
Abstract
Abstract
Purpose
The Ponseti method is widely used in clubfoot treatment. Long-term follow-up shows high patient satisfaction and excellent functional outcomes. Clubfoot tendency to relapse is a problem yet to solve. Given the importance of bracing in relapse prevention, we ought to discuss current knowledge and controversies about bracing.
Methods
We describe types of braces used, with its advantages and disadvantages, suggesting bracing schedules and duration. We identify bracing problems and pinpoint strategies to promote adherence to bracing.
Results
When treating a clubfoot by the Ponseti method, the corrected foot should be held in an abducted and dorsiflexed position, in a foot abduction brace (FAB), with two shoes connected by a bar. The brace is applied after the clubfoot has been completely corrected by manipulation, serial casting and possibly Achilles tenotomy. Bracing is recommended until four to five years of age and needs to be fitted to the individual patient, based on age, associated relapse rate and timing when correction was finished. Parental non-adherence to FAB use can affect 34% to 61% of children and results in five- to 17-fold higher odds of relapse. In patients who have recurrent adherence problems, a unilateral lower leg custom-made orthosis can be considered as a salvage option. Healthcare providers must communicate with patients regarding brace wearing, set proper expectations and ensure accurate use.
Conclusion
Bracing is essential for preventing clubfoot relapse. Daily duration and length of bracing required to prevent recurrence is still unknown. Prospective randomized clinical trials may bring important data that will influence clinicians’ and families’ choices regarding bracing.
Level of Evidence
V
Introduction
The Ponseti method has become widely accepted as the method of choice for clubfoot treatment, with long-term follow-up showing high patient satisfaction and excellent functional outcomes.1–3 It involves serial manipulations and casting of the clubfoot, using a specific technique, most frequently combined with a percutaneous Achilles tenotomy and then followed by the use of a foot abduction brace (FAB) to maintain the correction. 4 This brace should be measured and ordered for the child before the last cast is removed, to prevent possible discomfort and non-adherence resulting from not placing the corrected feet in the brace immediately after the last cast is removed. If the brace is not ready, a holding cast should be applied to maintain final correction. This FAB, which holds the feet in external rotation and dorsiflexion, must be worn for 23 hours per day for three months, and for at least ten to 12 hours per night for an additional three to five years.4–6
With the correct application of the Ponseti method and adequate patient adherence, complete correction of a clubfoot can be achieved in 98% of the patients, in as little as 16 days, if using an accelerated casting protocol, or, in most cases, four to six weeks, when performing weekly manipulations and cast changes.6–7
While the casting phase of Ponseti treatment is relatively short and has a quick and noticeable effect on the correction of the clubfoot deformity, the bracing phase lasts for four to five years and, although being an essential part of the treatment, it does not have an apparent dramatic effect on improving the foot appearance or function. Bracing must be done every night, worn full time (23 hours a day) for three months and then at night and nap time (more than ten hours a day) for three to five years. It is mainly the responsibility of the family, and is done with limited clinical supervision, 8 having the potential to become challenging to the child, the family and the healthcare team.
Regardless of the mode of treatment, clubfoot has an inherent and stubborn tendency to relapse. 4 Adherence to the bracing protocol is critical for the long-term success of the treatment, being a better predictor for relapse than severity of the deformity at birth. An up ten-times greater relapse rate has been observed in children of non-adherent families.7–12
Although the Ponseti method is established as the treatment of choice for idiopathic clubfoot, the problem of relapse is yet to be solved. Given the paramount importance of bracing in the success of the Ponseti method and prevention of relapse, we believe that it is pertinent to discuss current knowledge and controversies about braces and bracing wearing protocols.
Types of braces
The most widely used braces in Ponseti treatment are commonly referred to as a ‘Denis Browne Bar’ or ‘Denis Browne Splint’. These braces are an evolution and adaptation of that described by Denis Browne in 1931, 13 stating that maintaining the clubfoot correction “can be obtained by connecting the feet horizontally at the desired angles to the Sagittal plane”. He described “the desired angles” to be external rotations of 20° for unaffected feet and up to 90° for clubfeet.
When treating a clubfoot by the Ponseti method, the corrected foot should be held in an abducted and dorsiflexed position to prevent relapses. This is best achieved by using a FAB, in which two shoes are connected by a bar. If the deformity is unilateral, the external rotation on the affected foot should be set to 60° to 70° and on the unaffected foot to 30° to 40° (Fig. 1). The length of the bar between the heels should correspond to the distance between the child's shoulders. The child's comfort is the main reason for bar length being equivalent to a child's shoulder width.14,15 Recent data showed that racial differences may demand for customization of the FAB dimensions and sizes. 16

A three-year-old boy with a left clubfoot, treated by Ponseti method, and using a foot abduction brace. The external rotation on the left affected is to 60° to 70° and on the right unaffected foot is 30° to 40°.
The bar should be bent to permit 10° to 15° of dorsiflexion. Ideally, one should be able to lengthen the bar or the distance between heels over time, as the child grows. The shoes should be comfortable, straight laced and able to fit both feet, with no curves. 8 Although a brace with shoes that can clip into and out of the bar seems to be easier to use and potentially increase adherence, it may also be more prone to problems related to the clipping pieces.
There are several modern clubfoot braces available on the market, but their use across the world is uneven given that the cost is prohibitive for many patients, particularly in developing countries. 8 The Steenbeek brace (Fig. 2), developed in Uganda by Michiel Steenbeek and David Okello, is made with local tools (leather sewing machine, metal-working equipment, welding tools) and materials (leather, lining, plywood, mild steel rod stock) costs under 10 US dollars and is adequate for Ponseti treatment. 14

The Steenbeek brace, developed in Uganda, is made with local tools, being quite affordable and matching all the requirements for bracing following Ponseti casting.
There are other examples of locally produced FABs in Sweden, Vietnam, Armenia, etc. In some settings, parents themselves have reportedly produced their own home-made braces that consist in most cases of a wood or metal bar with shoes attached at the recommended angles, with good results in terms of preventing relapses. 8 This raises the question of whether there is a real need for the bar to be bent into dorsiflexion.
Several attempts to redesign the FAB have been made, with the goal of improving comfort and increasing the family's and children's adherence to bracing. In the Kessler Brace, the bar has some flexibility to allow the child some ability for plantar flexion during kicking, then returning to the original dorsiflexed position once the child stops kicking. 17
The Horton Click brace (MJ Markell Shoe Co, New York, USA) utilizes a shoe that can be easily ‘clicked’ onto the bar but allows both internal and external rotation of the foot. In Dobb's Dynamic Clubfoot Brace (D-Bar Enterprises, LLC, Saint Louis, USA), the bar allows the child to move both legs independently, but dorsiflexion may be difficult to achieve. The ALFA-Flex shoe (SEMEDA GmbH, Bad-Bodenteich. Germany) is a FAB produced in Europe, with the focus on the comfort and fit of the shoe. It uses non-toxic and biocompatible materials, with a foam mold for the shoe allowing a close, firm fit for the child's foot and provides proper distribution of pressure in the brace. The foam material has both viscous and elastic components. The shoes are easy to put on due to step-in straps. 8 The Mitchell Brace (Fig. 3) was designed under the direction of Dr Ponseti and was initially devised for the treatment of complex clubfeet, given the difficulty of maintaining a good correction with the Markell shoes (C-Pro Direct, Kent, UK). As the Mitchell Brace's shoes are very comfortable for the child, the brace quickly became popular with both patients and healthcare providers and it is widely distributed in developed countries, being quite expensive in many settings. 8

The Mitchell Brace is very comfortable and became popular between patients and healthcare providers, being widely distributed in developed countries.
While some authors have investigated the use of a unilateral ankle-foot orthosis following Ponseti treatment, using a classic ankle foot orthosis (AFO) fixed with Velcro straps 18 or a system consisting of a shoe fixed to a lateral bar spanning the knee at a 90°-angle, fixed by straps at the shank, 19 the results have been discouraging, with a relapse rate of 83% over follow-up periods of 60 months (50 to 72) 18 in the AFO group and 31% of feet, with a follow-up of 25 months (16 to 36) months in other group. 19
Recently, Berger et al 20 have shown that in patients who have recurrent problems of adherence to the treatment with FAB, a unilateral lower leg custom-made orthosis can be considered as a salvage option. Their unilateral lower leg orthosis (LLO) was custom-made with resin and carbon and built in three parts following Baise and Pohlig's 2005 design: 21 a circular foot unit, a lower leg unit and an inner liner made out of Tepefoam. The foot unit fixes the subtalar joint in a valgus position by encasing the calcaneopedal unit, which is then everted in the subtalar joint line by a turning movement by the person who applies the orthosis. Once in place, the ring-like enclosure (completed by a heel cap) works like an external arthrodesis of the subtalar joint. The resulting hindfoot valgus is 10° to 15°. An external rotation of 20° is set and the foot unit is fixed to the lower leg unit by screws and hinges, allowing a range of movement of 0-5-20° plantarflexion/dorsiflexion. Rotational stability of the orthosis in relation to the axis of the knee is mandatory to maintain the position and, therefore, the correctional capacity of the foot unit. This is achieved by mounting the lower leg unit with a combination of ear-shaped supports encompassing the femoral condyles at the proximal ending of the lower leg unit, working as a counter bearing against the rotational forces. The range of movement of the knee joint is not limited by the condylar supports. Further stability is provided by a firm intake of the calf, realized by a Velcro-fixed resin cap above the tibial tuberosity that provides an intake working like a Sarmiento brace. The authors claim that these principles of construction meet the demands of a post-Ponseti brace: 1) stretching of the structures of the posterior and medial ankle and tarsal ligaments and musculo-tendinous units; 2) allowing free kicking (and even walking), and thereby stretching of the gastrosoleus complex.
Berger et al 20 included a total of 45 patients (75 feet) in their study. Compliance with the LLO bracing protocol was 91%. Changing from FAO to LLO at any point during treatment did not result in an increased rate of surgery and caused few problems.
It is important to note that there is a lack of evidence in the literature regarding biomechanical effects of bracing on soft tissues, functionality, patient adherence and outcomes. 8
Bracing daily schedule and overall duration
The FAB is used only after the clubfoot has been completely corrected by manipulation, serial casting and possibly the heel cord tenotomy. All braces that comply with Ponseti's recommendations of shoe rotation and bar length will provide appropriate maintenance of the clubfoot correction as long as the feet are held in the suggested abducted and dorsiflexed positions and the appropriate bracing schedule is followed. Bracing protocol needs to be fitted to the individual patient based on age, relapse rate associated with that age and when the correction was finished 8 (Table 1).
Suggested bracing schedules following Ponseti casting 8
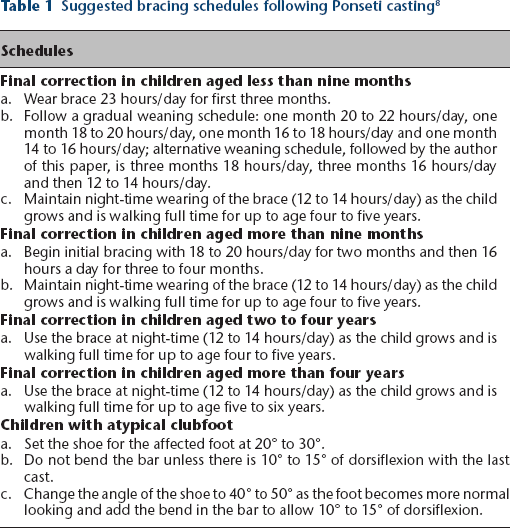
As there is a muscle growth and development problem in clubfoot, it seems important that children using a brace can maintain a degree of mobility during the day. For example, bracing hours will be longer for a newborn that was corrected in three weeks as opposed to an older child that is already walking when correction is achieved. 8
Because of the tendency of clubfoot to relapse up to the age of four to five years, many physicians recommend extending the use of the FAB until this age range. Just by using current knowledge and clinical evaluation skills, it is still not possible to know which patients would experience a relapse at this age if the brace was stopped earlier. 8 The Ponseti International website states that “the rate of recurrence for discontinuing brace wear at the age designated is: first year 90 percent, second year 70–80 per- cent, third year 30–40 percent, fourth year is 10–15 percent, subsequent years are about six percent”, although there is a lack of studies systematically or scientifically investigated recurrence rates after the first two years. 22
Controversy remains regarding the duration of bracing. The Clubfoot Foot Abduction Brace Length of Treatment Study, a prospective randomized-controlled clinical trial whose primary goal is to compare the effectiveness of two- versus four-year night-time brace duration for the treatment of idiopathic clubfoot, may contribute significantly to answer this question. As a multisite study involving eight paediatric orthopaedic surgery clinical sites, enrollment of 139 children was achieved on time in less than three years. Clinical follow-up of patients in both abduction brace duration arms continues for a minimum of five years after brace fitting. 22
Bracing problems
Parental non-adherence with the use of FAB during the course of treatment is a problem that can affect 34% to 61% of children and results in five- to 17-fold higher odds of recurrence of the clubfoot deformity.23–31
Ponseti observed that a relapse often occurs when the child begins to walk, as parents then become less insistent that their child wear the brace as prescribed. It is important that the treating clinician and family understand that walking does not substitute bracing. 4
Although many new brace designs are being proposed and developed, evidence in the literature regarding biomechanical effects, clinical outcomes, functionality and patient adherence is limited. The current research that is available regarding brace design focuses on increasing patient comfort and satisfaction to improve adherence. However, when looking to the future of the Ponseti method and prevention of relapse, brace cost must be addressed and a better understanding of the causes of relapse is needed. Locally produced orthotics with low-cost materials, such as the Steenbeek brace, can provide an option to patients in underprivileged areas and increase adherence and success rate of the treatment. 8
Problems reported by parents of children wearing the FAB include skin injuries (Fig. 4), acceptance difficulties by the child, usually translated into prolonged crying and sleeping problems through the night. 21 The use of comfortable shoes and socks and the institution of a bed-time routine may be useful to establish and promote proper use of the brace and adherence of the families.

Skin injuries are one of the problems which can interfere with family and child adherence to bracing. Education of parents is quite important, so that they can dress the child's feet with adequate socks and properly position the foot in the brace. This two-month-old boy was brought to clinic after two weeks of bracing. The skin injury was due to inadequate socks and difficulties in foot positioning within the brace.
There is a strong correlation between both initial Dimeglio/Bensahel scores and the number of casts required for initial correction and risk for relapse and the need for future surgical intervention.31,32 Initially stiffer feet should be followed with close attention, as they are more difficult to position correctly in the brace, being more likely to slip, causing blistering and irritability that consequently impacts overall bracing tolerance and adherence. 32
Measuring brace wear using parents’ reports may be misleading. By using a method of pressure measurement, which documented FAB wear, Morgenstein et al 33 have shown a significant decline in wear rates from months one to three in the patients of their study, concluding that FAB wear rates did not match their reported rates, thus putting into question previous assumptions about reported brace compliance.
Strategies to improve bracing adherence
The overall probability of a relapsed deformity may reach 52% at age six years, and this probability is significantly reduced by adherence with bracing. 31 If the bracing protocol is correctly maintained, recurrences needing surgery are reported to be around 12%.7,34,35
Since adherence to brace-wearing protocols is essential for preventing relapses, it is important for healthcare providers to communicate with patients regarding brace wearing and to set proper expectations and ensure accurate use. Table 2 describes recommendations that can be presented to parents by physicians, nurses, counselors or other health professionals in order to improve adherence with brace wear.8,36
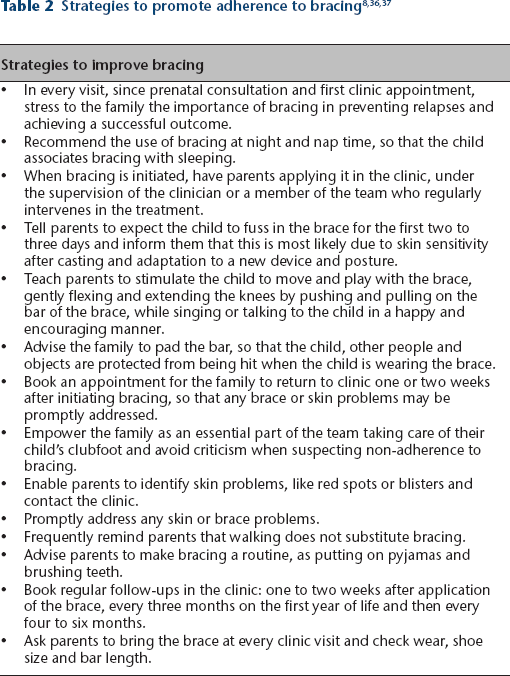
Institutions treating children with clubfeet may benefit from investing in parental education sessions, promoting one-on-one teaching, use of a practice dolls for brace application and having pictures, brochures and videos as supplemental educational tools. These strategies promote and increased understanding of bracing importance, and the ability of families to adhere to the prescribed protocols. 37
Interestingly, despite adherent bracing, some feet seem almost destined to relapse, whereas poorly braced feet sometimes maintain correction over the long term. 38
Conclusion
Foot abduction bracing is essential for preventing relapse in clubfeet treated with the Ponseti method, but the daily duration and length of bracing required is still unknown. The Clubfoot Foot Abduction Brace Length of Treatment Study, a prospective randomized-controlled clinical trial whose primary goal is to compare the effectiveness of two- versus four-year night-time brace duration for the treatment of idiopathic clubfoot, 22 may bring important data that will influence clinicians’ and families’ choices regarding bracing.