
Abstract
Abstract
Purpose
A mild delay in gross motor milestones and walking age has been reported in infants with clubfoot. The influence of different treatments on motor development has been poorly investigated. Some parents and physical therapists express concern that the Ponseti method (PM) and its constraints (abduction brace, casts) would affect development more than the French physical therapy method (FM) due to greater immobilization and lesser stimulation.
The purpose of this study was to evaluate achievement of three motor milestones (pull-to-standing, cruising and independent walking) in two groups of clubfoot patients treated at two experienced institutes respectively with the PM and FM.
Methods
In all, 52 consecutive infants (full-term at birth, mean age at beginning of treatment 24.3 days (sd 10), mean Dimeglio score 12 (sd 3.4)) were prospectively enrolled (26 patients per centre) and followed up to walking age recording milestones.
Results
The two groups were not different in terms of age at the beginning of treatment (p = 0.067) and rate of tenotomy. Age at tenotomy was significantly lower in the PM group (p = 0.000). Severity (p = 0.004) and number of bilateral cases (p = 0.012) were higher in the PM group. A non-significant difference was found for age of achievement of pull-to-standing (p = 0.109), cruising (p = 0.253) and independent ambulation (p = 0.349) between the two groups. Overall, milestones were achieved approximately two months later than normal population. Sex, severity, laterality and need of tenotomy were not found to significantly influence milestones.
Conclusion
Our results confirmed that infants with clubfoot are expected to have a minimum delay in motor development. Infants treated with the PM and those treated with the FM did not show significant differences in gross motor milestones achievement at walking age.
Level of Evidence
Level II – Prospective comparative therapeutic studies
Introduction
Congenital talipes equinovarus or clubfoot is one of the most common congenital birth defects, with a reported incidence of one to two per 1000 newborns. 1 The aetiology is not completely understood and is considered multifactorial, with a combination of environmental and genetic factors (mostly genes related to limb patterning and development of muscle and blood vessels) supposed to play a role in the pathogenesis. 1
In about 20% to 25% of cases, the deformity is associated with syndromic conditions (distal arthrogryposis, congenital myotonic dystrophy, myelomeningocele, amniotic band sequence or other genetic syndromes such as trisomy 18 or chromosome 22q11 deletion syndrome) or is secondary to an underlying pathology.1,2 This pathology is not always evident at birth; in some cases the pathology is suspected and can be diagnosed in the first years of growth, for example in case of repeated relapses or delay in motor development.3,4
At the beginning of treatment, many parents are concerned about possible delay in gross motor development of their child, which could be due to clubfoot pathology or to the treatment performed (immobilization, lack of stimulation, surgery).
A few papers have demonstrated a minimum delay in clubfoot patients5–7 but how different treatments may influence gross motor development has been poorly investigated. Among conservative methods for treatment that have gained worldwide diffusion, the Ponseti method (PM) and the French physical therapy method (FM) share similar principles of trying to limit extensive surgery as much as possible, but with different means (serial manipulation/casting, percutaneous Achilles tenotomy and foot abduction orthosis in the former, physiotherapy, taping and splinting in the latter).
Some parents and physical therapists express concern that the PM with its constraint (abduction brace, casts) would affect development more than the FM due to greater immobilization and lesser stimulation. This is especially true in some regional areas where the FM was traditionally applied before the wide diffusion of the PM.
The purpose of this two-institution study was to evaluate gross motor milestones in two groups of clubfoot patients: the first group was treated according to the FM at one institution (group FM); the second group was treated according to the PM in a different centre (group PM). A comparison between the two groups and with data reported in the literature for a non-affected population was performed.
Materials and methods
We performed an analysis on prospectively collected data from two centres. Infants consecutively treated for idiopathic congenital clubfeet between January 2011 and December 2015 at two institutes were enrolled.
Inclusion criteria were: full-term (gestation ≥ 37 weeks), no previous clubfoot treatment and age ≤ 90 days at beginning of treatment. Patients with postural deformities, benign feet (Dimeglio grade I) and non-idiopathic clubfoot were excluded.
All infants with conditions that could have determined delay of motor development were excluded from the analysis: orthopaedic conditions requiring physiotherapy or immobilization (torticollis, hip dysplasia, etc), lack of respect of the treatment protocol until the time of independent ambulation or patients who underwent casts or interventions for relapses before independent ambulation.
Severity of the deformity was determined at presentation using Dimeglio score (DimS):8 midfoot rotation, hindfoot varus, forefoot adduction and equinus were each given 0 to 4 points based on reducibility on the relative plane; pejorative items (posterior crease, medial crease, cavus and muscular abnormality) were each scored as 1 if present and 0 if absent. The sum of these elements constitutes a total on a 20-point scale, where a higher score indicates a more severe deformity. This score has been shown to have a high interobserver reliability. 8 The evaluation was performed by orthopaedic surgeons or physical therapists experienced with the score.
For infants with bilateral clubfoot, the more severe of the two scores was used for the analysis. 7
Intervention protocols
Treatment was performed differently at the two institutions according to local protocols by teams with large experience in managing clubfoot with their respective method.
At the first institute patients were treated according to the FM, including physiotherapy, taping and splinting to maintain correction. For this method, different descriptions and modifications have been reported. 9 The protocol used in this study, introduced in the regional area of the institute after formal training of the orthopaedic and physiotherapist staff by Dr Raphael Seringe in 2004, involved initial intensive physiotherapy about three times a week by an experienced (on average ten years of practice in the field of clubfoot, 25 patients treated per year) physical therapist; at each session, gentle mobilization and stretching of contracted tissues, stimulation and strengthening of weakened muscles were performed and lastly taping was applied, fixing the foot on a rigid plastic plate with a non-elastic strapping; finally, parents were instructed on how to promote psychomotor development of their children. In addition, an above-knee posterior splint with the knee in 90° flexion and the foot in a corrective position was applied, which was worn full time (23 hours/day) until six months of age and then progressively reduced to night and naptime use (12 to 14 hours/day) at the age of 12 months; once walking was achieved, it was used only at night. After walking age, taping ended and physiotherapy continued two to three times per week up to 30 to 36 months of age. Open Achilles tenotomy was performed by a single experienced (about 20 years of practice in the field of clubfoot, 25 patients treated per year) orthopaedic surgeon in cases of limited dorsiflexion (lesser than 10°), plantar convexity appearance or radiographic evidence of equinus of the calcaneus on lateral radiographs at about four months of age.
At the second institute, treatment was performed according to the method described by Ponseti10 by a single experienced (about ten years of practice in the field of clubfoot, 25 patients treated per year) orthopaedic surgeon. The method included weekly sessions of manipulation and above-knee casting until complete abduction was achieved and then percutaneous Achilles tenotomy was performed if the foot could not be dorsiflexed to 15° at that time. After the last cast, the foot abduction brace was applied: the brace regimen included 23 hours a day for three months, then reduced to 18 hours a day and then removed gradually, one hour a day until a use of 12 hours a day. After walking age, the brace was worn at night and naptime until about four to five years of age.
Gross motor milestones analysis
Parents were asked to record on a sheet provided the age at which their child achieved three gross motor milestones: pull-to-standing, cruising and independent ambulation (ten steps without support). At each visit clinic, the validity of the parental report was supported by observation of the infant by the physician and/or physical therapist until independent walking.
Statistical analysis
Mean age at beginning of treatment, mean severity, rate of tenotomy and mean age of achievement of milestones were calculated.
The two-sample t-test was used to compare the mean results for the two groups. A p-value < 0.05 was considered statistically significant.
The 50th, 75th and 90th percentiles for the age of achievement were determined.
Analysis was performed using two-sample t-tests to evaluate if sex, severity at presentation, laterality or need of tenotomy could have influenced age of achievement of the three milestones.
Results
Overall, 52 infants were included in the study: 40 male patients, 12 female patients, 27 unilateral and 25 bilateral. Mean age at beginning of treatment was 24.3 days (sd 10). Mean DimS severity was 12 (sd 3.4).
Mean age at last follow-up was 48 months (sd 14). In no case a disorder that could have caused clubfoot deformity was suspected.
Results of mean age of achievement of milestones are reported in Table 1. By 18 months, all patients were walking without assistance.
Age, presented as months (sd) (where sd is reported), of achievement of motor milestones in clubfoot and normal infants (from present study and the literature)
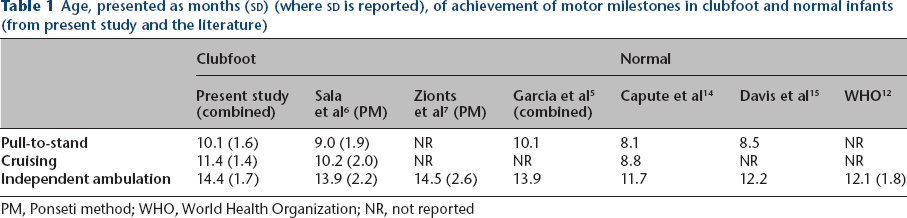
PM, Ponseti method; WHO, World Health Organization; NR, not reported
FM and PM group
At the first institute (FM) 26 consecutive infants (19 male, seven female, 18 unilateral, eight bilateral) were included. Mean age at beginning of treatment was 22.2 days (sd 8.7). Mean DimS severity was 10.8 (sd 3.1) (Table 2). Tenotomy was performed in 80.8% of cases at mean age of 127 days (sd 32). Correction was described as complete after tenotomy in all cases but in five patients at the time of independent walking some residual deformity was evident (two cavus, two varus, one limited dorsiflexion).
Comparison between the French physical therapy method (FM) and the Ponseti method (PM) group in the present study: characteristics of patients and treatment and age of achievement of motor milestones
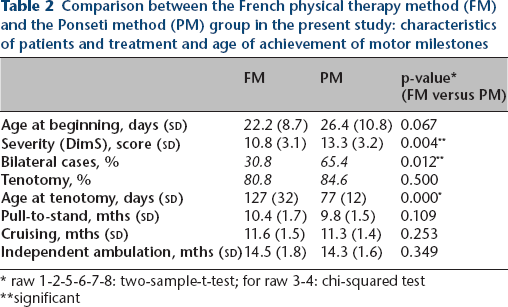
raw 1-2-5-6-7-8: two-sample-t-test; for raw 3-4: chi-squared test
significant
At the second institute (PM) 26 consecutive infants (21 male, five female, nine unilateral, 17 bilateral) were enrolled. Mean age at beginning of treatment was 26.4 days (sd 10.8). Mean DimS severity was 13.3 (sd 3.2) (Table 1). A mean of 4.8 casts (2 to 7; including post-tenotomy cast) was performed. Tenotomy was performed in 84.6% of cases at a mean age of 77 days (sd 12).
None of the infants in the PM group had any formal physiotherapy prior to walking age. Initial correction of the deformity was achieved in all patients.
FM versus PM group
Mean age at the beginning of treatment was slightly different (FM 22.2 days, PM 26.4 days) between the two groups but the difference did not reach statistical significance (p = 0.067). DimS was significantly higher in the PM group (13.3) than in the FM group (10.8; p = 0.004). The PM group included a significantly higher number of bilateral cases (65.4% versus 30.8% in the FM group; p = 0.012). The rate of tenotomy was similar (p = 0.500). Age at tenotomy was significantly lower in the PM group (77 days (sd 12)) than in the FM group (127 days (sd 32); p = 0.000).
The results of the mean age of achievement of milestones are reported in Table 2. Comparison of the age in the two groups showed a non-significant difference between the two groups for pull-to-standing (p = 0.109), cruising (p = 0.253) and independent ambulation (p = 0.349).
The 50th, 75th and 90th percentiles for the age of achievement of the three milestones are reported in Table 3, along with data reported in the literature for normal infants.11–15
Percentiles of age of achievement of motor milestones in clubfoot and normal infants (from present study and the literature)
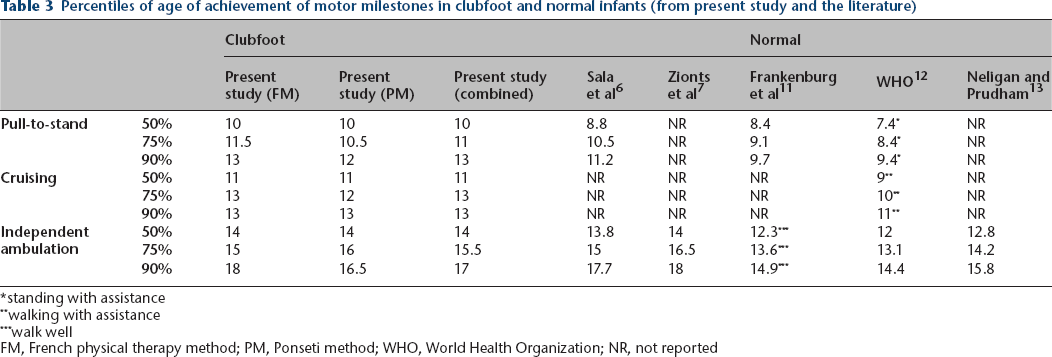
standing with assistance
walking with assistance
walk well
FM, French physical therapy method; PM, Ponseti method; WHO, World Health Organization; NR, not reported
Factors influencing milestones
An analysis was performed in the overall sample and in the two groups to understand if patient or treatment factors could have influenced achievement of milestones. Sex (male versus female), severity at presentation (DimS ≤ 14 points versus ≥ 15 points), laterality (unilateral versus bilateral cases) and need of tenotomy (performed versus not performed) were not found to significantly influence age of achievement of standing, cruising and independent ambulation in the FM group, PM group and overall sample.
Discussion
Gross motor development and achievement of independent ambulation may be delayed in infants with idiopathic clubfoot, as suggested by a few recent papers.5–7
Zionts et al 7 evaluated walking age in 94 patients and found that the mean age of independent walking was 14.5 months, about two months later than infants without clubfoot. Sala et al 6 analyzed gross motor milestones in a sample of 36 patients from rolling prone to supine to independent ambulation and found that delays were at most 1.5 months, except for walking age, which was approximately two months. Garcia et al 5 used the Alberta Infant Motor Scale to evaluate motor performance on a group of 26 clubfoot patients treated with different methods (PM 12 infants, FM nine infants or both five infants) and found a mild delay in attainment of motor skills at nine and 12 months of age in comparison with a group of normally developing infants.
These findings were confirmed in our study. Clubfoot patients in our study achieved pull-to-standing, cruising and independent ambulation approximately two months later than non-affected children: data for non-affected infants described in earlier studies11–15 are reported for comparison in the tables. Slight differences among clubfoot papers may be attributed to different inclusion criteria (for example, we have excluded patients that experienced relapse, included by Zionts et al7) or different brace protocol. Our regimen included 23 hours/day for three months, then reduced to 18 hours/day and then removed gradually, one hour a day until a use of 12 hours/day. The regimen used by Sala et al 6 and Zionts et al 7 included 23 hours/day for three months and then direct use at night and at naptime. In fact, different brace protocols have been described in the literature. 16
The motor delay found in our study was mild, with all patients walking by 18 months, which is similar to the results of other authors (90% of patients walking at 18 months for Zionts et al, 7 25 out of 26 patients in Garcia et al, 5 “almost all” in Sala et al 6 ). On the one hand this information can help to reassure parents and on the other hand can alert us that greater delays can be hardly attributed to clubfoot (in the absence of relapses or complications) and should be investigated with the suspicion of underlying conditions determining clubfoot and motor delay. Yet, a clear cut-off cannot be established.
It has been suggested that the motor delay in infants with clubfoot could be secondary to clubfoot pathology itself or to the treatment.5,6
As for pathology, an underlying mild motor development dysfunction related to clubfoot has been hypothesized. 5 This could be the effect of one or more of the multifactorial components hypothesized for clubfoot aetiology that would also negatively affect gross motor skills (for example, neuromyogenic imbalances). 5
Andriesse et al 17 analyzed motor ability at seven years of age in a group of 20 children treated for clubfoot by assessing the Movement Assessment Battery for Children, which includes items for the main motor skills (manual dexterity, ball skills and balance, coordination, visual-spatial perception, etc). They found an increased prevalence of motor impairment, with no relationship with foot status, laterality or the extent of surgery and suggested that other factors besides function may play a role.
As regards treatment, a possible cause for delay is the containment used to treat the deformity that is different according to the method used.
In the PM the use of long-leg casts initially and then foot abduction brace does not permit typical patterns of kicking in the early months of life. 5 Both feet are constrained and connected with a bar even if the deformity is unilateral. In the FM the constraints are different: taping and splinting are used without using a bar connecting lower extremities and massage, stretching and active facilitation are performed by parents and therapists.
This lesser constraint and greater stimulation is supposed to provide a better facilitation to motor development, but no study has evaluated this aspect and our findings did not confirm it; infants treated with the FM achieved the three gross motor milestones analyzed at a similar age in comparison with the PM group.
The characteristics of treatment performed in the two groups in the present study are similar to earlier descriptions for the two methods.9,10,18,19 In the PM group, a mean of 4.8 casts was performed (four to seven reported in the literature)6 and Achilles tenotomy was performed in 84.6% of cases (63% to 91% in earlier studies). 6 In the FM group the percentage of tenotomy (80.8%) was higher than that reported in previous studies (17% to 32%).19,20 Yet, more recent studies on the FM9,18,20 have suggested that early Achilles tenotomy in the FM may improve the final results and decrease the recourse to surgery.
The two groups were similar in terms of age at the beginning of treatment and the percentage of tenotomy performed. Age at tenotomy was significantly lower in the PM group and could have played a role. On the other hand, the PM group showed a more severe mean DimS and a higher percentage of bilateral cases. Infants with bilateral involvement have been supposed to represent a subgroup with more severe clinical expression in comparison with unilateral cases.21,22 Despite theoretical advantages of the FM group in terms of lesser severity and constraints, no superiority in motor milestones achievement was found.
To our knowledge, comparison between FM and PM in terms of motor development at walking age was previously performed only by Garcia et al, 5 that similarly reported no difference in gross motor development in the two groups, but the sample size was very small (nine patients for the PM and seven for the FM evaluated at 15 months of age).
As regards other factors possibly influencing motor milestones, Zionts et al 7 reported that motor development, particularly walking age, was influenced by severity of the deformity. This finding was not confirmed by our study. This difference is likely due to different criteria of inclusion of patients: the authors included in the analysis patients with relapses requiring treatments. In contrast, we have excluded these patients since it seemed obvious that a patient requiring longer period of immobilization and treatment would have revealed delay as shown by Zionts et al, 7 while our interest was in patients undergoing the basic treatment. By excluding these patients, no difference was found in relation to deformity severity, as reported by Garcia et al. 5
The strength of our study is that it represents a prospective analysis of consecutive cases treated in two centres experienced with the respective method (no bias of patient and treatment selection).
One of the main limitations is that data collection was partially performed by parents. We believe that data are to be considered accurate since parental reports were regularly verified by physicians and therapists at the visits, that are planned frequently (approximately every one to two months) at that age. In addition, the reliability of parental recall of developmental milestones of children has been analyzed by Majnemer and Rosenblatt: 23 the mean discrepancy was found to be less than 0.4 months at three to five years after occurrence of beginning of walking.
Analysis of results at final follow-up and of patients showing relapses after walking age lies outside the purpose of this study and was deliberately not performed. We acknowledge that the overall mean gross motor development for each method is clearly influenced by the rate of relapses, re-interventions and relative immobilizations. A comparison of results between the two treatments has been performed in very few papers.19,20,24 In a single-centre study (with parent-selected treatment), Richards et al 24 compared results of the FM and PM and found that initial correction rates were equal (95% and 94.4%, respectively), relapses occurred in 29% and 37% of cases, respectively, and outcomes were comparable at a mean follow-up of 4.3 years. Chotel et al 19 in a two-institution study reported higher rates of extensive surgery in the FM group (19% of feet) with lower clinical results at a mean follow-up of 5.5 years; in particular, they found that results for mild deformities were similar, but results for intermediate and severe clubfeet were better in the PM group.
In general, the FM has been reported to have less reproducible results, 19 that largely depend on the experience, skill and motivation of physical therapists. 25 This implies the necessity to develop a network of specialized physiotherapists and the need for geographic proximity of the patient to the competent physiotherapist. Other limiting factors of the FM in comparison with the PM may be the need for cooperation of families to assiduous physiotherapy and the cost/time requirement, not covered by all healthcare systems. 19
In this paper, only gross motor development until independent ambulation was analyzed and nothing can be said about further development in the two groups. In a recent paper, Zapata et al 26 analyzed gross motor function at ten years of age of children treated with either method and found that patients in the FM group scored higher on running speed/agility, body coordination and strength and agility. They concluded that it could be beneficial to incorporate physiotherapy during the maintenance phase of PM to maximize functional outcomes. Recently, a new hybrid protocol combining the advantages of the PM and FM has been proposed by Dimeglio and Canavese. 9
In conclusion, our results have confirmed that infants with clubfoot are expected to have a minimum delay in motor development and this finding could be used to reassure parents. Infants treated with the PM and those treated with the FM did not show significant differences in gross motor milestones achievement at walking age. Further studies are needed to evaluate gross motor development at longer follow-up.
Footnotes
Acknowledgements
The authors wish to thank Dr Salvatore De Masi (Clinical Trial Office, AOU Meyer, Florence) and Prof Giancarlo Bettuzzi for statistical analysis, Drs Alessandro Pagliazzi and Alessandra Novembri for their contribution in the treatment and follow-up of patients of FM group.
VF, CNA, CB, GS, EP, SDG: Data acquisition, Critical revision of the manuscript.