
Abstract
Abstract
Purpose
Asymmetric skin folds (ASFs) have been linked to developmental dysplasia of the hip (DDH) in select studies, leading to their inclusion in paediatric practice guidelines regarding orthopaedic referral for hip evaluation. The purpose of this study was to investigate the utility of isolated ASFs as a screening tool for DDH in a series of patient referrals evaluated at a single institution.
Methods
We performed a retrospective review of consecutive patients between 0 and 12 months of age referred to orthopaedic clinics for isolated ASFs. We recorded radiographic findings (acetabular inclination or alpha angle), diagnosis rendered and treatment administered.
Results
A total of 66 patients were included (mean age 6.4 months; 2.47 to 10.76). All patients received pelvic radiographs or ultrasound. In all, 36 patients (55%) were considered normal by their treating physician and 25 (38%) were considered dysplastic and underwent brace treatment. One hip with an isolated ASF was found to have a dislocated hip on radiograph prior to their initial orthopaedic visit. None of the patients in this study have required surgery to date.
Conclusion
Using ASFs as a reason for referral led to increased diagnosis of mild dysplasia resulting in orthotic treatment. Thus, in our particular clinical environment, isolated ASFs can be an indicator of mild dysplasia and warrant further workup or referral. Because treatment philosophies regarding recognition and treatment of mild dysplasia vary amongst centres, the value of screening with ASFs likewise depends on the treating orthopaedic surgeon's threshold for treatment of mild dysplasia.
Level of evidence
Level IV- Retrospective
Introduction
Asymmetric skin folds (ASFs) around the hips in children are often considered an early clinical sign for diagnosing developmental dysplasia of the hip (DDH). Early reports assert a relationship between subluxated or dislocated hips with additional thigh or gluteal folds. 1 Subsequent studies have expanded this association to reduced hips with acetabular dysplasia.1–5 Several studies claim that ASFs are an indicator of DDH due to their increased prevalence in patients with DDH compared with the normal population (27% to 83%2,3,5 rate in DDH patients versus 20%5–7). However, the significant variation in these rates calls into question the definition of asymmetry and the degree needed to be declared abnormal. Furthermore, these studies fail to include a control group that is not pre-screened that would allow a direct comparison of ASF rates using identical criteria. Adding to the confusion are similar studies with comparable flaws that contrarily do not demonstrate a large difference between the rates of ASFs in normal versus DDH populations. 6 Presently, the question as to the utility of ASFs as a diagnostic indicator of DDH remains unresolved.
Despite the absence of conclusive evidence for an association of ASFs with DDH, guidelines for general paediatricians, who perform most of the early DDH screenings in the United States, continue to instruct that ‘asymmetric thigh or buttock creases’ are a physical exam finding that may indicate DDH.8,9 In recent years, our orthopaedic surgery group has anecdotally noticed an increased referral rate of infants with all types of ASFs. Given the high prevalence of ASFs within the normal population, we questioned the utility of referring patients for DDH evaluation on the basis of ASFs alone.
The purpose of this study, therefore, was to investigate our institution's recent experience with infants referred for DDH assessment due to isolated ASFs. Rady Children's Hospital, San Diego is a tertiary referral centre at an academically affiliated stand-alone children's hospital with more than 1500 patients seen for DDH annually. We reviewed all patients referred for DDH evaluation because of an isolated finding of asymmetric gluteal, inguinal or thigh folds, and excluded those who were referred for any other reason. We catalogued the diagnosis and treatment of these patients to understand whether isolated ASFs led to the diagnosis of DDH within our practice environment. We hypothesized that infants referred for isolated ASFs would have typical hip development and would rarely have a subluxated or dislocated hip.
Materials and methods
The institutional review board approved this study. The electronic medical record was screened for patients with a primary referral reason of ‘Asymmetric Thigh Folds’ as entered by the orthopaedic practitioner at the time of the visit. Search dates were from May 2014 (when we began cataloguing referral reason) to February 2017.
The most comprehensive literature on ASFs has described asymmetric inguinal folds as being associated with an increased incidence of hip subluxation or dislocation in infants. 5 The association between middle or distal thigh ASFs with hip dysplasia is less clear. 10 Because the referring physicians and clinics do not seem to distinguish between the particular locations of ASFs, we have included all varieties in this study. We use the term asymmetric skin folds (or acronym ASFs) to describe any asymmetry of surface anatomy around the hip joint.
A retrospective chart review of all patients was conducted and the referral reason was verified. Patients were excluded if older than one year, or if there was a referral reason or diagnosis in addition to ASFs. We recorded demographic information, imaging type, diagnosis rendered (normal, dysplasia, subluxation/dislocation) and subsequent treatment. Anteroposterior and frog view pelvis radiographs were graded for the acetabular inclination (AI) by a single grader. The highest AI among either hip on either radiographic view was used for analysis. Subjects that were evaluated with an ultrasound at initial visit were graded using alpha angle. Alpha angle was measured on the coronal view for each hip and the lowest alpha angle among the two hips was used for analysis. Based on the work of Tönnis 11 and Graf 12 AI and alpha angle were used to grade the acetabulum as normal, mild DDH or DDH (Table 1). Descriptive statistics were performed for all outcome measures using Microsoft Excel (version 14; Redmond, Washington), except for distribution testing and analysis of variance testing between groups for AI which was evaluated using SPSS (version 24; IBM, Armonk, New York).
Radiographic classification
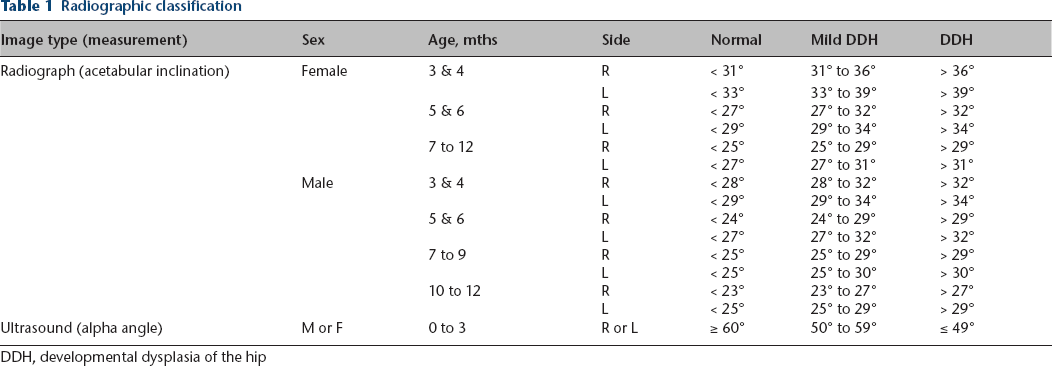
DDH, developmental dysplasia of the hip
Results
A total of 66 patients were included and were seen by any one of five treating surgeons, all fellowship-trained in paediatric orthopaedics with experience in treating DDH. Mean age at initial presentation was 6.4 months (sd 2.1; 2.47 to 10.76). Mean AI was 29.5° (sd 4.2°; 21° to 45°). Four subjects were initially evaluated with an ultrasound exam, their ages ranging from 2.47 months to 2.99 months and their alpha angles ranging from 55° to 65°. In all, 83% (55/66) of our cohort were female. A full list of our cohort characteristics can be found in Table 2.
Cohort characteristics
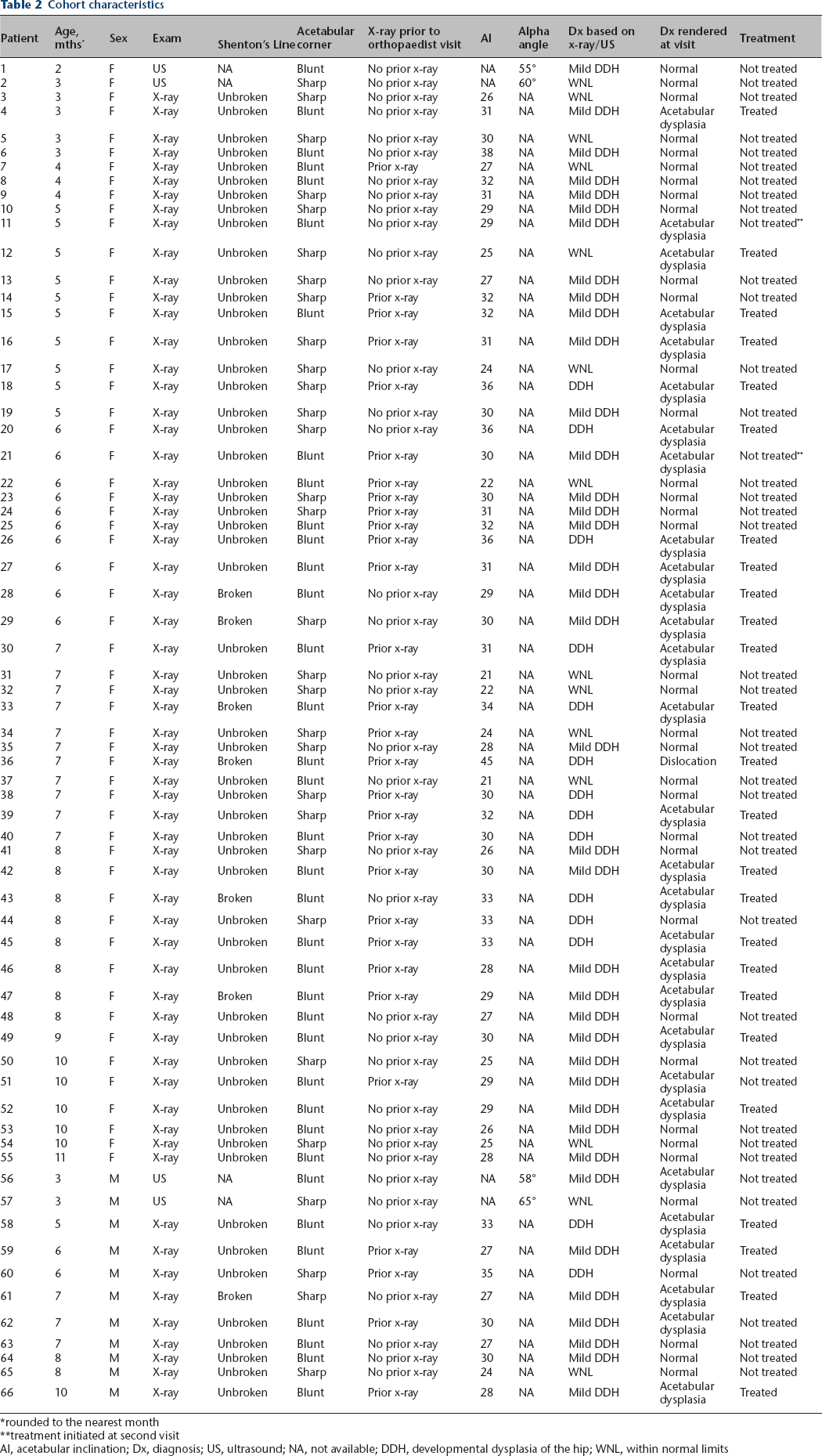
rounded to the nearest month
treatment initiated at second visit
AI, acetabular inclination; Dx, diagnosis; US, ultrasound; NA, not available; DDH, developmental dysplasia of the hip; WNL, within normal limits
A total of 30 patients (45%) were diagnosed with acetabular dysplasia by their physician at time of initial visit; one of these hips was dislocated. Although 45% of patients were deemed by their clinician to have acetabular dysplasia, only 38% (25/66) were treated at initial visit. Of note, two subjects declined treatment at initial visit, but were treated with a brace at their next visit. Based on AI or alpha angle, the majority (79%) of subjects referred for ASFs had acetabular dysplasia. In all, 58% (38/66) had mild acetabular dysplasia noted as an AI between one and two standard deviations above the mean for their age, sex and side; 21% (14/66) had acetabular dysplasia noted as two standard deviations above the mean AI for their age, sex and side; and 21% (14/66) of the cohort was found to have an AI within normal limits.
A total of 29 patients had radiographs prior to their orthopaedic visit, 26 had a radiologist's reading accompanying it. Of these, all patients (26/26) had a prior radiologist diagnosis of a hip abnormality on the spectrum of hip dysplasia. In all, 11 of these 29 were considered normal by our orthopaedic surgeons and were not treated, 17 were considered dysplastic and one had a left hip dislocation that was successfully reduced using a Pavlik harness.
Discussion
Our study sought to investigate the utility of using ASFs as criteria for DDH referral by paediatricians. We identified and analyzed a cohort of patients that were referred solely due to ASFs who conceivably would not have been evaluated by an orthopaedist without this finding or if the policy of advising referral on the basis of ASFs did not exist. One of these patients had a dislocated hip. Interestingly, although 79% of our cohort was found to have acetabular dysplasia based on strict radiographic classification, only 38% of our cohort had dysplasia significant enough to warrant treatment in the eyes on their treating physician (Fig. 1).

Anteroposterior pelvis radiograph of an eight-month old female patient in the study cohort who was diagnosed with acetabular dysplasia and treated with a Pavlik harness.
DDH in the newborn remains one of the few orthopaedic conditions in the United States for which routine screening is recommended.8,9 The concept is that a poor outcome (due to a late-recognized hip dislocation) can be prevented by early identification and intervention, as early treatments are less risky to the developing hip. Screening methods are not without controversy, however, as there is question as to their efficacy in reducing the rate of missed dislocations and there is evidence that screening significantly increases treatment rates.13,14 In addition, there is no cost-effective benchmark test for DDH, which turns DDH screening into an exercise in risk-stratification for the paediatrician.9,13 The ideal screening test would have a high sensitivity to limit the number of false negative tests (missed diagnoses), as well as high specificity to limit the number of false positive tests (unnecessary referrals to orthopaedic surgeons).
The utility of ASFs has been asserted and refuted throughout the DDH literature. Presumably, this is due to the varying definition of what constitutes an abnormal fold and the practitioner's sensitivity to this finding. Most estimates indicate that even normal infants have ASFs at about a 20% rate. 7 The most rigorous study of ASFs comes from Ando and Gotoh 5 from Japan, who studied abnormal inguinal creases in the frog-leg position of 2111 infants referred to orthopaedics and correlated their findings to the radiographic diagnosis. 5 They found an ASF rate of 23.8%, and found that ASFs were present in all 12 patients with dislocations or subluxations. Acetabular dysplasia without subluxation was diagnosed in 17 patients, yet only 41.7% of these patients exhibited ASFs. Their study demonstrated that ASFs are a sensitive test for dislocation or subluxation, but lack sensitivity in detecting acetabular dysplasia. Furthermore, with a 23.8% rate of ASFs in this large cohort, specificity was exceptionally poor as there were 470 patients with ASFs who did not have the disease. Using a prospectively collected sample of infants referred for DDH evaluation in the United Kingdom, Anderton et al 15 studied a 105-patient subgroup with ASFs to investigate the diagnostic value of the ASFs. Only two (2%) of these patients were found to have pathological DDH (subluxation or dislocation), and both cases had other physical exam findings present (limited abduction and Galeazzi sign) to diagnose a dislocation. The authors conclude that ASFs do not add value to the DDH examination, as these other exam findings are just as sensitive, with more specificity. 15
In the present study, we took a different approach than the aforementioned studies by investigating the fate of those patients who are referred solely because of ASF findings. This theoretically allows us to evaluate the additive benefit of ASF screening by eliminating contributions of other clinical factors. Like the Anderton et al 15 study, we did not associate hip subluxation or dislocation with ASFs in isolation. Distinct from prior reports, however, we found that 38% of patients referred with ASFs were treated for acetabular dysplasia with hip orthoses.
The reason for this discrepancy in treatment rates is likely due to variability in the threshold to diagnose and treat dysplasia. In our study, those that were treated for dysplasia had an average acetabular index of 29.5°, which is higher than expected at six months of age (girls ∼24°, boys ∼22°). 16 With growing recognition of the prevalence and morbidity of dysplasia in young adult hips, there are many paediatric orthopaedists who favour early treatment of mild dysplasia, both by orthoses and surgery, when necessary. 17 Undoubtedly, there are patients within our study cohort who would have normalized without treatment, yet with non-invasive and low-risk treatment options such as orthoses, it is not surprising that many surgeons opt to treat mild dysplasia to ensure its resolution. 18
This retrospective and small study does have noteworthy limitations based on its design and the nature of the subject. The approach of investigating patients who are referred to orthopaedists specifically because of ASFs, while offering a critical look at those patients, does limit the number of patients available for evaluation. Finding only 66 patients referred for isolated ASFs out of such a large potential pool demonstrates that our initial over-referral concerns were likely unfounded. In all, 44% of our cohort had a radiograph prior to their orthopaedic visit. We cannot determine if those radiographs were reviewed prior to the paediatrician referring the patient to orthopaedics, or if they were simply ordered to be performed prior to the orthopaedic visit because the paediatrician understood that radiographs would be needed. If some paediatricians routinely wait for a radiologist's reading prior to referral to orthopaedics, we have no way of knowing how many radiographs were ordered by paediatricians because of ASFs, but were not referred to orthopaedics because the radiologist's reading was negative. This may inflate the percentage of subjects with ASFs that require treatment. However, our orthopaedic surgeons were found to disagree with the radiology readings 42% of the time which may offset the risk of sample bias. Another limitation is the short follow-up interval. While the goal of this study was to document the initial treatment of screened patients with isolated ASF, there is no doubt that long-term follow-up of these patients could allow us to see the effects of our treatment decisions. In fact, a major limitation to all studies on this topic is the poor understanding of the natural history of mild dysplasia. 19 Until the orthopaedic community gains the ability to differentiate between those patients with mild dysplasia who warrant treatment and the great majority that will improve on their own,20,21 this uncertainty will remain pervasive in this and other studies.
Clearly the North American medical-legal climate makes definitive diagnosis and treatment of infantile DDH problematic for multiple medical specialists including paediatricians, radiologists and orthopaedic surgeons. Paediatricians, averse to missing a DDH diagnosis and diligently following their academy guidelines, search carefully for findings such as ASFs and then refer for imaging studies. The radiologist, fearing legal consequences, is more likely to err on the side of over-diagnosis when encountering a borderline case. Finally, the orthopaedic surgeon, faced with anxious caretakers and a diagnosis of dysplasia already in the printed record, may be more inclined to treat the mild dysplasia.
How our experience should be applied is likely related to the economic and cultural climate in which one practices. In circumstances that necessitate an economical approach to diagnosis and treatment, where the concern is only detection of subluxation/dislocation, ASFs alone seem to offer no additional value. If the practice environment warrants that the physicians recognize (and potentially treat) all dysplasia, including mild cases, then isolated ASFs can identify patients who would otherwise escape detection. If this philosophy is to be utilized, the literature would suggest that focusing on more proximal or inguinal asymmetry offers greater diagnostic value. 5
After careful analysis of our results and consideration of limitations, we conclude that there can be utility in the use of ASFs as a screening criteria for acetabular dysplasia, depending on the orthopaedist's threshold for treatment. Referring paediatricians should continue to use this as only a single criterion among many, recognizing that ASFs in infancy are a very common finding with limited specificity. Orthopaedic surgeons might consider their threshold for dysplasia treatment when advising their referral base on the utility of ASFs in their particular practice.
Future studies on this subject would require prospective evaluation of all infants to characterize their specific skin fold anomaly so that we may better understand if particular patterns enhance diagnostic ability. Also, further prospective evidence regarding late outcomes of mild dysplasia with and without treatment would greatly improve our understanding of DDH screening practices.
Footnotes
Acknowledgements
CRL: Study design, Data collection, Data interpretation, Manuscript preparation.
JDB: Study design, Data analysis, Data interpretation, Manuscript preparation.
MEP: Study design, Manuscript preparation.
SJM: Study design, Manuscript preparation, Data interpretation.
VVU: Study design, Manuscript preparation, Data interpretation.
DRW: Study design, Manuscript preparation, Data interpretation.
VVU reports work as a paid presenter or speaker for BroadWater, DePuy, A Johnson & Johnson Company, Nuvasive and OrthoPediatrics; research support for EOS Imaging; paid consultancy for Globus Medical and OrthoPediatrics; stock or stock options in Imagen; research support for Pacira; publishing royalties, financial or material support from Wolters Kluwer Health – Lippincott Williams & Wilkins, outside the submitted work.
DRW reports paid consultancy for Rhino Pediatric Orthopedic Designs, Inc., outside the submitted work; publishing royalties, financial or material support from Wolters Kluwer Health – Lippincott Williams & Wilkins, outside the submitted work.
All other authors declare no conflict of interest.