
Abstract
Abstract
Purpose
To point out the need to take into account the dysplastic nature of tarsal bones when treating idiopathic clubfoot (CF).
Methods
Review the published evidence on the developmental abnormalities of tarsal bones in idiopathic CF.
Results
The literature review provides abundant proof of the existence of delayed appearance and slower development of ossification centres of tarsal bones in idiopathic clubfoot.
Conclusion
Gentle manipulations and casting are the cornerstone of the Ponseti method. The biological response of all foot elements is critical for a successful outcome. Delayed ossification and abnormal development of tarsal bones in idiopathic CF may affect the results. Development of a personalized tailored bracing protocol based on severity assessment and response to casting treatment will improve results and quality of care in CF management.
Level of Evidence
V
Introduction
Understanding the ossification process and the development of tarsal bones in idiopathic clubfeet (CF) is of utmost importance in achieving and maintaining successful results of treatment using the Ponseti method.
In infants, ossification centres (OC) of the tarsal bones are relatively small within a large cartilaginous mass. During growth and development, the OC expand from the centre to the periphery of each bone, assuming the shape into which the cartilaginous anlage has already been moulded by the sequential gentle manipulations and casting according to the Ponseti method. The treatment protocol is based on a sound understanding of the functional anatomy and the biological response of all foot elements until the correct position change is gradually obtained. It is possible to predict the shape of the tarsal bone from the shape of the ossific nucleus.
Pirani et al 1 followed CF treated with the Ponseti method using MRI. In their study they were able to demonstrate what happens between cast changes. They reported on the correction of a wedge-shape talar head, medial talar inclination as well as medial navicular displacement. Furthermore, they showed the correction of the wedge-shaped distal calcaneal articular surface and medially displaced cuboid. The inverted calcaneus reverts to a normal position. Once the tarsal bones retain their normal 3D relationships with corresponding moulded cartilaginous anlage and enough ossification volume, the foot can better resist the tendency of treated CF to relapse.
We have shown 2 that there is a direct relationship and significant correlation between the neonatal foot length, severity of the CF and the treatment outcome. A small foot size may represent a less mature newborn with a lesser developed foot.
It was shown that the use of a foot abduction brace (FAB) is one of the most important factors in maintaining the initial correction3,4 and non-compliance with bracing protocol may result in recurrence of the deformity. Randomized clinical trials trying to identify the optimal duration of FAB use, following successful correction of CF are not available. Ponseti's initial recommendation was two years of night use 5 but others have suggested that longer bracing is more effective.4,6 To date, the Ponseti information website (http://www.ponseti.info/ponseti-method.html) advocates that a FAB should be worn 23 hours a day for two to three months and thereafter at night for an additional three to four years. There is a lot of confusion in the paediatric orthopaedic community and the duration of brace use is varied. 7
Here we provide published evidence on the dysplastic nature of CF tarsal bones (Fig. 1), challenging the dogma of using the FAB for an initial two- to three-month period during the critical period of early development of the tarsal bones following successful correction of idiopathic CF. We would like to suggest extending the first FAB usage period and gradually weaning children off the bracing at nine to 12 months of age in order to maintain correction and prevent or reduce relapses in the more rigid and severe idiopathic CF.

Anteroposterior radiograph of both feet taken together of a three-year-old boy with a unilateral (R) clubfoot treated according to the Ponseti method. Note the size differences of the cuboid and the cuneiforms between the affected (R) and the non-affected (L) foot. The ossification centre of the affected tarsal navicular and intermediate cuneiform are not ossified yet.
We strongly believe that the early phase of the bracing protocol should be tailored according to the severity assessment, i.e. age at presentation, initial Pirani score, number of casts needed for correction, need for tenotomy, etc. The idiopathic CF population is quite heterogeneous. Some children need more casts and a longer bracing period while others will benefit from shorter casting and bracing period.
Evidence on the dysplastic nature of tarsal bones
In 1945 Leonard 8 emphasized the importance of using physical force to correct the deformity and mechanical fixation to maintain the correction until certain changes in the structural elements of the foot have taken place. Failure of treatment is thought to be the result of insufficient rather than wrong management.
Based on ossification index of foot, Leonard 8 made a comparative study of congenital CF. His conclusion was that the usual normal variation in appearance of OC exists in the feet of children under treatment for congenital CF. There is a certain percentage of abnormal delay in the appearance of ossification in cases which experienced a relapse of the deformity and had a corrective operation. The ossification process of the lateral cuneiform in children with CF treated using the Ponseti method was studied by Lang et al. 9 They have demonstrated that although the lateral cuneiform is growing in all dimensions during the follow-up period, it remained smaller than the unaffected side.
The advantages of a series of gross and histological sections after autopsy of CF patients are obvious. This technique allows observation of the bony and soft-tissue pathology as well as demonstrating the intrauterine deformities without the influence of advanced growth or treatment. In 1972 Irani and Sherman 10 preformed autopsies of 11 extremities with CF and found that the talus and calcaneus are always abnormal due to a deformed cartilaginous analgan with a probable developmental intrinsic germ plasm defect before six weeks of gestation.
Shapiro and Glimcher 11 published a histological study which showed that the OC of the talus was smaller and positioned anteriorly and laterally compared with a normal OC which was positioned close to the geometric centre. In this study, further abnormalities of the enchondral sequence of the OC were demonstrated and the authors’ conclusion was that the pathology origin of talus is due to a primary developmental defect in the cartilage analage.
Gilbert et al 12 investigated congenital CF calcaneal growth plates and demonstrated that they were virtually inactive, probably due to primary growth disorder, causing slower ossification compared with the normal ones and leading to hypoplasia and subsequently a smaller foot.
The shape of talus described by Ippolito 13 , Irani and Sherman 10 , Shapiro and Glimcher 11 and Ippolito and Ponseti 14 was small and altered, with a short neck and a medially angulated dome shaped head, positioned in plantarflexion. The OC was relatively smaller, eccentric and more lateral and anterior compared with the normal one and the anterior part of the trochlea did not articulate with the ankle mortise.
Imaging studies using the 3D MRI technique demonstrated that the volume of both the bone and the cartilaginous structures were smaller in the CF together with a reduction in volume for the cartilaginous anlage and osseous nucleus.15–17 The length of the CF talus was shorter than normal, 16 the neck and the head were medially angulated18,19 and the long axis of the osseous nucleus was medially rotated relative to the long axis of the cartilaginous anlage. 15 The tibiotalar joint demonstrated a severe plantarflexion such that only the posterior part of the body of the talus articulated with the mortise and a wedge-shaped head of the talus. 1 Roche et al 20 followed seven adolescent patients that were treated surgically for CF and showed that all tarsal bones were smaller in volume and area compared with the contralateral normal foot as well as the talar articular surface and the tibiotalar articular surface. Kamegaya et al 21 found a correlation between the degree of talonavicular malalignment and the severity of CF as well as more a medially deviated navicular when compared with normal feet.
It is accepted that the CF deformity of the calcaneus is less distorted than the talus. 10 The coordination of perichondral and endochondral ossification is disturbed and ossification grooves and associated cartilage canals are not found in regular positions. 22 The calcaneus usually appears slightly shortened and widened, with a mild medial bowing.14,23 Ippolito 13 and Ippolito and Ponseti 14 found that the calcaneus was tilted and medially rotated underneath the talus, being part of the varus deformity. Howard and Benson 24 showed that the calcaneus ossific nucleus lay more obliquely and the proportionate size and position were similar to the normal foot. In MRI studies the calcaneus was significantly more externally rotated relative to the talar body, 25 resulting in anterior medial, posterior lateral and plantar deviation. The cartilaginous anlage was aligned in relative parallelism, as described earlier for the talus. 15 The size of the calcaneus in the MRI study was smaller for the CF patients compared with the normal foot but with a lesser reduction when compared with the talus reduction of size; 20% versus 40%, respectively. 15 Furthermore, the calcaneal ossific nucleus was reduced by 12.1% in comparison with the talus which was reduced by 42.6%; the calcaneus was 4.8% shorter while the talus length was 8.2% shorter than normal. The same trend was shown for the cartilaginous anlagen as well as the distal location of the ossific nuclei. 17 These findings indicate a disproportionate growth between the talus and calcaneus in CF.
The normal appearance of the navicular OC is around four years of age and it is the last tarsal bone to ossify (Figs 2 and 3). 8 In dissection studies of CF the navicular size was small, normal in shape and proportional to the severity of the deformity of the talus.10,13,14 Pirani et al 1 described a long wedge-shaped navicular with flattened lateral and dorsal surfaces compared with its plantar surface. These findings were supported by Napiontek 26 who described a decrease of the navicular OC, its flattening, fragmentation, cystic-like changes and wedging.

Anteroposterior radiographs of both feet taken together of a three-year-old boy with a unilateral (L) clubfoot treated according to the Ponseti method. The navicular and intermediate cuneiform ossification centres are not seen yet.
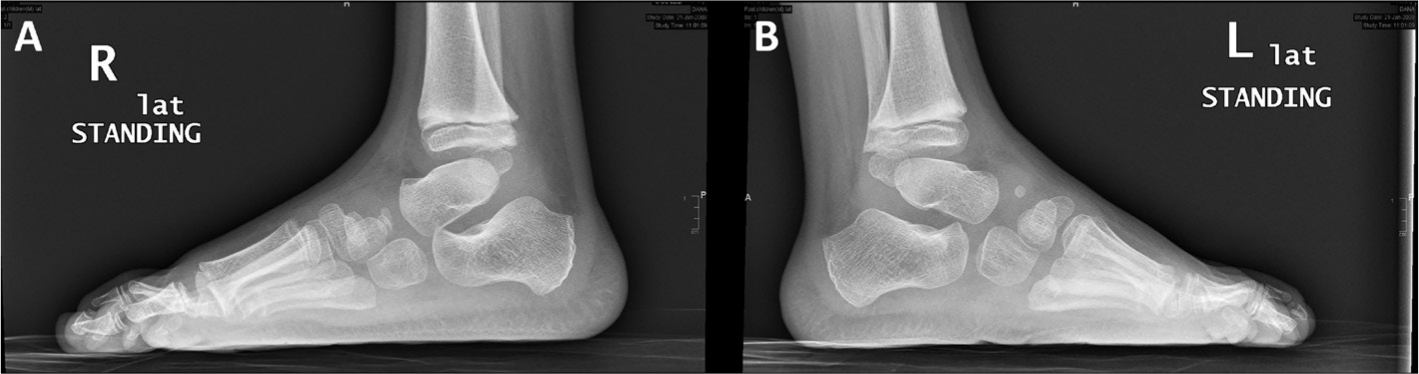
Lateral standing radiographs of a six-year-old boy treated for left clubfoot according to the Ponseti method. Note that the ossification centre of tarsal navicular bone is just appearing in the affected foot (L).
The navicular articulated with the talus medially8,10,13,14,27 with adduction and inversion, and may have been displaced sufficiently to be in close contact with medial malleolus and if severe enough, with the medial tuberosity of the head of the talus. 1 MRI studies support previous findings of medial dislocation of the navicular relative to the talar head.18,21,25,28 Kamegaya et al 18 were able to demonstrate the entire anlage of the navicular which was perpendicular to the transmalleolar axis of the longitudinal line of the talar body. Pekindil et al 19 revealed dorsal talonavicular subluxations which were not apparent on radiography in MRI sagittal slices.
In Roche et al's 20 series, the navicular and the cuboid in the surgically treated CF were smaller in volume and had smaller articulating surface as previously described by Cahuzac et al. 15 Navicular bones in the CF were also flatter than those in the contralateral normal feet. 20
A cuneiform evaluation in CF patients was done recently by Lang et al 9 who evaluated the length, width and height of the lateral cuneiform using standardized anteroposterior and lateral radiographs showing that the lateral cuneiform on the affected side increased annually in all dimensions but remained smaller than the corresponding dimensions of the unaffected foot. This correlates with previous findings of delayed ossification of the cuneiform bone in the congenital CF 29 (Fig. 4).

Anteroposterior radiographs of both feet taken together of a three-year-old boy with a unilateral (L) clubfoot treated according to the Ponseti method. Note that all ossification centres of tarsal bones can be seen in the non-affected foot (R) but not in the affected foot (L). There is a size different between the tarsal bones of the affected and the non-affected bones.
Segev et al 30 demonstrated in a radiographic study that the measurements of talocalcaneal angles and size of the talus, calcaneus and the first, second and third metatarsals were significantly smaller on the affected side, whereas the values for the fourth and fifth metatarsals were similar on both sides.
Suggested implications
Assessment of the outcome of idiopathic CF treatment with the Ponseti method is very difficult. High quality comparative studies or long-term outcome studies are not available. The overall level of evidence of the published studies is low and uses different rating systems of evaluation. 31
We were able to show that a longer initial bracing phase of the corrected idiopathic CF and a longer night bracing period 32 results in reduction of the number of operations and thus improvement in the functional score. Attainment of walking in children with idiopathic CF following Ponseti treatment is a major concern of parents. In our study, the average walking age was 15 months; 88% of our children start independent walking before 18 months of age. This may question the significant influence of the length of FAB use during the first year of life on the initiation of walking.
Better criteria must be defined in order to identify good versus bad responders to the Ponseti method. We need to develop an agreed upon optimal bracing protocol based on severity and response to Ponseti casting phase adapted to the child themselves rather than using a general scheme. We must better understand that the diversity inbetween idiopathic CF children must be reflected in better suited personalized bracing recommendations. We want to point out the need for a well performed prospective multicentre studies in this area. These will provide better guidelines for the future.
Footnotes
RG: Collecting and analyzing the information, reviewing the manuscript.
SW: Collecting and analyzing the information, reviewing and editing the manuscript.