
Abstract
Abstract
Purpose
This study aimed to elucidate whether levels of physical activity (PA) return to normal after bone healing or whether long-term behavioural changes in PA are to be expected in children and teenagers who have sustained limb fractures.
Methods
In all, 100 children and teenagers with a first episode of limb fracture and 100 sex- and age-matched healthy controls (CTRL) were recruited for a prospective study. PA in limb fracture patients was assessed at 18-month follow-up using accelerometer measurements, and values were compared with those of CTRL. Time spent in PA at different levels of intensity was determined for each participant and expressed in minutes and as a percentage of total validly measured time.
Results
Mean levels of PA at different levels of intensity by previously injured children and teenagers were similar than CTRL (42 sets of paired data). However, time spent in moderate-to-vigorous PA (MVPA) was lower than 60 minutes among limb-fracture patients at 18-month follow-up.
Conclusion
The amount of skeletal loading in children and teenagers returns to normal values by 18 months after limb fracture. Even if time spent in MVPA is not significantly lower in children and teenagers with limb fractures, it no longer reached the international recommendations for school-aged children (MVPA > 60 minutes), which may be interpreted as a lifestyle modification or a behavioural change to avoid new trauma.
Level of Evidence
II
Introduction
Physical activity (PA) has significant health benefits; it contributes to the prevention of cardiovascular diseases and is an essential factor for the regulation of bone homeostasis. Indeed, the skeleton needs continuous physical stimulation to maintain healthy bones otherwise bone loss ensues. 1 Bone mineral mass is higher in children who are physically active compared with those who are mildly active 2 and higher in children who participate in activities that generate high-impact forces than in those who engage in activities that impart lower-impact forces.3–10 Prospective studies have also demonstrated that PA intervention programmes in children improve bone mass and muscle strength.11–14 Based on this evidence, it is now recommended that PA for children include activities generating relatively high ground-reaction forces, such as jumping, skipping, running and possibly strengthening exercises. 15
It is also recognized that a lack of normal stress on bone can result in osteopenia,16–18 the bone's physiological response to disuse. In children and teenagers, loss of bone mineral mass usually occurs during phases of reduced PA, such as when an injured extremity spends several weeks in a cast. 19 In a previous study, we demonstrated that there was a significant reduction in levels of PA among subjects with lower-limb fractures during cast immobilization and, primarily, that the time spent in vigorous PA was 84.4% lower in children and teenagers with lower-limb fractures than their healthy peers. 20 In contrast to adults,21–23 full recovery from post-traumatic osteopenia is expected in children and in teenagers.24–26 Clinical experience on this point shows that children and teenagers exhibit faster functional rehabilitation in normal daily life than adults do. The major mechanisms explaining this phenomenon probably include greater flexibility, muscle strength, muscular balance, agility, functional coordination and, above all, they feel the need to be active again. All these parameters help them to achieve a full return to their pre-injury level of PA by accelerating the mechanical loading of their skeletons.27,28
Nevertheless, there are currently no data to prove that levels of PA really do return to normal among children and teenagers who have sustained limb fractures. Thus, this study's purpose was to elucidate whether levels of PA return to normal after bone healing, or whether long-term behavioural changes in PA are to be expected in children and teenagers who have sustained limb fractures.
Methods
Experimental approach to the problem
This study aimed to elucidate whether levels of PA return to normal after bone healing or whether long-term behavioural changes in PA are to be expected in children and teenagers who have sustained limb fractures. PA was measured 18 months after the fracture, when children and adolescents were considered healed and had recovered normal PA. Objective measurements of PA were obtained using a uniaxial accelerometer (Actigraph 7164, MTI, Fort Walton Beach, Florida). The present study focused above all on total activity counts, thus on average range of PA. We used also the intensity level cut-offs described by Ekelund et al 29 where sedentary behaviour was defined as less than 500 counts.min-1, light PA was from 500 to 1999 counts.min-1, moderate PA was from 2000 to 2999 counts.min-1 and vigorous PA was > 3000 counts.min-1.
Subjects
We conducted a longitudinal, matched case-control study including 100 children and teenagers with a first episode of limb fracture (50 lower-limb fractures; 50 upper-limb fractures) and 100 healthy, paired controls (no history of fracture) aged 10 to 16 years old and recruited to the study through an advertisement. Injured children and teenagers were selected if they had been admitted to hospital as inpatients for orthopaedic reduction or minimally invasive surgery (closed reduction and stabilization using percutaneous wires or screws) of their fracture under general anaesthesia, if they had worn a cast during their healing phase and if they agreed to undergo follow-up at the orthopaedic clinic during the whole duration of the study (from time of fracture until 18-month follow-up). Exclusion criteria for both injured adolescents and healthy controls were: prior history of bone fractures; chronic disease; congenital or acquired bone disease; any condition limiting PA; and hospitalization for more than two weeks in the previous 12 months. All participants and their parents provided written informed consent, and the protocol was approved by the institutional ethics committee.
Anthropometric measurements
Standing height was measured in bare or stockinged feet using a precision mechanical stadiometer, and body weight was measured using a mechanical calibrated beam scale. Body mass index (BMI) was calculated as weight in kilograms (kg) divided by height in metres squared (m2).
Measurement of PA
PA was measured 18 months after the fracture. Objective measurements of PA were obtained using a uniaxial accelerometer (Actigraph 7164). Monitoring was set on a one-minute cycle, and at the end of each run the sum was stored in the memory and the numerical integrator was reset. Accelerometers were attached above the iliac crest of the right hip using an elastic belt and adjustable buckle, and they were oriented vertically in the same direction. Accelerometers were programmed to start recording at 08:00 on the first day of measurement and participants were asked to wear them continuously for ten days. As we had no criteria defining absolute normal PA in children and teenagers, data emanating from sex- and age-matched healthy controls were regarded as comparative values.
PA data interpretation
Data reduction was carried out based on criteria applied in previous publications.29–32 Only periods between 08:00 and 21:00 were analyzed. Periods of zero activity of 20 minutes or longer were interpreted as being due to unworn accelerometers and were removed from the activity totals. 33 Participants who did not manage to record more than 600 min.d−1 of activity30–32,34,35 for at least five consecutive days were excluded from further analysis. 36 Data were expressed as total activity counts per registered time (counts.min−1) to generate an average range of PA. We used the intensity level cut-offs described by Ekelund et al 29 where sedentary behaviour was defined as less than 500 counts.min−1, light PA was from 500 to 1999 counts.min−1, moderate PA was from 2000 to 2999 counts.min−1 and vigorous PA was > 3000 counts.min−1. Time spent in each category of PA intensity was also determined for all participants as a percentage of total validly measured time.
Statistical analysis
Pairs were matched for age (± six months) and sex (male/female). Data are expressed as mean ± sd. A paired Student's t-test with an alpha threshold of 5% was used to analyze the variability of matching characteristics (age and sex) between cases and healthy controls. A Shapiro–Wilk test with an alpha threshold of 5% was used to test the normality of PA variables. As these variables were not normally distributed, a paired Wilcoxon test with an alpha threshold of 5% was used to assess differences in PA levels between previously injured participants and healthy controls. We decided not to use imputation of missing values if more than 10% of the data were missing since we considered that excluding rows prevented any errors from being introduced due to the missing values. Data analyses were performed using STATA 9.2 software (StataCorp LP, Lakeway Drive, Texas). Based on total activity values and using G*Power 3.1.9.2., 37 the statistical power for the upper-limb fractures (44 participants, 22/matched group, effect size = 0.64) was 99% and for the lower-limb fractures (40 participants, 20/matched group, effect size = 0.58) was 97%. Good reliability of the dependent measures was reported (intra-class correlations > 0.85). 38
Results
A total of 66 injured children and teenagers were reviewed at 18-month follow-up. However, pairing was only possible with 42 healthy controls due to data reduction, pair-matching procedures and above all a high number of patients who refused to wear the accelerometer. Age, physical characteristics and the PA levels of paired cases with fractures and their healthy controls are shown in Tables 1 and 2. Patients with lower-limb fractures received a bent-knee long-cast and were instructed to follow a strict zero weight-bearing directive during the initial healing phase. After three to six weeks, the initial immobilization device was removed and a below-the-knee walking cast was worn until definitive bone healing. All patients with upper extremity fractures were immobilized into a long-arm cast during the initial healing phase, followed by a forearm cast until bone healing.
Characteristics and physical activity measures of adolescents with upper-limb fractures versus healthy controls at 18-month follow-up
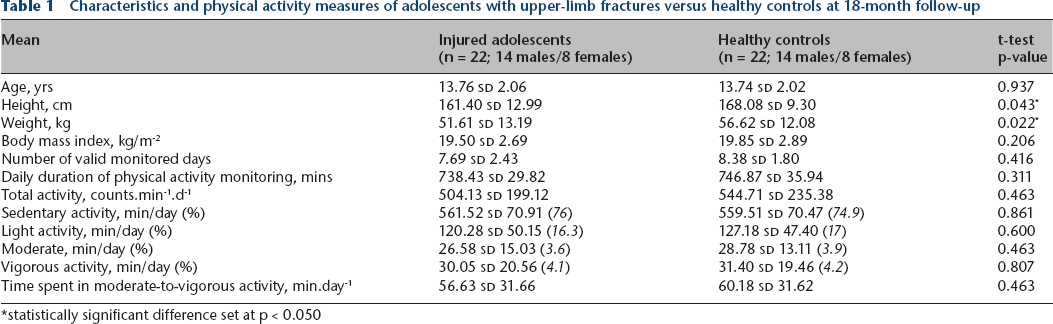
statistically significant difference set at p < 0.050
Characteristics and physical activity measures of adolescents with lower-limb fractures versus healthy controls at 18-month follow-up
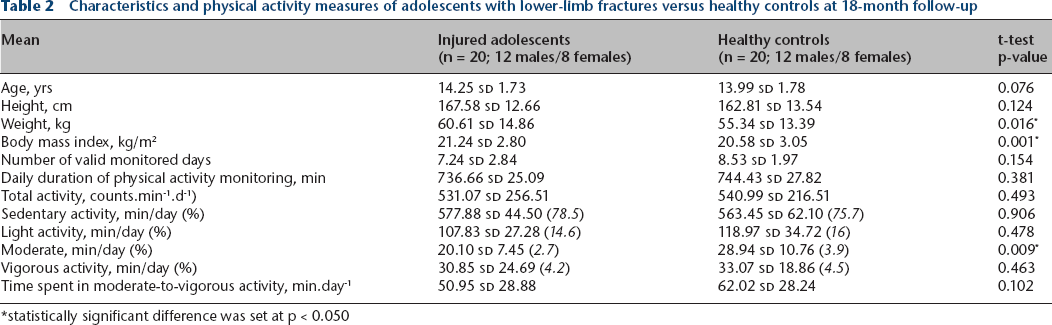
statistically significant difference was set at p < 0.050
When considering all the children and teenagers with fractures together (upper and lower limbs), there were no statistical differences from their controls with regards to age, height, weight, daily duration of PA monitoring or the mean number of valid monitored days. Children and teenagers with limb fractures demonstrated the same level of PA as healthy controls. No significant differences between injured children and teenagers and healthy controls were noted with regards to time spent in moderate PA or in vigorous PA (VPA). However, time spent in moderate to vigorous PA (MVPA) was below 60 minutes (53.9 minutes) among previously injured participants, thus no longer reaching the international recommendations for school-aged children. 39
Pairing children and teenagers with upper-limb fractures with healthy controls was possible in 22 cases. The upper extremity fractures’ group included 19 wrist's fractures and three forearm's fractures. Their comparative ages, physical characteristics, and levels of PA are shown in Table 1. There were no statistical differences between the groups with regards to age, daily duration of PA monitoring or the mean number of valid monitored days. However, those who had sustained an upper-limb fracture were significantly taller (p = 0.0428) and heavier (p = 0.0216). Children and teenagers with upper-limb fractures demonstrated the same PA levels as healthy controls. No significant differences were noted between injured adolescents and healthy controls for time spent in MPA or VPA. However, time spent in MVPA was less than 60 minutes (56.6 minutes), thus no longer reaching the international recommendations for school-aged children. 39
Pairing children and teenagers with lower-limb fractures with healthy controls was possible in 20 cases. The lower-limb fractures’ group included 18 ankle fractures and two leg fractures. Their comparative ages, physical characteristics and levels of PA are shown in Table 2. There were no statistical differences between the groups with regards to age, daily duration of PA monitoring or the mean number of valid monitored days. However, those who had sustained a lower-limb fracture had a significantly higher weight (p = 0.0156) and BMI (p = 0.0012). Children and teenagers with lower-limb fractures demonstrated the same level of PA as healthy controls, but they also exhibited a significant residual reduction in time spent in moderate PA (-30.5%; p = 0.0086) in comparison with the values of healthy teenagers. No significant difference was noted between injured children and teenagers and healthy controls for time spent in VPA. Again, the time spent in MVPA was less than 60 minutes (51 minutes) among previously injured participants, thus no longer reaching the international recommendations for school-aged children. 39
Discussion
Limb fractures and subsequent cast immobilization constitute a frequent cause of a reduction in childhood levels of PA, the predictable consequences of which are a loss of bone mineral tissue and substantial muscle atrophy. A full restoration of bone mineral mass in childhood may only occur upon reaching pubertal maturity40,41 and, above all, a return to normal activity. 42 Nevertheless, there is currently no data to prove that levels of PA really do return to normal among children and teenagers after a fracture since there is no certainty that behavioural changes in PA do not occur.
To the best of our knowledge, this study is the first to report measurements of PA in a representative sample of a paediatric population after the healing of upper- and lower-limb fractures. The present study revealed that children and teenagers with limb fractures returned to the same levels of PA as healthy controls. No significant differences were noted between injured adolescents and healthy controls with regard to the time spent in VPA. However, it was noted that children and teenagers with fractures were less active and exhibited a significantly lower amount of time spent in MVPA at 18-month follow-up (53.9 minutes). This phenomenon was more pronounced for lower-limb fractures (51 minutes) than for those affecting upper limbs (56.6 minutes). The rate of MVPA was 10% lower at 18-month follow-up (15% lower for patients after lower-limb fractures) and may suggest a permanent reduction in the time spent in MVPA among patients after a fracture, which may be interpreted as a lifestyle modification or a behavioural change to avoid new trauma. As mentioned above, international recommendations are that school-aged youths should participate in at least 60 minutes of MVPA daily to prevent weight gain and increase bone mineral mass. 43 Being sedentary is a strong contributor to being overweight and of low physical fitness. The reduction in PA among adolescents after fractures results in them expending less energy, and our clinical experience has shown that when this reduction occurs during the cast immobilization period, it could be a starting point from which children and adolescents become overweight.
The present study has some limitations in its interpretation. Firstly, there are activities during which accelerometers have to be removed (swimming) or do not accurately measure the intensity of exercise (cycling). These unmonitored activities may result in underestimations of PA. Nevertheless, Trost et al 44 stated that adding children's self-reported periods of unmonitored activity to registered accelerometer data led to no significant changes in calculated activity levels. Secondly, to obtain ten days of recordings, activity counts were averaged using a one-minute epoch in order to ensure that the accelerometer's memory capacity was not exceeded. This averaging method underestimates the teenager's VPA because such activity is rarely sustained for longer than one minute. 35 Previous studies have demonstrated that VPA may be substantially underestimated. 26 However, the underestimation of VPA is unlikely to be significant in the present study as we can hypothesize that it would be the same for both groups. Thirdly, 24 (36.4%) recordings had to be omitted from the analysis because of data from obviously defective accelerometers, a failure to reach the minimum number of days required or the minimum number of minutes per day to validate recordings or even refusal to wear the accelerometer. The 36.4% exclusion rate is significantly higher than the data published by Pate et al, 45 who reported a 6.3% exclusion rate over a seven-day recording period, but it was closer to the 25% exclusion rate over a three-day period reported by Riddoch et al. 35 The greatest limitation to the interpretation of the present findings is due to the combination of the high percentage of missing data (36.4%) and the high drop-out rate among participants at 18 months (34%). Finally, the number of patients is unfortunately too low to identify clinical differences for absolute values of PA; large prospective studies are, therefore, needed for improving recruitment and for identifying significant differences between the two groups.
Accelerometer use has become increasingly popular in PA research but it is a challenging method when dealing with teenagers, and it is prone to problems of missing data, which complicate the data reduction and analysis process. Many studies have focused on the optimal approach for obtaining high adherence and low levels of missing data. Applying adherence-promoting strategies, such as approaching the research participant as a partner, building a personal rapport with teachers, parents and coaches, using different means of reminding participants about the study's progression (reminder stickers, cell-phone applications) and, above all, providing adequate incentive payments, may have a positive impact on the wearing of accelerometers and thus on data quality. 45
Conclusion
Even though accelerometer use in PA assessment remains prone to problems involving missing data (which may complicate data reduction and result analysis), it remains a valid tool with which to quantify reductions in levels of PA among children and teenagers after limb fracture and for assessing the recovery of PA levels. The present study suggested that children and teenagers with limb fractures exhibited a permanent reduction in the time they spent in MVPA, which may be interpreted as a lifestyle modification or a behavioural change to avoid new traumas. As MVPA is known to have beneficial effects on bone composition, cholesterol, blood pressure, blood sugar, aerobic fitness, muscular strength, movement skills and bone health, this study provides important information about how PA by children and adolescents could be restored to appropriate levels after limb fracture. Physicians must keep in mind that behavioural change and lifestyle modification may occur after a limb fracture, and make sure that the affected children/teenagers have resumed their habitual pre-fracture activities. We have thus to elaborate more effective ways of reaching the ideal MVPA guideline during physical education, as well as increasing MVPA during school time and extracurricular activities. Such strategies require increased intensity when doing activities related to locomotion, such as jumping, leaping, hopping and running during physical education and extracurricular activities. Achieving competence in motor skills should be a priority to increase MVPA in both sexes and teachers should be encouraged to identify stimulating options to do so.
Footnotes
Acknowledgements
This work was supported by grants from the Swiss National Science Foundation (SNSF #405340-104611); the funding source played no role in study design, the collection, analysis and interpretation of data, writing or the submission of this report.
XM reports grants from Swiss National Science Foundation during the conduct of the study.
CS reports grants from Swiss National Science Foundation during the conduct of the study.
AT-F reports grants from Swiss National Science Foundation during the conduct of the study.
RD reports grants from Swiss National Science Foundation during the conduct of the study; and grants and personal fees from DePuy Synthes and Medtronic outside the submitted work.
CD reports grants from Swiss National Science Foundation during the conduct of the study.
DC reports grants from Swiss National Science Foundation during the conduct of the study.
XM: Participated in study's coordination, Performed the CSA investigation, Collected the data, Realized data's interpretation, Revised the article for important intellectual content.
CS: Participated in drafting and critically revising the article for important intellectual content.
AT-F: Participated in drafting and critically revising the article for important intellectual content.
RD: Participated in drafting and critically revising the article for important intellectual content.
CD: Performed the data analysis and the statistical analysis, Revised the article for important intellectual content.
DC: Participated in the design, conception and coordination of the study, Collected and treated the patients, Revised the article for important intellectual content.
All authors read and approved the final version of the manuscript to be submitted.