
Abstract
Abstract
Purpose
Epidemiological studies on idiopathic clubfeet have shown a typical distribution consistent across ethnic groups: bilaterality in about 50% of cases and a male to female ratio of 2:1. Whether this corresponds also to differences in severity according to laterality and sex has been poorly evaluated. As well, the correlation between family history and severity has not been previously investigated. The aim of this study was to investigate how laterality, sex and family history influence severity and treatment.
Methods
In all, 97 infants with idiopathic clubfoot (81 male, 16 female; 55 unilateral, 42 bilateral; 19 with a first or second-degree relative affected) consecutively treated with Ponseti method were prospectively enrolled. Initial severity (according to Dimeglio and Pirani scores) and treatment (number of casts and need for tenotomy) were analyzed in the different subgroups.
Results
Initial severity according to Pirani (p = 0.020) and Dimeglio score (p = 0.006), number of casts (p = 0.000) and tenotomy (p = 0.045) were significantly higher in bilateral than in unilateral cases. In bilateral cases, a significant correlation was found between the right and left foot of each patient in terms of initial severity, number of casts and tenotomy performed. No statistically significant difference was found according to sex and family history.
Conclusions
This study has confirmed the different behaviour of bilateral cases reported by previous studies; bilateral cases are more severe and show similar features in their right and left foot. This could be the result of different pathogenic mechanisms, likely on a genetic basis. Sex and family history did not seem to influence severity.
Level of Evidence
Level of evidence II
Introduction
Congenital talipes equinovarus or clubfoot is one of the most common congenital birth defects, with a reported incidence of one to two per 1000 newborns. 1 It is characterized by ankle equinus, heel varus, plantar arch cavus and forefoot adduction, with a wide range of severity and possible unilateral or bilateral involvement (about 50% of cases respectively). 2
In most cases the deformity is isolated and idiopathic, whereas in about 20% of cases is associated with syndromic conditions (distal arthrogryposis, congenital myotonic dystrophy, myelomeningocele, amniotic band sequence or other genetic syndromes such as trisomy 18 or chromosome 22q11 deletion syndrome). 3
Despite modern advances, the complex aetiology and pathogenesis of clubfoot is still unclear and the cause of phenotypic variability in affected individuals is unknown. 4
Epidemiological studies have provided support to researchers’ hypothesis, showing different distribution and phenotypes in different subgroups. For example, differences in clubfoot prevalence across ethnic populations 3 and the higher concordance rate for identical twins compared with fraternal twins (33% versus 3%)4,5 support a genetic basis for isolated clubfoot.
Recently, different clinical features have been described in bilateral cases (higher severity6,7 and larger distribution of severity 2 ) in comparison with unilateral patients which, therefore, would represent different phenotypes due to different pathogenic mechanisms or underlying genetics. 2
On the other hand, when an analysis based on sex distribution is performed, a male to female ratio of 2:1 is found in isolated clubfoot that is consistent across ethnic groups.4,5 The reason for this sex discrepancy, in the absence of sex-linked inheritance, is currently unknown. 4 Even though some previous investigators have postulated that female sex may represent a more severe clubfoot phenotype due to underlying genetic mechanisms,8,9 no difference in initial severity with respect to sex has been found. 2
Another support to a genetic basis is the fact that about 24% to 50% of all patients with isolated clubfoot (depending on the populations studied) report a positive family history for clubfoot.4,5,10 No study, to our knowledge, has evaluated if a positive family history also has an influence on clubfoot severity.
The purpose of our study was to further investigate how laterality, sex and family history influence initial severity and treatment.
Materials and methods
A retrospective analysis of prospectively collected data was carried out. Idiopathic congenital clubfeet consecutively treated at our institution from February 2016 to June 2018 were enrolled in this study.
Postural deformities, non-idiopathic clubfeet and patients older than four months at presentation or that had undergone any previous intervention (surgery, physiotherapy or casting) were excluded from the study. Infants presenting feet with mild deformity (grade I Dimeglio score (DimS)) were excluded.
Severity score was determined at presentation using both DimS 11 and Pirani score (PirS). 12 For DimS, midfoot rotation, hindfoot varus, forefoot adduction and equinus are each given 0 to 4 points based on reducibility on the relative plane; pejorative items (posterior crease, medial crease, cavus and muscular abnormality) are each scored as 1 if present and 0 if absent. The sum of these elements constitutes a total on a 20-point scale, where a higher score indicates a more severe deformity.
For PirS, six different features of clubfoot deformity (posterior crease, emptiness of the heel, rigidity of equinus, medial crease, curvature of the lateral border of the foot and reducibility of the lateral part of the head of the talus) are evaluated. Each item is given a score of 0 (no abnormality), 0.5 (moderate abnormality) or 1.0 (severe abnormality) and summed to produce a final score between 0 and 6, where 6 is the most severe score.
In all cases, treatment was performed according to the method described by Ponseti, 13 including weekly sessions of manipulation and casting, percutaneous Achilles tenotomy if needed and foot abduction orthosis. Achilles tenotomy was performed if the foot could not be dorsiflexed to 15° once complete abduction was achieved. Evaluations and treatment were performed by orthopaedic surgeons experienced with the scores and Ponseti method.
Sex, laterality (uni-/bilateral), family history, number of casts required for correction (excluding post-tenotomy cast) and need for tenotomy were analyzed.
Family history was considered positive (FH1) when a first-degree relative was affected or had been treated for clubfoot deformity, regardless of the severity or treatment performed. An additional analysis was performed considering positive family history (FH2) if a first or second-degree relative was affected, as reported by the family.
For infants with bilateral clubfoot, only the foot with more severe deformity was included in the analysis for that patient, to reduce the statistical error of considering two feet of each patient as independent.2,14
Statistical analysis
Correlations of laterality, sex and family history, respectively, with severity scores (PirS and DimS), number of casts and need for tenotomy were evaluated using parametric or non-parametric tests, as appropriate. In addition to the analysis using the raw PirS and DimS, an additional analysis was performed by dividing the feet into categories according to PirS (‘very severe’ if ≥ 5 points, ‘less severe’ if ≤ 4.5 points) and DimS (‘moderate’, grade II, 6 to 10 points; ‘severe’, grade III, 11 to 15 points; ‘very severe’, grade IV, 16 to 20 points) as previously described2,6,7 and using the chi-squared analysis or the Fisher exact test, as appropriate. A p-value < 0.05 was considered significant.
In bilateral feet, correlation between the right and left foot in terms of initial severity scores (DimS and PirS), number of casts and need for tenotomy was analyzed using Pearson correlation coefficient.
Results
In all, 97 infants (81 male, 16 female) with idiopathic clubfoot met the criteria and were included in the study. The deformity was bilateral in 42 cases, unilateral in 55 (28 right, 27 left). A positive family history (FH2) was reported in 19 cases (19.6%) and in 11 cases a first-degree relative was affected (FH1). Mean age of patients at presentation was 26 days (7 to 119).
Mean severity score at presentation for all patients was 5.1 points (2.5 to 6; severity classification: 25 less severe, 72 very severe) using PirS and 12.4 points (7 to 16; 18 moderate, 68 severe, 11 very severe) using DimS. A mean of 4.4 casts (2 to 8) were performed. Achilles tenotomy was performed in 92 (94.8%) infants.
Laterality
Bilateral cases showed significantly higher PirS and DimS (Fig. 1) at presentation, number of casts performed and rate of tenotomy performed in comparison with unilateral cases. Data and p-values are reported in Table 1. Using severity categories, the difference of distribution was significant both for PirS (p = 0.006) and DimS (p = 0.024); there were 1.2-times as many expected bilateral patients diagnosed with ‘very severe’ deformity according to PirS and there were 1.5-times as many expected bilateral patients diagnosed with ‘very severe’ deformity according to DimS.
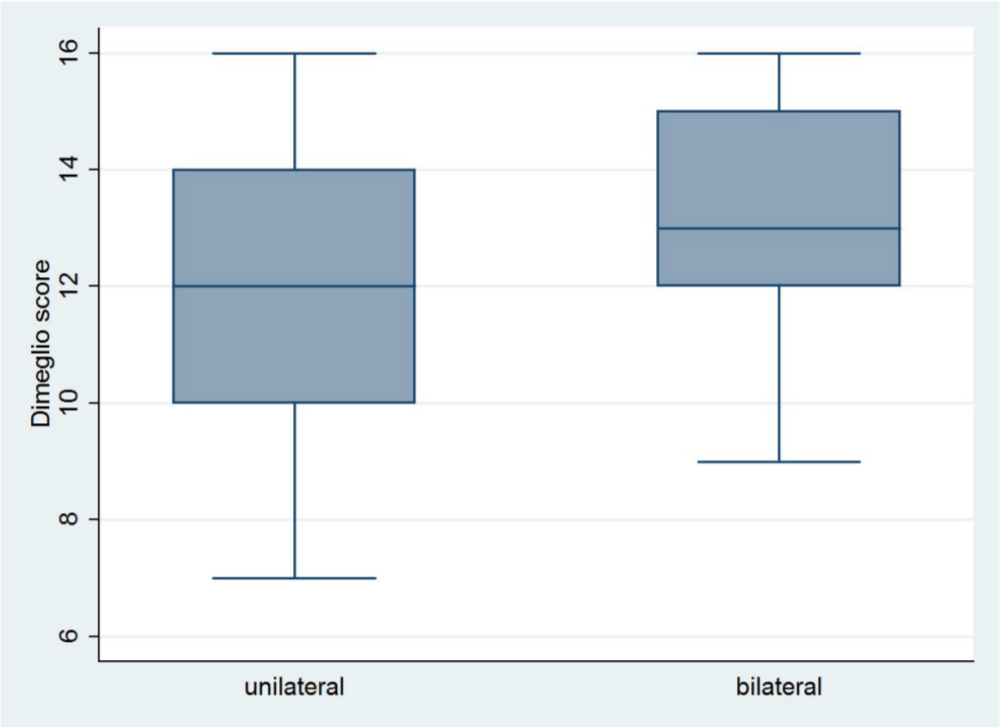
Box plots represent the distribution of Dimeglio scores for bilateral versus unilateral cases. The median is shown by the horizontal line in each of the boxes, the bottom and top of each box represent the 25th and 75th percentiles, respectively.
Influence of laterality (uni- versus bilateral) on clubfoot severity and treatment: results of our study and revision of the literature
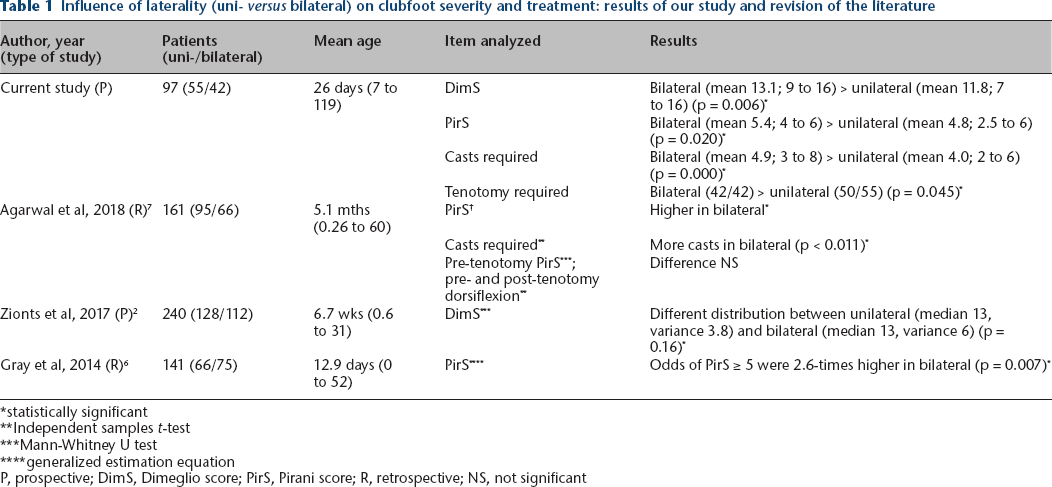
statistically significant
Independent samples t-test
Mann-Whitney U test
generalized estimation equation
P, prospective; DimS, Dimeglio score; PirS, Pirani score; R, retrospective; NS, not significant
Sex
Male and female patients did not show significantly different DimS, PirS and distribution according to severity categories at presentation. Number of casts and rate of tenotomy performed were not significantly different as well. Data and p-values are reported in Table 2.
Influence of sex on clubfoot severity and treatment: results of our study and revision of the literature
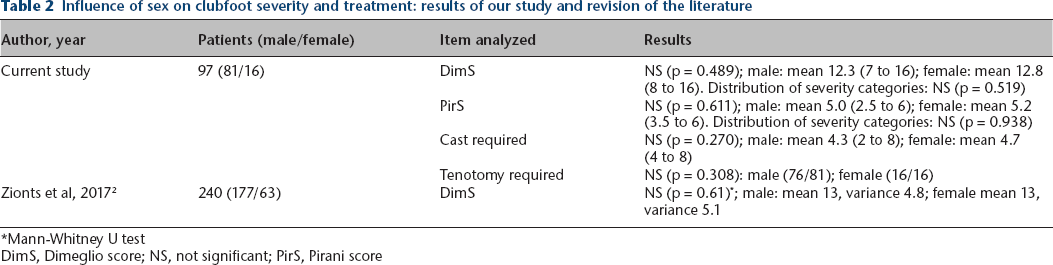
Mann-Whitney U test
DimS, Dimeglio score; NS, not significant; PirS, Pirani score
Family history
Both DimS and PirS were higher in patients with a positive history (Fig. 2) but this difference was not significant; mean PirS was 5.3 (3 to 6) for patients with a positive FH2 and 5.0 (2.5 to 6) for patients with no family history for clubfoot (p = 0.185). When only FH1 was compared with infants with no family history, the difference was also not significant (p = 0.176). Mean DimS was 12.8 (7 to 16) for FH2 and 12.3 (7 to 16) for infants with no family history, with a non-significant difference (p = 0.339). The difference was also not significant for FH1 (p = 0.110). In addition, the analysis of distribution of severity showed a higher ratio of very severe deformity in patients with positive family history (for example, 1.4-times as many as expected patients according to DimS) but the difference was not significant (p = 0.771). A mean of 4.7 casts (2 to 8) were performed on infants with a positive FH2 and a mean of 4.3 (2 to 7) in cases of negative family history; the difference was not significant (p = 0.226). In all, 18 out of 19 (94.7%) cases with a positive FH2 underwent tenotomy, in comparison with 74 out of 78 (94.9%) cases with no family history; the difference was not significant (p = 0.981). The difference was not significant for FH1 (p = 0.442) as well.
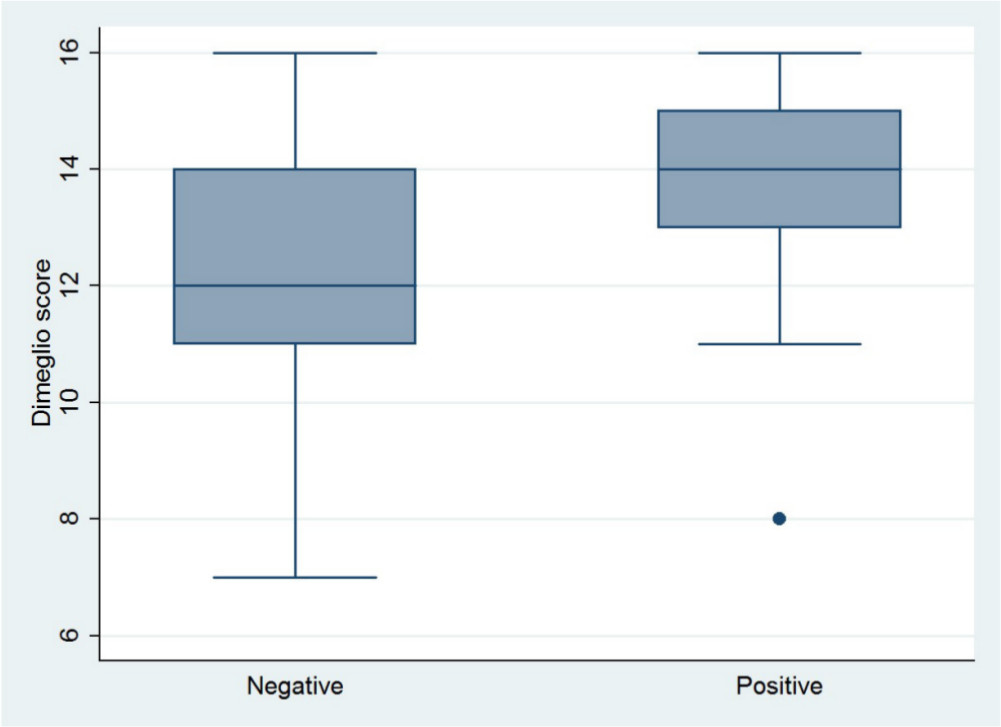
Box plots represent the distribution of Dimeglio scores for patients with positive versus negative family history. The median is shown by the horizontal line in each of the boxes, the bottom and top of each box represent the 25th and 75th percentiles, respectively.
Right versus left foot in bilateral cases
Initial severity in the right and left foot of each patient was highly correlated using DimS (Fig. 3), DimS grade and PirS. Data and p-values are reported in Table 3.
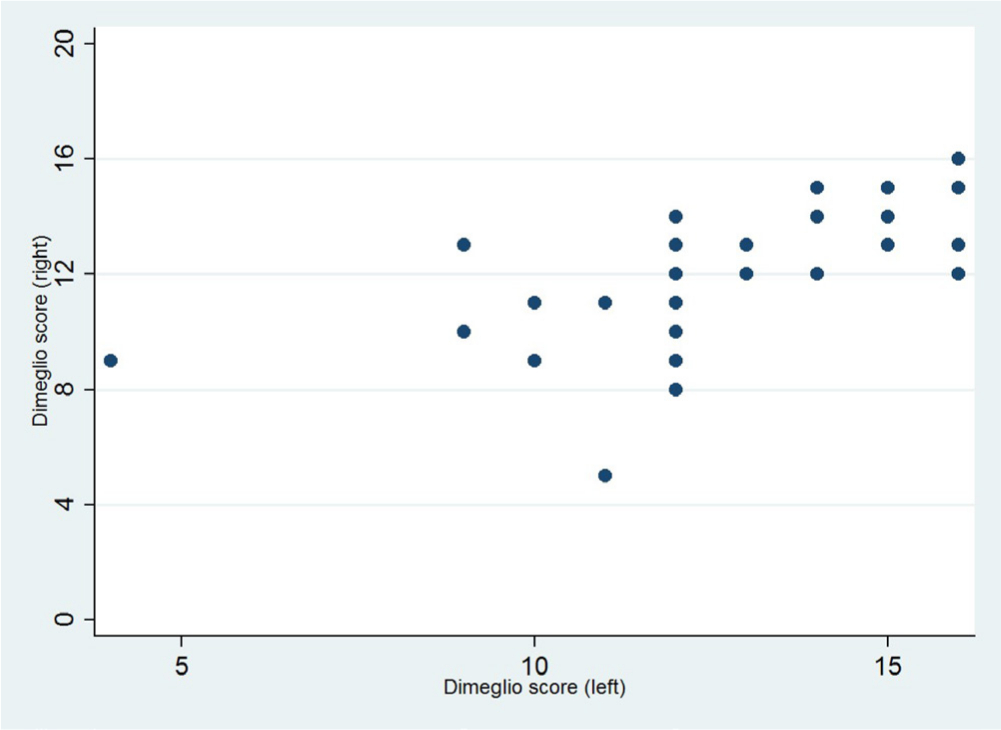
Correlation between initial Dimeglio scores of right and left feet in bilateral cases.
Correlation between right and left foot in bilateral cases: results of our study and revision of the literature
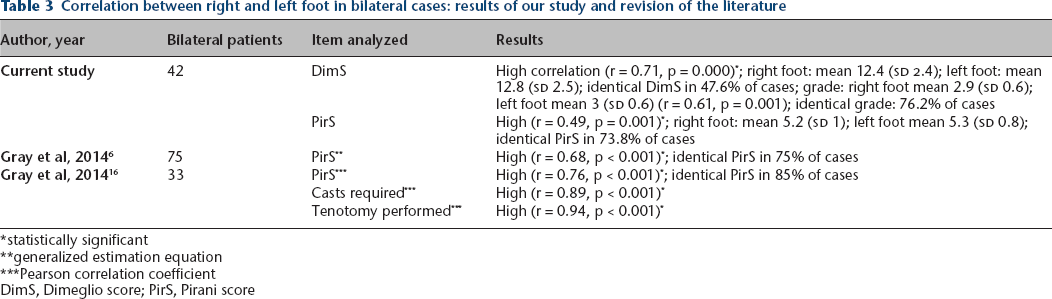
statistically significant
generalized estimation equation
Pearson correlation coefficient
DimS, Dimeglio score; PirS, Pirani score
There were only two out of 42 infants in which a different number of casts was performed in left and right foot; the deformity in these two feet was very different, so the surgeon decided to start casting only in the more severe foot and then continued simultaneously. All the other cases (95.2%) underwent the same number of casts on both sides. A total of 41 out of 42 (97.6%) underwent bilateral Achilles tenotomy; only one infant tenotomy was performed on one foot and not on the other.
Discussion
Patterns of inheritance and expressivity of idiopathic clubfoot are complex and still not completely clear; the condition is unlikely due to mutations within a single gene but instead is multifactorial and/or polygenic in nature.3,5 Subgroups with different phenotypes and clinical features may reflect different pathogenic mechanisms.
Traditionally, unilateral/bilateral clubfeet and male/female individuals have been considered to have similar characteristics and have been included in the same group for scientific research. 13 In recent years, the use of more reliable evaluation scores (DimS and Pirs) and the worldwide diffusion of treatment by the Ponseti method with its reproducible short-term results (full correction achieved in most cases), have permitted a better understanding of differences in initial presentation and response to treatment of different subgroups.
Laterality
Clubfoot severity seems to be influenced by laterality. Some authors have postulated an increased genetic load 8 or a greater treatment-resistance in bilateral cases,2,15 but these studies did not provide evaluation scores to support their hypothesis.
Evidence on phenotypic discrepancy according to laterality was provided by recent studies (Table 1). Zionts et al 2 found no differences in terms of severity but reported a larger range of severity in bilateral cases; the ratio of bilateral patients was higher among those with moderate (DimS grade II) or very severe (DimS grade IV) deformities compared with those with severe deformities (DimS grade III) (p < 0.01).
Gray et al 6 used the PirS and reported bilateral cases to be more severe than unilateral feet; the odds of being very severe (≥ 5 PirS points) were 2.6-times higher in bilateral cases compared with unilateral cases (p = 0.007).
Agarwal et al 7 also reported that idiopathic bilateral clubfeet were more severe at initial presentation using PirS and that they required a greater number of corrective casts; instead, the correction (pre-tenotomy PirS, pre- and post-tenotomy dorsiflexion) was similar in the two subgroups.
We have found similar results both in terms of initial severity, number of casts and tenotomy required. Some discrepancies among studies can be explained by methodological differences (prospective versus retrospective; statistical models used for taking into account the potential correlations between feet in bilateral cases) but the finding of different behaviour according to laterality is consistent.
In addition, bilateral feet were found to have another clinical feature: correlation between right and left foot, both in terms of severity and treatment required, that can be hypothesized to be related to genetic mechanisms of regulation of expressivity. It should be stressed that these findings could have been influenced by several areas of bias, 16 for example, without blinding of feet (which is not feasible), assessment bias may influence the score assigned to each foot in bilateral cases. The number of casts is also influenced, since even in cases of different response to casting on the two sides, casting is best not interrupted on the less severe foot until tenotomy or brace application; also the decision to perform or not tenotomy on the less severe foot is likely influenced, in doubtful cases, if the more severe foot is undergoing tenotomy. Similar findings have been previously reported and also have important statistical implications for trials in which data from bilateral clubfoot cases are included. Researchers should be cautioned against using data from the right or left foot as independent data for statistical analysis. 16
Sex
Some authors8,9 have suggested that female patients may represent a more severe clubfoot phenotype since a greater rate of posteromedial release was required, 9 but did not report initial severity scores to support this hypothesis. A prospective comparison of initial severity (using the DimS) according to sex was recently performed by Zionts et al 2 on a population of 240 infants and no difference was found (Table 2). Our results were similar, with no difference in terms of initial severity (using both PirS and DimS) and treatment required.
The higher clubfoot prevalence in male cases has been related to a postulated sex-related threshold effect, where female cases would require a greater number of abnormal genes to manifest the deformity and, if affected, would be more likely transmit the condition to their offspring. 2 According to our findings, this supposed higher genetic load would not be associated with an increased severity.
Family history
Our study is the first, to our knowledge, evaluating family history's influence on severity. Higher initial severity scores and a higher ratio of patients with very severe deformity were found in patients with positive family history with respect to patients with negative history, but these differences were not statistically significant. It is possible that larger samples could have detected some significant discrepancy.
The strength of this study is that data were collected prospectively and consecutively. Mean age at presentation was low (26 days), similar to other reports (12.9 days 6 and 6.7 weeks 2 ). Agarwal et al 7 included older children (up to 84 months) where initial severity could have been influenced by unreported treatment or walking.
Both DimS and PirS were used for evaluation of initial severity, whereas previous authors used just one of them.2,6,7 These scores have been reported to have high reliability and to be correlated. Yet, Fan et al 17 reported poor score correlation in the case of mild and very severe clubfoot deformity, so we considered it more appropriate to use both; nevertheless, results were comparable.
The main limitations of our study are the small number of patients and the fact that our sample shows some differences of distribution with respect to the general population: in particular, the male to female ratio was 5.1:1 (proportion of bilateral cases and of positive family history corresponded to the general population). Yet, our sample included consecutive cases of a given period.
Analysis of the family history of clubfoot was more reliable when first-degree relatives were included; inclusion of second-degree relatives based on a family report has the potential bias of a false-positive included and missing data. For this reason, separated analysis was performed but results were comparable. Finally, longer follow-up would be required to detect differences in prognosis or relapse among subgroups.
In conclusion, this epidemiological study has confirmed the different behaviour (initial severity, number of casts and tenotomy required) of bilateral and unilateral cases reported by previous studies. Bilateral cases are more severe and show similar features in their right and left foot. They could, therefore, represent different clubfoot entities 6 or the result of different pathogenic mechanisms, likely on a genetic basis. Conversely, no statistically significant difference was found with regard to sex and family history.
Footnotes
Acknowledgements
The authors wish to thank Dr Salvatore De Masi (Clinical Trial Office, AOU Meyer, Florence) and Professor Giancarlo Bettuzzi for statistical analysis.
CB: Data acquisition, Analysis and interpretation of data, Ideation and writing of the manuscript.
CNA: Data acquisition, Critical revision of the manuscript.
GL: Data acquisition, Critical revision of the manuscript.
AZ: Data acquisition, Critical revision of the manuscript.
ML: Data acquisition, Analysis and interpretation of data, Ideation and writing of the manuscript.