
Abstract
Introduction
Only a handful of studies report outcomes after open reduction for developmental hip dislocation beyond skeletal maturity. For successfully reduced hips it is the outcome into late adulthood on which the results of this intervention should be judged. These studies indicate clearly the importance of preservation of the acetabular growth centres during surgery. The acetabulum must also be addressed when insufficient growth remains reliably to remodel residual dysplasia even after stable, concentric reduction.
Summary
Comparing the longest-term outcome studies for open reduction to less invasive, but mainly historical, techniques of gradual traction reduction it is unsettling to note that the latter protocols are associated with the best results. Whereas open reduction and innominate osteotomy are practised as originally described by Salter, gradual traction reduction has largely been abandoned.
Conclusions
There are probably aspects of the more time-consuming methods of gradual reduction that do not violate the hip joint capsule that expose the femoral head to a lower risk of femoral head osteonecrosis leading to better long-term outcomes.
Keywords
Introduction
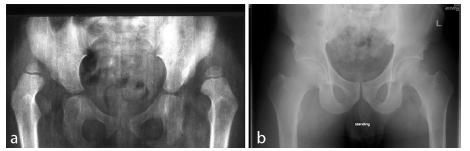
It was 60 years ago that the first cohort of children, aged between 18 months and five years at diagnosis, with congenital hip dislocations were treated by open reduction and innominate osteotomy by the late Robert Salter 1 at the Hospital for Sick Children in Toronto. He had been appointed to the staff there, aged 30, in 1955 after a short fellowship in Oxford, England and two years in a medical mission hospital in the wilds of Newfoundland. Then, 12 years ago, that cohort, then middle-aged (Fig. 1) was traced with the help of a private investigator and an 80-year-old Dr Salter. Patients mainly resided in Canada still. Many remained in their native North American communities of Ontario where there had been a high incidence of hip dysplasia arising from the practice of swaddling newborns on a cradleboard.2,3 Some had migrated as far afield as the United States and Australia, but 80% recall was achieved. The results of that study 4 and others published since are reviewed in this article.
(
Review of methods
Salter had recognized that, with later diagnosis of developmental hip dislocation into the second year of life, contractures of adductor longus and iliopsoas have become established. These and an ‘hourglass’ capsular stricture between the dislocated femoral head and the acetabulum are increasingly likely to block reduction. Completely closed reduction methods at this stage are likely to require traction and progressive abduction,5–8 using the femoral head as a dilating sound against the contracted muscles and capsule. Subjecting the soft, deformable anlage to these forces sits uncomfortably with many surgeons who prefer open releases and capsulotomy at this stage. 9
After a certain period of time, a hip that has been dislocated or is otherwise unstable may not develop normally even after successful concentric reduction by whatever means. Based on his early experience and considerable intellect, Salter believed that a tipping point, in favour of an acetabuloplasty, was reached around the age of 18 months.10,11 Thereafter he recommended the routine addition of an innominate osteotomy, concurrent with open hip reduction, to address established acetabular dysplasia. Subsequent data from Iowa, published some 50 years later, endorse his view. By 18 to 24 months of age the risk of persisting acetabular dysplasia, even after successful reduction, is 35% to 48% and rises thereafter above 50%. 12 Performing an osteotomy, while the pelvis is exposed during open hip reduction, appears very reasonable for those risks.
Salter is best remembered for that innominate acetabular osteotomy that came to bear his name; 10 the principle of which is redirection of the entire acetabulum 13 so that the reduced dislocation that is initially stable in a position of hip flexion and abduction, is made stable in the functional position of weight-bearing (Fig. 2). However, the protocol that he devised also recognized and addressed other important aspects of the condition. Except that preoperative traction is generally now omitted, the same protocol is widely followed today. 14
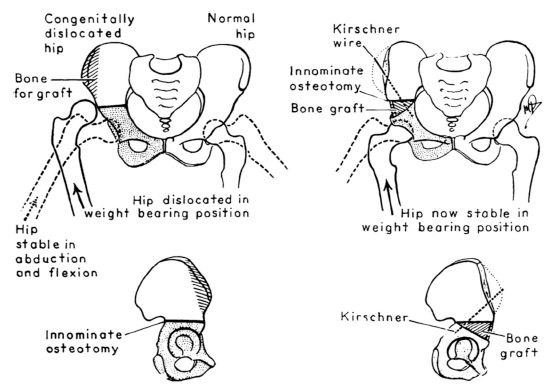
Innominate osteotomy. 10 The base of the triangular bone graft taken from the iliac crest is equal in width to the distance between the anterior superior and anterior inferior iliac spines. This reliably provides 15 degrees of lateral and 25 degrees of anterior coverage. 13 Reproduced and translated from Salter (1961) 10 with permission and copyright of the British Editorial Society of Bone and Joint Surgery.
An alternative philosophy for late presenting dislocations prevailed on the other side of the Atlantic after the Second World War. Edgar Somerville had been appointed a consultant in 1946 in Oxford after Air Force service in the Middle East. 15 He advocated a short period of traction prior to arthrography, excision of the ‘limbus’ through a limited anterolateral approach and derotation femoral osteotomy. He characterized the ‘limbus’ as a substantial and pathological fibrocartilagenous structure, made up of immature acetabular labrum and capsule, that he considered a critical block to reduction. 16
Salter, on the other hand, argued that the labrum contained the growth centres for the acetabular rim, would not block reduction after adequate soft-tissue releases and therefore should always be preserved. Again, this conviction that the growth cartilage should be preserved, was borne out by subsequent scientific study. 17 He advocated open reduction with a more extensive anterolateral approach to release the adductor longus and psoas tendons and open the capsule while preserving the peripheral labrum. The transverse acetabular ligament was incised to increase the volume of the socket and the hypertrophied ligamentum teres was excised. A generous ‘T’-shaped capsulotomy was designed with a limb that runs over the apex of the dislocated femoral head through the elongated false capsule. This enabled excision of a triangle of capsule, made redundant by reduction of the femoral head, converting the ‘T’ to a ‘V’ that, once repaired, should prevent femoral head dislocation. This triple approach, completed by innominate osteotomy, effectively stabilized the hip in the functional position of weight-bearing allowing a reduced period (six to eight weeks) in cast. 14
Comparison of outcomes
The results of Somerville's ‘direct method’ were reported for 120 hips, median age two years at reduction, at skeletal maturity. Good Severin grades (I/II) had been achieved in 59%. 18 At 33 years, 19 50% had moderate or severe arthritis with a 14% rate of hip arthroplasty or arthrodesis. Salter's original cohort, comprising 80 hips in 60 patients aged 18 months to five years at reduction, were graded Severin I/II at skeletal maturity in 90% of cases. 11 They were traced at 45 years and brought back for clinical and radiographic review. 4 At 33 years the rate of hip arthroplasty was much lower at 3.8%. By 45 years survivorship, using hip arthroplasty as an endpoint, had fallen to 54%. One-third of surviving hips had clear radiographic signs of osteoarthritis despite generally good functional scores.
The earlier development of severe osteoarthritis with Somerville's ‘direct method’ of limbus-ectomy is a clear mandate for preserving the immature acetabular labrum during surgical reduction. Poor acetabular development after excision of the labrum was consistent with the Severin grades seen at skeletal maturity in Somerville's series. However, achievement of good Severin grades at skeletal maturity in Salter's series did not uniformly protect against deterioration in the latter part of the 45-year follow-up despite careful preservation of the capsulo-labral rim.
Both Somerville and Salter's series used preoperative traction and reported femoral head osteonecrosis (FHO) rates at skeletal maturity of 13% and 6%, respectively.11,18 These are low compared with subsequent series.20–23 The published rates of FHO vary widely and are dependent on the evaluator's stringency of inclusion, method of evaluation and age of the patient at final follow-up. 21 Put more succinctly, by Dr Weinstein from Iowa, ‘The actual prevalence of FHO may vary less than the means by which it is assessed’. 24
FHO is rightly the most feared complication of intervention for developmental dysplasia of the hip; it is iatrogenic, potentially devastating and largely untreatable. The very lowest rates, 2% to 6%, are reported with closed techniques of gradual traction reduction.5–7 These contradict widely held concerns about applying progressive abduction pressure against the immature femoral head. It is interesting to compare the long-term results of Salter's protocol with those since published by Terjesen et al 5 for a gradual method, now historical in their unit, for 90 hips aged four months to five years at diagnosis (average age 1.7 years). Their protocol was of prolonged traction and abduction for 33 days (16 to 65) with the hips internally rotated towards the end of that period. Closed reduction was then achieved under general anaesthesia and a first hip spica applied with the hips in slight flexion, 60° abduction and slight internal rotation. The spica was changed every three months for 9.5 months (6 to 20). Six early failures were switched to open reduction. In all, 44 hips underwent derotation femoral osteotomy within three years of closed reduction. A further 30 hips underwent late surgery for residual dysplasia: 13 varus femoral osteotomies, 13 shelf procedures and four Salter osteotomies. Since the majority required femoral or acetabular surgery this might be best considered a ‘closed capsule’ method of operative-assisted traction reduction. FHO rate was 10%.
Respecting the capsule in this and other ‘closed capsule’ series5–8 may be critical to the low-reported rates of FHO. By skeletal maturity, 62% in Terjesen's series 5 were Severin grade I/II but at an average age of 52 years only, 23% had undergone hip arthroplasty. A further 10% had osteoarthritis. In those aged over 1.5 years at the time of reduction these figures increased to 33% and 49%, respectively. Survivorship in this group, using joint arthroplasty as the endpoint, was 68% at 50 years. This was better than the Salter series 4 which reported 54% survivorship at 45 years. There was osteoarthritis in a third of surviving hips, although this may well have increased after a further five years of follow-up.
The treatment times, technical difficulties and medical costs associated with a protocol of prolonged traction reduction and cast immobilization are formidable. Extended hospital stays and requirement for personnel with expertise in nuanced traction techniques probably make such methods unfeasible in the United Kingdom, for example, where many parents would baulk at a further nine months in a hip spica compared with six to eight weeks after an operation. Three further caveats are important: pelvic and/or femoral osteotomies are subsequently required in the majority of cases reduced by ‘closed capsule’ methods; comparably low FHO rates are reported in the best of the anterolateral open reduction series;9,11 and there is wide variation in quoted FHO rates for all methods suggesting differences in interpretation and reporting of a subjectively measured outcome. The long-term outcomes after open reduction and Salter osteotomy at 45 years for children aged 1.5 to five years were good; 4 especially so for the first 30 years. Nonetheless, the longest outcome study for this age group reported better survivorship, using hip arthroplasty as an endpoint, for a ‘closed capsule’ gradual traction reduction method 5 compared with anterolateral open reduction. 4
Conclusion
Orthopaedic surgeons are interventional by nature which may explain some of our reluctance to revert to the more traditional techniques reported by Terjesen et al. 5 Techniques of open reduction have not appreciably changed or improved since the Salter cohort had their index intervention. 4 We can therefore give parents of children with late presenting hip dislocations an evidence-based prognosis of expected outcome into middle age. The spotlight should perhaps return to those less invasive, but more time consuming, methods that do not violate the hip joint capsule. The evidence base, albeit limited, indicates marginally better long-term outcomes with a ‘closed capsule’ method that may expose the femoral head to a lower risk of FHO.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
None declared.