
Abstract
Abstract
Purpose
The therapeutic algorithm of paediatric anterior cruciate ligament (ACL) tears remains controversial. The primary aim of the study was to describe variations in practice patterns among European Paediatric Orthopaedic Society (EPOS) and Pediatric Orthopaedic Society of North America (POSNA) members with respect to management of ACL tears in skeletally immature patients. The secondary objective was to determine the number, type and severity of growth disturbances associated with ACL reconstruction (ACLR).
Methods
An email invitation to complete a 52-question survey was sent to all members of POSNA and EPOS. Data were collected automatically. Descriptive statistics were applied.
Results
In all, 305 (25.4%) surgeon members responded. Only 182 (60%) of the participants treated ACL injuries in skeletally immature patients and completed the survey. A total of 17% of EPOS and 70% of POSNA members recommended ACLR within three months for a prepubescent paediatric ACL tear. In total, 61% of POSNA and 83% of EPOS members recommended ACLR within three months for a pubescent paediatric ACL tear. Epiphyseal tunnels were the preferred technique in prepubescent children (43% at the tibia and 49% at the femur), while transphyseal tunnels were recommended preferentially in pubescent children (85% at the tibia and 63% at the femur). In all, 5.5% of participants reported growth disturbances after ACLR.
Conclusion
Current practice patterns across the Atlantic remain varied and controversial. Consensus remains elusive; as such, research collaboration among societies will be important to develop an evidence-based treatment algorithm. The use of transphyseal tunnels has been reinforced. The number of cases of significant growth disturbance is minimal, yet worrisome.
Level of Evidence
II
Introduction
As the age of onset decreases, the incidence of anterior cruciate ligament (ACL) tears among paediatric patients continues to increase.1–3 This fact is likely due to participation in high-risk athletic activities among young patients, in addition to early sport-specific training and increased recognition of this injury in children. 4 The therapeutic algorithm remains controversial, notably among skeletally immature patients, with respect to indications and timing of surgery, operative technique and graft selection. Surgical management has become the consensus in the recent literature and has been reinforced by the frequent failure of nonoperative management among skeletally immature patients. 5 Multiple authors have suggested that delayed ACL reconstruction (ACLR) until skeletal maturity is associated with an elevated rate of chondral and meniscal injuries and may lead to early osteoarthritis.6–8 However, growth disturbances have been reported and remain a primary concern. Primary nonsurgical treatment with active rehabilitation has been recommended. 9 In a frequently cited survey from 2002, Kocher et al 10 reported most participants favoured initial nonoperative management. Only 16% recommended early operative management among children eight years of age, and 34% among children 13 years of age. In all, 15 cases of growth disturbance were documented, most of which were linked to technical errors including malposition of transphyseal interference screws, over-tensioned graft or oversized tunnels positioned in proximity or through the physis.
Authors from North America have often reported deleterious effects of conservative treatment 5 and delayed ACLR 7 while describing most of the world widely used ACLR techniques.11,12 On the other hand, rehabilitation programmes and satisfactory outcomes from nonoperative treatment were reported in Europe.9,13 The primary objective of our study was to assess the evolution of treatment approaches to ACL tears among skeletally immature patients and to examine the variations among members of Pediatric Orthopaedic Society of North America (POSNA) and European Paediatric Orthopaedic Society (EPOS). The secondary objective was to determine the number, type and severity of growth disturbances correlated with surgical reconstruction of the ACL.
Materials and methods
An electronic questionnaire comprised of 52 questions was designed and made available on SurveyMonkey online survey software (San Mateo, California, USA) (see supplementary material). This practical survey aimed to elucidate contemporary management with respect to therapeutic approach, surgical technique, graft type, follow-up duration and growth-related complications encountered among skeletally immature patients. Growth disorders were sorted according to Chotel classification. 14 Questions were selected in order to best capture the current scope of the paediatric field on the subject. The relevance of the questionnaire was validated by using a sample of ten paediatric orthopaedic surgeons. An invitation to participate in the survey was sent via email to members of POSNA and EPOS in September 2016. If a member did not respond within the week, a second email invitation was sent, followed by a third invitation during theird week. In cases when the participant answered ‘No’ to the second question, ‘Do you treat ACL injuries in skeletally immature patients?’, the questionnaire stopped there. Participation was voluntary and responses were kept confidential. Data were collected automatically by SurveyMonkey. Descriptive statistics (mean with sd for continuous variables and frequencies with proportions for categorical data) were used to summarize recorded variables. Statistical analysis was conducted using R (version 3.3.2, R Core Team 2013, R: A language and environment for statistical computing; R Foundation for Statistical Computing, Vienna, Austria).
Results
The participation rate was 25.4% (23.2% for EPOS and 29.3% for POSNA), which amounted to a total of 305 responses. Among the participants, 27.5% were members of EPOS, 65.9% of POSNA and 6.5% were members of both societies. In all, 123 (40%) participants did not treat ACL injuries in skeletally immature patients, thus ended the survey after the second question. In all, 72% of 182 remaining participants primarily practised Paediatric Orthopaedics, 29% of whom performed at least ten surgical ACLRs in skeletally immature patients per year and 16% performed over 20. The mean age of their youngest patient who underwent operative intervention was 9.29 years (2 to 15).
When asked what treatment they recommended for a skeletally immature patient with an ACL tear, 60% of respondents recommended surgical reconstruction within three months for children aged eight years (prepubescent) and 79% recommended similar treatment for children aged 13 years (pubescent). There was, however, disparity in responses across societies (Fig. 1). In an eight-year-old individual, overall 43% of respondents recommended epiphyseal tibial tunnel placement and 47% of POSNA members used the ‘over-the-front’ technique. On the femoral side, 49% of respondents recommended epiphyseal tunnels, 40% preferred the ‘over-the-top’ technique,and 11% used transphyseal tunnels (Fig. 2). For 13-year-old children, there was a majority of transphyseal tibial tunnel placement (85%) as well as transphyseal femoral tunnel placement (63%) (Fig. 3). Autologous hamstring tendons were the preferred graft for both prepubescent (53%) and pubescent (85%) children. Iliotibial band autograft was used by 37% (46% of POSNA members) of respondents while 5.3% preferred allograft. The most frequently utilized fixation method among prepubescents was cortical buttons on both sides (42% tibial, 53% femoral). Among pubescent children, preferred fixation methods were an interference screw on the tibial side (50%) and cortical button on the femoral side (72%). Intraoperative fluoroscopy was used by 77% of respondents.
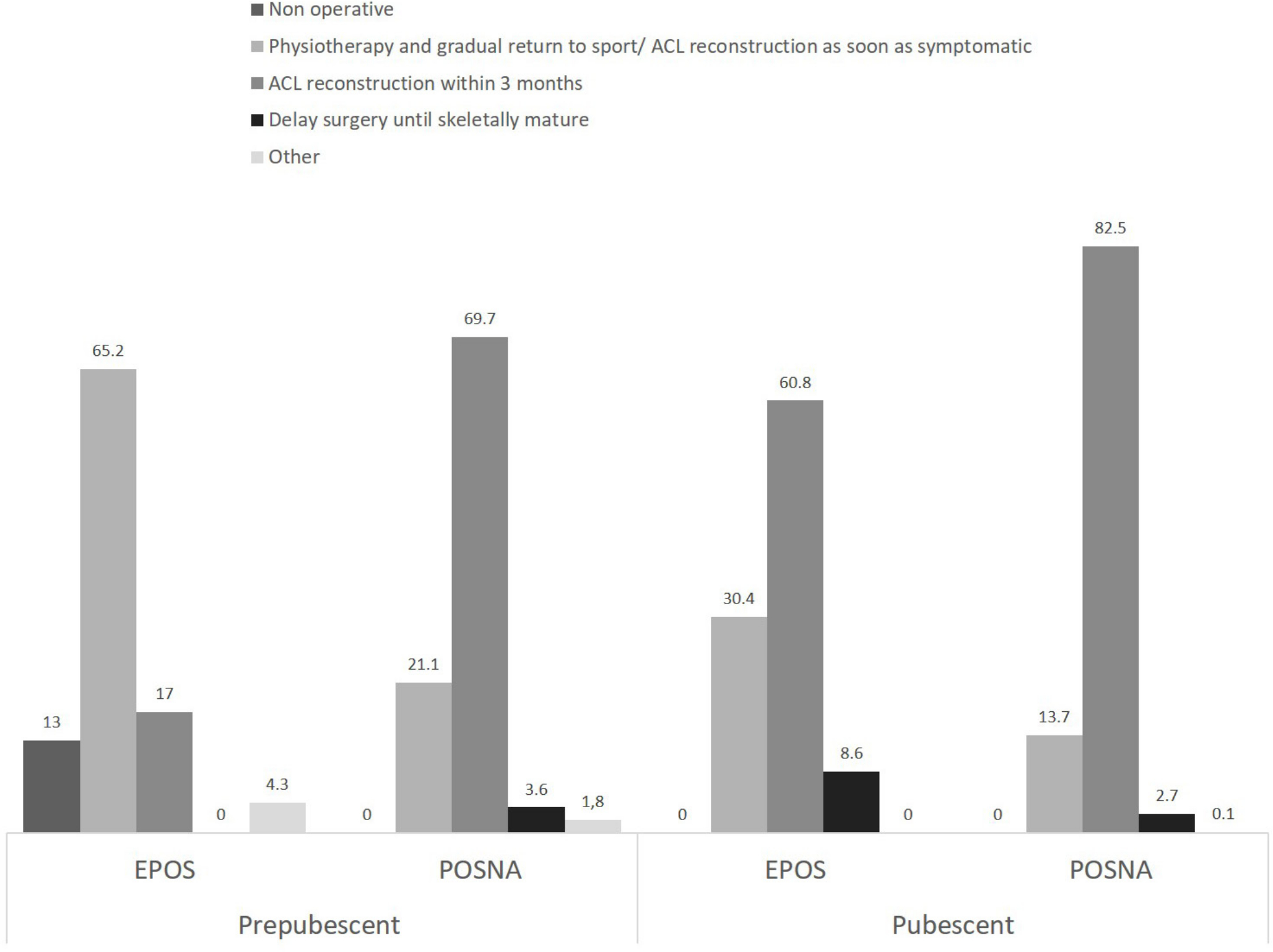
Distribution of the recommended treatment for a paediatric anterior cruciate ligament (ACL) rupture (EPOS, European Paediatric Orthopaedic Society; POSNA, Pediatric Orthopaedic Society of North America).
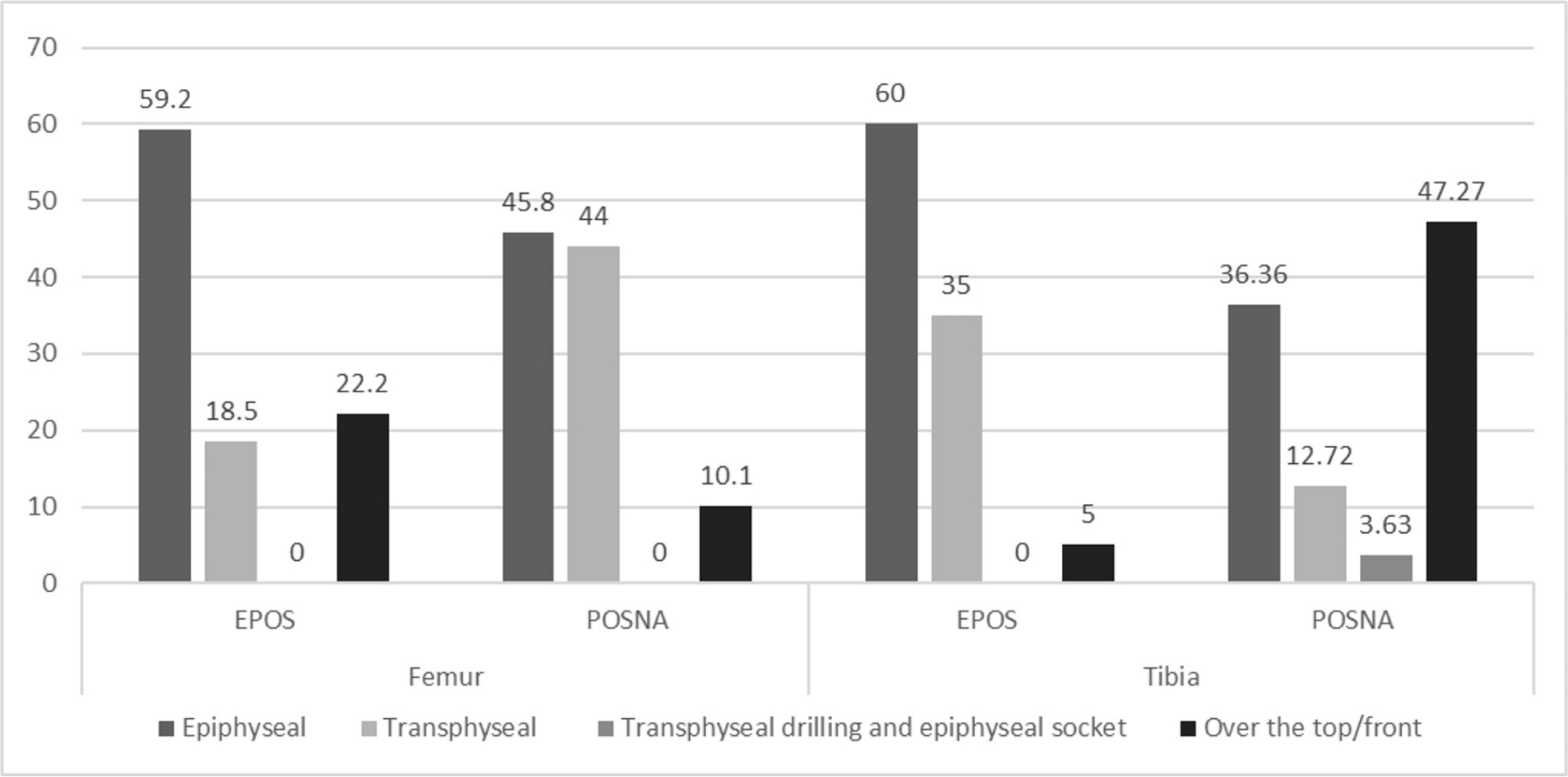
Preferred tunnels for anterior cruciate ligament reconstruction in a prepubescent child (EPOS, European Paediatric Orthopaedic Society; POSNA, Pediatric Orthopaedic Society of North America).
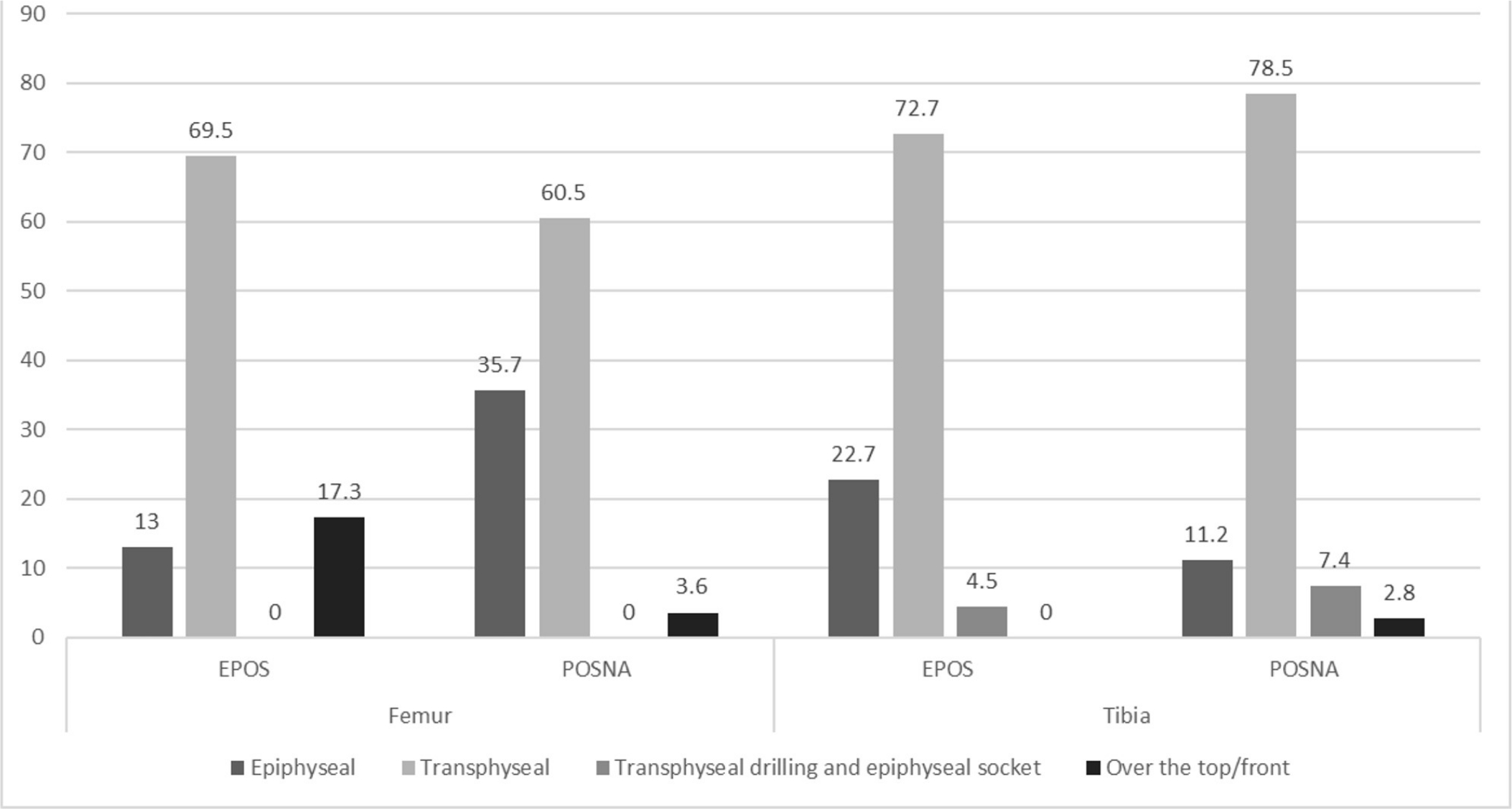
Preferred tunnels for anterior cruciate ligament reconstruction in a pubescent child (EPOS, European Paediatric Orthopaedic Society; POSNA, Pediatric Orthopaedic Society of North America).
In all, 5.5% of participants reported clinically relevant growth disturbances, defined as leg-length discrepancy (LLD) > 1 cm and/or axial deviation > 5°, primarily on the femoral side (33 versus 22 tibial cases). There were five cases of LLD > 2 cm, one case of varus > 10°, six cases of valgus > 10° and two cases of recurvatum > 10°, all in comparison with the contralateral limb. There were 20 reported cases of growth arrest/bone bars (Chotel type A), 16 of overgrowth (Chotel type B) and six of tension band effect (Chotel type C). A total of 54% of participants systematically performed preoperative standing full-length lower limb radiographs and 56% of patients were observed until skeletal maturity. Preoperative physiotherapy was recommended by 56% of respondents, while 76% recommended postoperative rehabilitation according to a standardized protocol. In total, 65% recommended postoperative immobilization in extension.
Discussion
This survey allowed us to gather data regarding the evolution of surgical practice over the course of the last 15 years. Early surgical ACLR is now a key element in the therapeutic algorithm with respect to management of ACL ruptures among skeletally immature patients, including prepubescent children. 15 The dichotomy between eight-year-old and 13-year-old children allowed us to identify an evolution towards transphyseal tunnel placement in pubescent children.Even though growth disturbances are still reported, monitoring for the appearance of this complication is far from systematic with only half (54%) of respondents performing preoperative standing radiograph of the lower limbs and 56% following the operated patient until skeletal maturity. Currently reported rates are relatively low, but the incidence is likely underestimated.
In 2002, among members of the Herodicus Society and ACL study group interviewed by Kocher et al, 10 16% recommended early surgical management of ACL tears in eight-year-old children, while 34% recommended the same management in children who were 13 years of age. In light of failures of nonoperative management reported in the literature, more surgeons now favour early surgical management of these injuries regardless of patient age, according to a recent survey of high volume paediatric ACL surgeons from the Paediatric Research in Sports Medicine group. 16 Aichroth et al 5 described a prospective series of 23 patients managed nonoperatively and reported a decrease in Tegner scores from 6.7 to 4.2 and in Lysholm scores from 78.6 to 52.4 at four years of follow-up (1 to 8). 5 In addition to the poor compliance of the paediatric population to sport activities restriction, recurrence of instability after nonoperative treatment often leads to secondary cartilaginous and meniscal tears, and eventually early onset osteoarthritis. Lawrence et al 7 demonstrated that time, tested as a continuous variable, between the traumatic event and surgical reconstruction was a significant risk factor for medial meniscus secondary injury. Vavken et al 17 confirmed these results in their series which reported an increase in the prevalence of meniscal and chondral lesions by 6% per month of delay from the time of injury to surgical intervention. In a large, prospective series by Moksnes et al, 13 40 patients underwent algorithm-based nonoperative treatment; 19.5% developed new meniscal injuries at a mean four-year follow-up, 33% required surgical reconstruction of the ACL for symptoms of instability, 46.2% of which also had meniscal lesions. Early reconstruction is, therefore, advocated to prevent secondary meniscal tears. 8 Non-surgical treatment is only viable and safe in selected skeletally immature patients who do not have associated injuries or major instability problems, and under close monitoring. 18
The use of transphyseal tunnels for graft fixation has been reinforced in recent years. Kocher et al 10 reported rates of 79% and 50% respectively, for transphyseal tibial and femoral tunnels among skeletally immature patients regardless of age. Moksnes et al, 19 in a survey of European Society for Sports Traumatology, Knee Surgery and Arthroscopy members in 2015, had already identified this evolution when they reported a 91% rate of transphyseal tibial tunnel placement as well as a 67% rate on the femoral side. Patel et al 16 have investigated current practices in the management of ACL injuries in adolescents at each year of skeletal age from eight to 15 years. Significant variation was found in the preferred surgical technique for male patients aged 11 to 14 years and female patients aged 11 to 13 years. In these patients, respondents with paediatric orthopaedic training tended to prefer an all-epiphyseal reconstruction, while those with both paediatric and sports medicine training preferred the modified MacIntosh. Overall, the modified MacIntosh was the most commonly used technique in patients aged eight to ten years. The all-epiphyseal technique was preferred over a broader age range in male patients than female patients, with peak use at age 11 years in both. The transphyseal technique was most widely used in female patients 13 years and older and in male patients 14 years and older. 16 The current results are consistent with these studies, with slight variations between POSNA and EPOS. Overall volume of injury to the physis can be < 5% of the physeal volume, 20 although it increases when using a femoral independent tunnel drilling technique. 21 Several animal studies have demonstrated that transphyseal soft-tissue graft placement prevents formation of a permanent bone bridge at the level of the physis.22,23 In a recent review of the literature, Collins et al, 24 presented 39 cases of growth disturbances described in 21 studies, among which 25% of LLD and 47% of axial deviations were associated with physeal sparing techniques despite a majority of transphyseal tunnels (54% tibial and 77% femoral). Similarly, a meta-analysis reported a mean LLD rate of 1.8% among 55 studies with, paradoxically, a significantly increased risk among physeal sparing techniques compared with transphyseal techniques (5.8% versus 1.9%). 25 This could be explained by the epiphyseal tunnels being close and tangential to the growth plate and thus being more likely to damage the resting cells and the perichondral ring. Pierce et al, 26 however, performed a systematic review which revealed similar incidences of LLD and re-rupture rates between transphyseal and physeal sparing techniques. These data support the use of transphyseal techniques, even among prepubescent children who have more potent physes. 27
Hamstring autograft remains the preferred graft for most surgeons (65.2% of EPOS and 79.8% of POSNA members). However, quadruple semitendinosus tendon autograft presents the advantages of sparing the epiphyseal bone stock, limiting the diameter of transphyseal tunnels and sparing the gracilis tendon which might decrease persistent hamstring weakness 28 and risk for re-tear 29 acquired by sacrificing both tendons, although this remains to be demonstrated. The use of allograft has increased between Kocher's survey in 2002 and the current study amongst POSNA members (5.3 versus 1%). 10 Allograft allows for reduction in donor site morbidity, pain and postoperative oedema as well as duration of the procedure. Recent data in the literature do, however, describe elevated re-rupture and revision rates with this graft.30,31
One of the alarming results of our study was the minimal degree of concern of the participants with following patients for growth disturbances. Performance of systematic preoperative standing radiographs of the lower limbs in addition to observation up until skeletal maturity was only completed in 54% and 56% of cases, respectively. Despite the fact that this method has its limitations, it has been validated in the literature 23 and is practically applicable. 32 Few significant growth disturbances were reported; however, we feel that they were likely underestimated due to the lack of follow-up by approximately half of the participants.
This study is not without limitations. The principal limitation inherent to the methodology is a possibility that the surveyed population is not representative. The questionnaire was only sent to members of POSNA and EPOS. In an effort to limit selection bias, surgeons who do not perform ACLRs in skeletally immature patients were excluded by the first question. Only 53 respondents (29%) performed more than ten ACLRs per year, hence the results may not be reflective of the clinical practice of those surgeons with highest case volume unlike the original article by Kocher et al. 10
Conclusion
Even though no clear consensus has been reached, this study allowed us to observe the evolution of practice over the course of the last 15 years. There is an evolution towards early surgical ACLR via a transphyseal technique. Although they are under-reported, growth disturbances should remain of primary concern for surgeons performing paediatric ACLRs.
Footnotes
Acknowledgements
The authors thank Françoise Auriol and Meagan Tibbo for their precious help.
Thank you to all of the anonymous POSNA and EPOS members who responded to this survey.
GG: Data analysis.
PL: Manuscript preparation.
CTL: Study design.
BEH: Manuscript revision.
MSK: Supervised research.