joint, midtarsal pes planus without subtalar valgus but with marked midtarsal abduction and sag predominating at the cuneonavicular joint, mixed pes planus with subtalar valgus, midtarsal abduction and sag at both the talonavicular and cuneonavicular joints, and pes planocavus with sag of the medial arch and cavus deformity of the lateral arch. On dorsoplantar view, the talocalcaneal angle, the talo-first metatarsal angle, the calcaneo-fifth metatarsal angle and talonavicular coverage were measured; on lateral view, the talocalcaneal angle, the talo–first metatarsal angle, the calcaneus pitch angle and the talo-horizontal angle were measured. 15 At last follow-up, we looked for the signs of calcaneocuboid osteoarthritis, and subluxation was determined on lateral view by dividing the measurement of the dorsal height of the articular surface of the calcaneus above the cuboid by the total length of the articular surface of the calcaneus at the calcaneocuboid joint and multiplied by 100. 16
Statistical analysis
Pre- and postoperative data were compared using the signed-rank paired Wilcoxon test. A p-value < 0.05 was considered to be significant.
Results
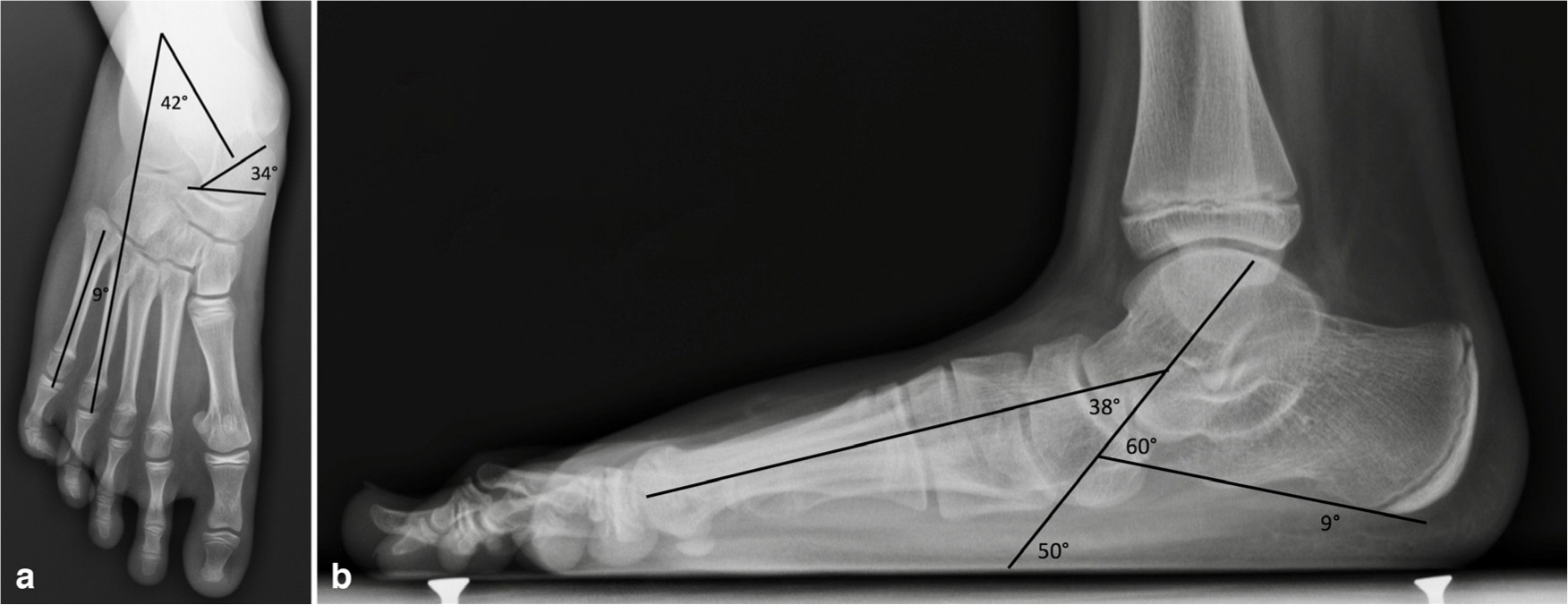
We operated on 20 feet in 15 patients. The mean age at the intervention was 13.9 years (10 to 17). The mean follow-up duration was 8.3 years (4 to 15) (Table 1). The sample comprised four subtalar and 16 mixed flat feet (Table 2). Patient 4 was lost to follow-up after four years, and revision surgery was performed on one foot due to a persistent lack of anteromedial support after surgery. All feet required tricipital lengthening prior to osteotomy. A total of 15 feet had short fibular muscle lengthened. Calcaneus lengthening led in ten cases to intraoperative forefoot supination requiring correction by pronation-flexion osteotomy of the medial cuneiform. The AOFAS-AH score increased from 73 to 96 (p < 0.01). Mean radiological measurements improved significantly (Table 2; Figs 1a, 1b, 2 and 3). In all, 13 feet had good clinical and radiographic results, with painless, flexible normal orientation; these patients resumed sports activities. Four patients (seven feet) had residual pain. Three of these patients (six feet) had postoperative residual supination of the forefoot which was unmasked in non-weight bearing while correcting the hind foot. This residual defect became symptomatic within a few months. These three patients did not undergo osteotomy in the medial arch. Three of our patients underwent additional surgery. One patient underwent reoperation with plantar-based subtraction osteotomy in the medial cuneiform (patient 4). Patient 15 had a sepsis of the right foot, which required a sural flap and early pin removal. Secondary displacement appeared, causing plantar pain adjacent to the distal end of the calcaneus and subluxation and pinching of the calcaneocuboid joint at last follow-up. He was the only patient with a suspicion of early osteoarthritis at last follow-up. Patient 2 had a cuneiform osteotomy nonunion that became symptomatic after two years and required reoperation to achieve consolidation, but was asymptomatic at last review.
Clinical evaluation preoperatively and at last follow-up
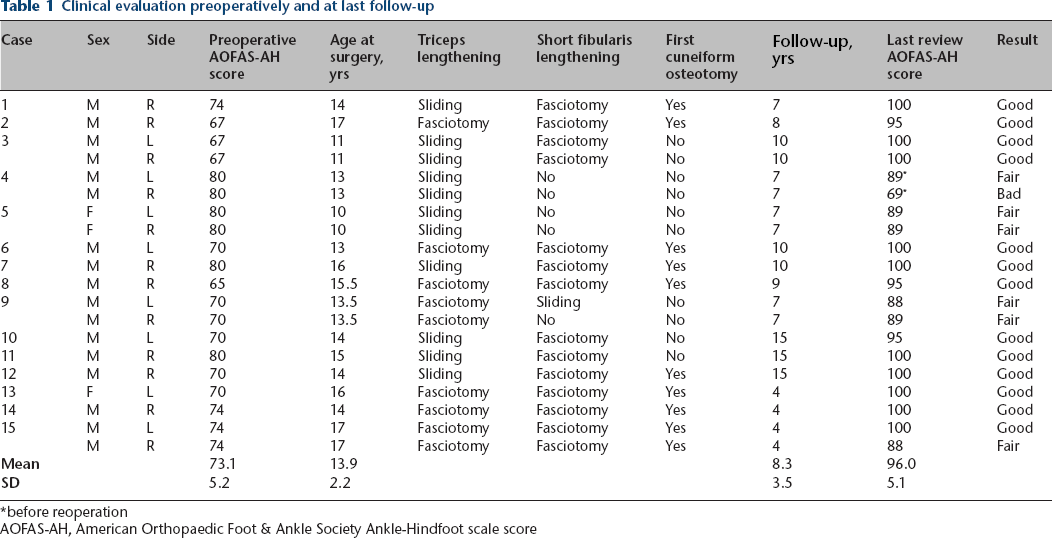
before reoperation
AOFAS-AH, American Orthopaedic Foot & Ankle Society Ankle-Hindfoot scale score
Radiological measurements obtained preoperatively and at last follow-up
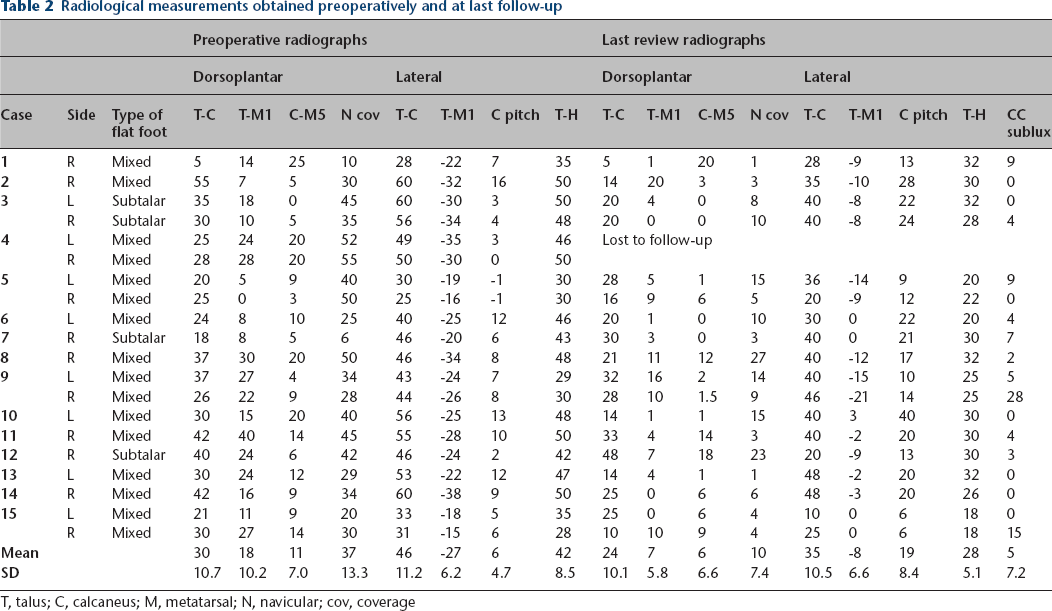
T, talus; C, calcaneus; M, metatarsal; N, navicular; cov, coverage

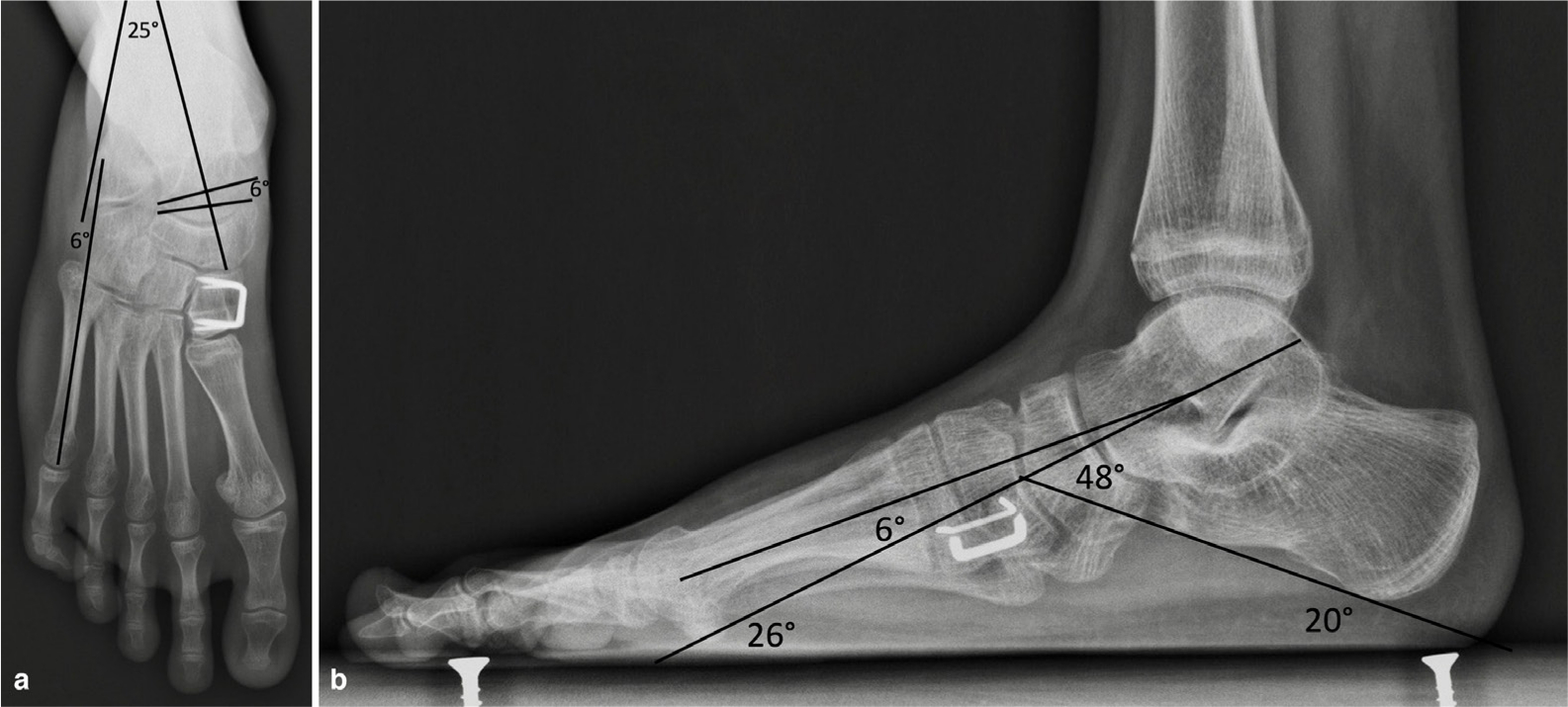
Radiograph obtained immediately after surgery showing correction of the various defects, the two calcaneal stabilization pins and the correction of residual forefoot supination after calcaneal lengthening by a pronation-flexion osteotomy of the first cuneiform. The insert picture is the preoperative weight bearing film of the patient. The arrows show the effect of the medial cuneiform osteotomy.
Discussion
Calcaneal lengthening with adequate complementary musculo-tendinous and/or bone procedures according to preoperative and intraoperative foot deformation led to good medium-term results in 65% of cases. Some complications may affect these results (infection, nonunion and residual deformity). The essential complementary procedure is the correction of intraoperative residual forefoot supination by pronation-flexion osteotomy of the medial cuneiform after calcaneal lengthening. Three of our patients had pain during follow-up because of poor intraoperative assessment of this deformity, which required revision surgery in one case.
According to the calcaneopedal unit concept, in a flat foot, the forefoot is supinated in relation to the hindfoot. 17 Calcaneal lengthening inverts the acetabulum pedis along the axis of Henke. The calcaneal lengthening can uncover an intrinsic forefoot supination deformity. If the foot is flexible, this supination can resolve spontaneously, probably thanks to the plantar fascia that forces the bones to realign. In some severe flat feet, this supination is stiff and requires an additional osteotomy of the medial cuneiform. We decided to perform this osteotomy in most patients with supination that was unmasked intraoperatively after the calcaneus lengthening. A simulated intraoperative weight bearing radiograph could help to appreciate this residual supination. We had a few cases of patients who had clinically poorly tolerated this residual supination. Most of the time the first cuneiform osteotomy is a pronation-flexion plantar-based subtraction osteotomy. It is recommended when supination is associated with a forefoot in abduction or neutral position. If supination is associated with an adducted foot, this osteotomy should be a dorsomedial base opening. 18 We have not had this situation in our patients. As classified by Bourdet et al, 14 the majority of flat feet were of the mixed type. Four feet were classified as the pure subtalar type, but calcaneal lengthening did not lead to adduction of the forefoot.
We used a tricortical iliac graft. In his original technique, Evans used a graft taken from the homolateral tibia. 2 Some authors have reported good results of allograft use. 19 Like most authors, we use bone fixation.20,21 We used two longitudinal pins inserted percutaneously in the distal-proximal direction. Mosca described this technique, and left the pins in only in cases of graft or calcaneocuboidal joint instability. 12 Using his original technique, Evans 2 merely embedded the graft in the osteotomy site. Good calcaneal vascularization and press-fit of the osteotomy would allow performance of the procedure without bone fixation. Nevertheless, we continue to use bone fixation to ensure stability, avoiding the possibility of secondary displacement. 22 This loss of correction occurred in the patient requiring early pin removal.
In our experience calcaneal lengthening didn't lead to degenerative changes, except in patients who had a secondary displacement. Some
Few studies have examined only idiopathic valgus flat feet treated by calcaneus lengthening. Mosca 12 operated on 25 feet, five of which were idiopathic, with good results except in the two most severe cases. Phillips 3 reviewed the outcomes of 23 feet, 15 of which were idiopathic, with a follow-up duration of seven to 20 years, operated on by Evans, and documented the sustainability of good results. 3 Akimau and Flowers 24 presented mid-term results from 11 children who underwent surgery, with an average follow-up duration of 4.5 years, and recommended performance of this intervention ‘a la carte’ with various associated procedures.
Other non-stiffening surgical techniques are of interest. Based on the medial translational osteotomy described by Koutsogiannis 11 and Rathjen and Mubarak 25 performed triple calcaneo-cuboid-cuneiform (‘triple C’) osteotomy on 24 valgus flat feet of patients with a mean age of 11.5 years. 11 Moraleda et al 26 compared 30 idiopathic flat feet treated with ‘triple C’ osteotomy with 33 such feet treated with calcaneus lengthening. The mean age at the time of surgery was 11 years. Mean follow-up durations were 2.7 years for the ‘triple C’ group and 5.3 years for the calcaneus-lengthening group. The authors observed no significant difference in clinical outcome. Calcaneus lengthening provided superior correction of talo-navicular coverage. That's why we prefer calcaneus lengthening to ‘triple C’ in flexible feet. In their series, one out of two patients in the calcaneus lengthening group had calcaneocuboid subluxation at last follow-up. Only five patients underwent calcaneocuboid joint stabilization prior to elongation. The presence of this subluxation did not affect the AOFAS-AH score.
Some authors reported good results of the use of the ‘calcaneostop’ screw and subtalar implants which allows extra-articular subtalar arthroereisis.9,10 Correction of the foot was performed during the surgical procedure and by a proprioceptive effect. The subtalar arthroereisis is a minimally invasive procedure that provides good mid-term outcomes but material migration and pain can occur and AOFAS-AH scores and radiographic corrections are less improved than in calcaneal lengthening.27,28 The horseman procedure shares the same principles as the subtalar arthroereisis techniques. Temporary blocking the calcaneopedal unit by a screw allows satisfying immediate and long-lasting correction. 5 We feel that these procedures might be an alternative for the subtalar flat feet (predominant valgus deformation) in young patients.
This study has some limitations. It is a retrospective study with relatively few patients operated over a long period, because the surgery was indicated for painful flat feet as a last resort. The AOFAS-AH score was used in some other studies about flat feet in children and adolescents.21,24,26-28 This score is not validated in children and there are serious concerns even from the AOFAS. 29 The Oxford Ankle Foot Questionnaire for Children is a validated system that could be a good alternative. 30 Our first patients were operated on before this score was published.
Conclusion
These medium-term results confirm that stiffening procedures (arthrodesis) can be avoided in the treatment of idiopathic valgus flat foot in children and adolescents. When this condition becomes symptomatic, calcaneus lengthening is helpful, provided that the surgical technique is strictly adhered to and associated with the appropriate complementary procedures. This approach requires careful preoperative and, particularly, intraoperative evaluation of deformation. Residual supination of the forefoot must be evaluated after lengthening of the external column. If this condition is present, pronation-flexion osteotomy of the first cuneiform must be performed.
Footnotes
MD: Data acquisition, Analysis and interpretation of data, Drafting and revision of the manuscript.