
Abstract
Abstract
Purpose
The aim of the study was to evaluate predictable parameters with the highest sensitivity used in the diagnosis of children septic shoulder arthritis.
Methods
All children treated in our paediatric orthopaedic hospital between 2000 and 2017 with intraoperative verified septic arthritis of the shoulder were included in this retrospective study. Diagnostic procedures e.g. ultrasound, MRI, radiograph or blood samples as well as typical clinical symptoms were evaluated as predictable parameters for septic shoulder arthritis in paediatric patients. Descriptive statistics as well as sensitivity analysis were performed.
Results
In all, 25 children, 20 boys and five girls, aged from eight days to 15 years, were included for further statistical analysis. All parameters included were tested for sensitivity with binomial confidence intervals (Cis) of 95%. Predictive parameters with highest sensitivity were pseudo paralysis (100%, CI 0.86 to 1.00) and C-reactive protein (CRP) (96%, CI 0.79 to 0.99) superior to temperature (52%, CI 0.3 to 0.73), white blood count (11%, CI 0.01 to 0.34), radiograph (21%, CI 0.04 to 0.50), ultrasound (71%, CI 0.47 to 0.88) or MRI (100%, CI 0.78 to 1.00).
Conclusion
The diagnosis of a septic arthritis of the shoulder in children can be challenging for the clinician and especially for the resident doctor. Clinical symptoms such as pseudo paralysis and increased CRP level must be considered as predictive markers not to delay further diagnostics and treatment.
Level of Evidence
IV
Keywords
Introduction
Septic arthritis of the shoulder associated or not with osteomyelitis in children represents a constrained group of joint infection that is sometimes poorly diagnosed. The diagnosis and the treatment should not be delayed, due to the late sequalae humeral shortening and inferior subluxation of the shoulder. There is only limited data available regarding an algorithm or the most predictive parameters that can help in diagnosing the septic shoulder in children.
No matter how appropriate it is to compare the septic shoulder with the septic hip or knee, in practice, we frequently observe that the same criteria does not apply regarding the shoulder.
Differential diagnosis includes the congenital brachial plexus palsy, the arthrogryposis and fracture of the proximal humerus or clavicle and cerebral palsy. 1
In newborns it is more common to find a post-traumatic upper limb palsy than an infection. 2 It is uncommon to have a true nerve palsy associated with an infection such as osteomyelitis, and the changes in the electromyography appear to be rare. 3
In case of a traumatic palsy of the upper extremity, the diagnosis should not be difficult regarding fracture of the clavicle or proximal humerus. The challenges are the newborns with shoulder pseudo palsy and elevated C-reactive protein (CRP), but without fever or pathological changes at the point of imagistic examination.
The aim of this article is to determine the most frequently encountered parameters that could help in diagnosing a septic shoulder and simultaneously to determine what kind of clinical or imagistic parameters are most useful in the diagnosis. We tried to find an accurate algorithm of judgment, particularly among small children, without signs of fever or with negative imagistic results.
Material and methods
Data collection and patients
In this retrospective study we performed a data search in the hospital data information system for all children that were treated in our hospital (specialized for paediatric orthopaedics) between 2000 and 2017 with the diagnosis of a septic arthritis of the shoulder due to primary septic arthritis or osteomyelitis of the proximal humerus due to secondary arthritis. Only children with an intraoperative verified septic arthritis or osteomyelitis of the proximal humerus have been further analyzed (verified meaning that in all cases pus or purulent secretions within the joint or in the bone were found). We included infections with negative and positive cultures. We included patients under the age of 17 years of age.
Algorithm of treatment and diagnostics in our hospital
If a child presents and there is suspicion of septic arthritis of the shoulder with or without osteomyelitis of the proximal humerus, with the incapacity to elevate the upper extremity and/or with signs of a pseudoparalysis, regardless of whether the child presents fever or not, we first of all examine the upper extremity and then we take a blood test, to check if the child has elevated CRP, leukocytes or erythrocyte sedimentation rate (ESR). Meanwhile, our radiologist does an ultrasound of the shoulder. If the child has a pseudoparalysis of the upper extremity and an elevated CRP and a positive ultrasound, we consider septic arthritis of the shoulder. If the child is having a negative ultrasound, we consider MRI diagnostics and reevaluation.
Clinical parameters and diagnostics
The data collected was categorized by age, sex, affected side, days between the onset of the symptoms and presentation in our hospital, clinical manifestation, temperature, previous infection, antibiotic use, blood tests and imagistic exams. We also included children that were examined with an MRI in other hospitals. All MRI results were re-examined by our surgeons and radiologist colleagues.
Fever was defined as the rectal or ear measured temperature equal or higher than 38°C.
We used different values for white blood cells, depending on the patient age.
We used the term of pseudoparalysis for all motor function deficits such as decreased range of movement of the upper limb, relieving posture, weakness of the abductors and external rotators and/or the impossibility to raise the upper limb or to use it properly.
With regards to previous infections, we included the children that where admitted with previously neonatal infections, due to the mother, like streptococcal group B infections or infections like otitis, rhinitis, bronchitis and other respiratory tract infections.
Positive MRI included signs of bone involvement like periosteal reaction, joint effusion with or without signs of destruction or osteolytic changes in the proximal humerus.
Positive ultrasound included liquid in the shoulder joint, signs of bursitis or soft-tissue modification, periosteal reaction, signs of thickening of the synovial capsule, while positive radiograph included periosteal reaction or an osteolytic lesion.
Statistical analysis
We analyzed our collected data with the binomial confidence intervals, testing the sensitivity of each factor with a confidence level of 95%, resulting in a proportion percentage defined as a mean probability of confidence interval (CI).
Results
The data collected included 25 children, 20 boys and five girls, with a mean age of 34.8 months (8 days to 15 years), between 2010 and 2017.
The patients were stratified by age into three groups: six children between 0 and four weeks, 12 children between four weeks and three years old and seven children between three and 15 years old. The right side was affected in 15 cases and the left side in ten cases. We documented previous infections in nine cases.
Out of 25 children, 12 presented a high temperature (general sensitivity of 52%, CI 0.30 to 0.73).
Out of six children with ages between 0 and four weeks, four children presented normal temperature (one child had high temperature and one value was unknown).
Out of 12 children with ages between four weeks and three years, four children presented normal temperature, seven children had a fever and one child had missing information.
In the group aged three years to 18 years, three cases out of seven had normal temperature and four had fever.
All 25 cases were showing signs of shoulder pseudoparalysis, such as described above (Cl 0.86 to 1.00). A total of 18 in the 25 presented pseudoparalysis combined with other signs such as pain or tenderness, as shown in Table 1 (72% sensitivity, Cl 0.50 to 0.87).
Parameters used to determine the most predictive factor that appear in a shoulder septic arthritis.
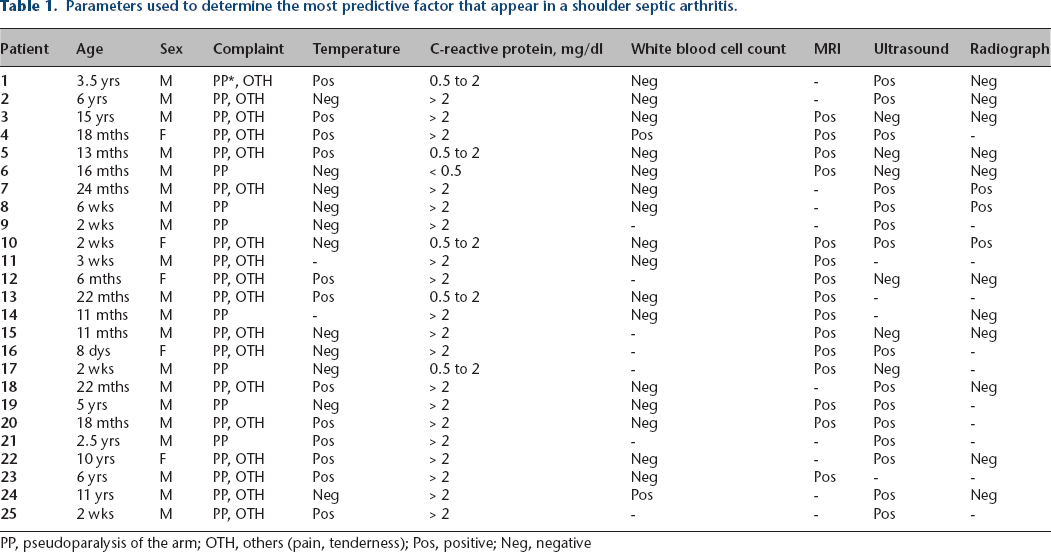
PP, pseudoparalysis of the arm; OTH, others (pain, tenderness); Pos, positive; Neg, negative
The average white blood cell count (WBC) was 12.40 × 103 /µl (5.93 to 28.00). WBC sensitivity was 11% (CI 0.01 to 0.34). We had WBC cut-offs between 5.00 to 20.00 × 103 /µL for six patients under one year old and 5.00 to 18.00 × 103 /µL for one patient (one month old), 5.50 to 15.00 × 103 /µL for two patients (2.5 to 3.5 years old), 5.00 to 14.00 × 103 /µL for another two patients (five to six years old), 4.00 to 10.00 × 103 /µL for one patient (15 years old), 6.00 to 17.00 × 103 /µL for nine patients (11 months to two years old) and 4.50 to 13.00 × 103 /µL for three patients (six to 11 years old).
In all, 24 out of 25 patients had an elevated CRP value (sensitivity of 96%, Cl 0.79 to 0.99).
We categorized the CRP values into three groups: lower than 0.5 mg/dl defined as normal, between 0.5 mg/dl and 2 mg/dl defined as elevated and higher than 2 mg/dl defined as high elevated. The mean value of CRP at admission was 5.4 mg/dl (0.4 mg/dl to 24.2 mg/dl, normal < 0.5 mg/dl).
A total of 19 children had a CRP value higher than 2 mg/dl (mean value 6.6 mg/dl), five children between 0.5 mg/dl to 2 mg/dl (mean 1.5mg/dl) and one child lower than 0.5 mg/dl.
Normal radiographs were found in 11 cases and osteomyelitis signs with osteolysis in three cases (sensitivity of 21%, Cl 0.00 to 5.00).
The ultrasound was positive in 15 cases (71%) with 95% Cl 0.47 to 0.88 and negative in six cases. Ten ultrasound results had only signs of arthritis without bone involvement, two had only signs of osteomyelitis like periosteal elevation without arthritis and three had signs of arthritis with osteomyelitis. Six ultrasounds were negative and four were missing.
MRIs was done in 15 cases; all cases were positive (60%). A total of 11 cases demonstrated only effusion, meanwhile four cases had evidence of osteomyelitis with bone edema and periosteal reactions, associated also with effusion.
Intraoperatively we confirmed 18 cases of isolated septic arthritis without involvement of the proximal humerus metaphysis and seven cases of osteomyelitis associated with septic arthritis of the shoulder.
Regarding the microbiological examination, 36% of intraoperative culture was positive and 64% negative. Regarding the pathological agent, we found three cases with Staphylococcus aureus, three cases of Streptococcus Beta-hemolytic group B, two cases of Staphylococcus epidermidis, one case of Neisseria meningitidis and 16 negative cases.
Out of 25 cases, eight patients (32%) received antibiotic therapy before the operation and 14 cases (56%) did not. Postoperatively, we commonly performed therapy with Cefuroxime intravenously for two weeks, followed by oral therapy for four weeks. In one case first we performed a therapy with Tazobactam and Gentamicin, due to a simultaneous paediatric infection.
We performed 13 arthrotomies with joint lavage and drainage in 17 cases. In four cases out of these 17 patients we also added a Sulmycin implant for ten days in the proximal metaphysis of the humerus. In seven cases we performed an arthroscopy of the shoulder with joint lavage and in one case out of these seven, we had to reopen the joint and perform an arthrotomy with joint lavage the next day because of an increase in inflammation signs. In only two cases we did a shoulder arthrocentesis primary, followed also by an arthrotomy of the joint the next day.
Discussion
In contrast to septic hip arthritis or osteomyelitis, they are fewer reports in the literature about the septic shoulder, maybe because the differential diagnosis in the septic shoulder is easier when it is traumatic or because there is not a pathology like transient synovitis of the hip that mimics septic arthritis in the shoulder joint. It is difficult to establish an algorithm, especially among small children.
It is not clear which parameters are most predictive for septic arthritis of the shoulder in children. Possible predictive factors are elevated CRP, leukocytes or ESR, positive ultrasound, pseudoparalysis and fever; we observed that pseudoparalysis and elevated CRP are the most encountered.
Bono et al 4 found in their study that the children younger than three months are least likely to present a high temperature, because they may not be able to have an appropriate immune response to infection. In our study, we had in the youngest age group (0 to four weeks, n = 6) four children with normal temperature. In the age group three to 17 years we also had nearly 50% without fever. Only in the age group four weeks to three years did more than 50% present with fever.
The results show that fever is not a high-level predictive parameter, only 12 from 25 children presented an elevated temperature. CRP otherwise showed positively in 24 cases out of 25. Pseudoparalysis was present in all children in this case series.
The challenging cases are the cases without fever and with mild symptoms or blood samples. They are more likely to be sent home from the emergency department. These cases could be examples of infection with Kingella kingae septic arthritis. Even if we had no positive cases with Kingella kingae at the microbiological examination, we considered the possibility. Williams et al 5 published a study of 27 cases of septic arthritis with poor symptoms and blood results, and all tested positive for Kingella kingae at polymerase chain reaction (PCR) assays. They also had two cases of Kingella kingae septic shoulder.
In our study we did not find any cases of Kingella kingae infection, but we had 16 cases with negative culture. The blood culture was made after standard laboratory tests and not PCR assays. We cannot corelate these cases with Kingella kingae septic arthritis even if the mild symptoms without fever in more of 50% cases could raise the possibility.
Pseudoparalysis due to a septic arthritis should be distinguished from brachial plexus palsy as a differential diagnosis in a newborn. It should be considered that a true paralysis of the upper extremity due to brachial plexus palsy needs to be diagnosed by nerve conduction exams 6 and focused neurological clinical evaluation, exams that are difficult to make on a newborn and for this reason it is sometimes preferred to postpone it.
The review of Li et al 7 of 52 cases with septic arthritis in the neonate revealed a percentage of appearance of 32.1% regarding the shoulder, with pseudopalsy as the earliest sign in 50% cases. In their study, children that fulfilled three criteria out of five were diagnosed with septic arthritis. Concerning the criteria, we also consider that symptoms of infection such as fever, tenderness of the join, pain and palsy of the arm, are important clinical signs, which should raise concern and lead to proper imagistic examination. Besides imagistic (ultrasound, CT or MRI) and blood samples (WBC, ESR and CRP) they took radiographs and joint aspiration as criteria.
We used MRI in 15 cases from 25 (60%) and all cases presented positive results. Despite the positive results, the disadvantage is that the MRI was not always done on the same day as the presentation or the ultrasound examination.
Ernat et al 8 observed a higher accuracy of the MRI compared with other methods of diagnosis related to the osteoarticular infections. In their case, they used MRI as a preoperative method of diagnosis in 19 out of 22 cases and in all cases, MRI showed a positive result.
Belthur et al 9 described that when compared with septic arthritis of the hip, the infections of the glenohumeral joint need significant longer time from the onset of symptoms and, they present a higher rate of surgical intervention.
Solebo et al 10 published the case of a neonate who presented with decreased range of movement and pain in the arm, without fever, which was misdiagnosed as Erbs palsy and referred for physiotherapy.
In the younger age groups, due to an improperly ordinary immune response, the probability that the only objective sign for septic shoulder to be a palsy of the arm is quite high. Particularly because the osteomyelitis of the humerus at neonatal age is often presented as an Erbs palsy. 6
Montgomery et al 11 showed which factors can be identified in helping diagnose the concurrent infections earlier. They show the importance of using advanced imaging like CT scans, bone scans or/and MRI, particularly in children younger than four months or children with shoulder septic arthritis.
In cases of an advanced imagistic examination such as MRI, the small child must receive anesthesia, a fact that makes the decision harder. This decision must be carefully discussed with parents that sometimes are anxious about this. As an advantage in cases of confirmation of the diagnosis, the anesthesia will be needed only once, and the child can be operated on immediately following MRI.
The probability that septic arthritis is evolving from osteomyelitis of the proximal humerus in the younger age group is very high, as was shown in the study of Schmidt et al 12 in their review of the septic shoulder. More than half of their patients presented osteomyelitis of the proximal humerus.
To sum up, we found that the two most reliable criteria are pseudoparalysis of the arm and elevated CRP. The ultrasound was almost as accurate as the MRI, but the MRI was not always performed on the same day of the presentation.
We strongly recommend considering as at-risk young children with a moderate or high level of CRP, pseudoparalysis of the arm and mild symptoms. Fever should also be treated as a complementary factor.
Limitations
Our study is retrospective, and it was confronted with lack of data due to poor documentation. We could not determine the results of the ESR because this test was sometimes made separately in the emergency unit and not documented consistently on the observation chart. Another limitation is the fact that not all the children received an MRI, and the MRI was sometimes made after a few days of delay. The delay in performing the MRI or the decision to operate were made subjectively and by more than one doctor, as were the ultrasounds and the interpretation of the images.
Conclusion
Based on the presented data, we think that increased CRP and pseudoparalysis of the shoulder should be taken into consideration as the most accurate predictive factors for septic shoulder in children. A moderate increase of CRP should be noted and further observed and the it can be decided if the patient needs additional advanced imagistic examination. Other clinical parameters such as temperature, leukocytes or ESR must be considered, but not related directly with the septic arthritis or at least not used as an exclusion factor.
Overall isolated septic arthritis in association with osteomyelitis in small children can be challenging, and reevaluation the child after one to two days clinically, with imagistic techniques and with blood samples should be considered.
Footnotes
CI: Corresponding author, Active implication on the structure of the article and in the writing, Statistical analysis of ideas and factors to be determinate, Intellectual input, Final correction and suggestions before submitting.
FFF: Part of the leader team, Great experience in septic joint infections, Main senior supervisor, Intellectual inputs, Ideas about the researched theme and about the study.
GB: Statistical data, Ideas about the best approach for statistical analysis and suggestion about different statistical programmes that could be used, Objective expertise the data collected and the significance of the studied patients.
TW: Intellectual input, Final correction such as suggestions for organising the data, Structuring the question and the researched data.
OH: Main senior supervisor, Directly monitoring the patient data and the factors examined, Significant intellectual input, Correcting the manuscript and improving the structure.