
Abstract
Purpose
To investigate the outcomes of an anteverting triple periacetabular osteotomy for the treatment of hip instability in skeletally immature patients with Down syndrome.
Methods
We evaluated 16 patients (21 hips) with Down syndrome and hip instability who underwent an anteverting triple periacetabular osteotomy between 2007 and 2016. There were nine females and seven males with an average age of 7.4 years SD 2.0. We assessed the level of hip pain, gait ability and clinical stability at a minimum of one year after surgery. Radiographic evaluation included pre- and postoperative lateral centre-edge angle (LCEA), Tönnis acetabular angle and extrusion index.
Result
After an average follow-up of 4.1 years SD 2.6, 20 of 21 hips (95%) remained clinically stable. In all, 12 of 16 (75%) patients had a full gait without a major limp, but three patients (19%) had a persistent limp. Of the 21 procedures, one hip (5%) was considered a failure due to persistent instability. There was a mean increase of 18.3º SD 15.3º of the LCEA (p < 0.001); a mean decrease of 15.2º SD 11.6º (p < 0.001) for the Tönnis angle and the extrusion index had a mean decrease of 0.27 SD 0.20 (p < 0.001). The most common complications were minor and included nonunion of the pubis or ischium (24%) and stress fractures of the pubis and ischium (14%). Only one patient required unplanned surgery for the treatment of an infection; which was considered a major complication.
Conclusion
The anteverting triple periacetabular osteotomy provided global deformity correction and achieved hip stability in 95% of the hips after a mean follow-up of 4.1 years.
Level of Evidence
Therapeutic level IV.
Introduction
Hip instability has been reported in up to 7% of patients with Down syndrome.1–4 Although clinical presentation may vary with age, hip instability tends to be progressive, evolving to subluxation, fixed dislocation or residual acetabular dysplasia with potential osteoarthritis development in the long term.1,5 Hip disease in patients with Down syndrome has been associated with high morbidity, with half of the patients losing the ability to walk independently during adult life. 5
In addition to ligamentous laxity and generalized muscle hypotonia,6–8 there is a spectrum of skeletal anatomical abnormalities that might contribute to the hip instability in Down syndrome.4,9–14 Abnormalities of the femur including increased femoral anteversion and coxa valga have been reported and have been described as the rationale for treatment by femoral intertrochanteric osteotomy.4,11,15 However, recent studies have shown that insufficient posterior acetabular coverage14,16 and acetabular retroversion9,16,17 play a major role in the aetiology of hip instability. Surgical treatment by a complete redirectional osteotomy of the acetabulum has been shown to provide stability in a higher proportion of patients when compared with femoral osteotomy alone or combined to incomplete pelvic osteotomies. 17 Previous studies reporting the outcomes of triple osteotomy in patients with Down syndrome were limited to a small number of patients with limited information about success rate, complications and radiographic outcomes.17,18
In this study, we sought to investigate clinical and radiographic outcomes of an anteverting triple periacetabular osteotomy for the treatment of hip instability in skeletally immature patients with Down syndrome followed for a minimum of one year postoperatively.
Materials and methods
This is a single centre retrospective case series study approved by our Institutional Review Board. The inclusion criteria were: 1) diagnosis of Down syndrome; 2) hip instability; 3) skeletally immature patient with open triradiate cartilage in the preoperative radiograph; and 4) treatment by the modified anteverting triple periacetabular osteotomy. The exclusion criteria were: 1) follow-up less than one year; and 2) denied consent by the patient's parents. We identified 17 patients with Down syndrome who had undergone an anteverting triple periacetabular osteotomy for the treatment of hip instability between 2007 and 2016. Parents of one patient denied consent for the research. Five patients underwent bilateral surgery, eight on the right hip and three on the left, yielding a total of 21 procedures in 16 patients (nine girls, seven boys). The mean age (and sd) at the time of surgery was 7.4 years sd 2.0 (4.7 to 12.6), and the mean body mass index percentile was 0.72 sd 0.18 (0.30 to 0.99).
Before surgery, all patients had a history of painless hip instability, although two patients were non-verbal. All hips were unstable in flexion and no reference of instability was noted when the hips were in full extension. All unstable hips were clinically reducible, except for one patient who had a non-reducible fixed dislocated right hip. Two patients (13%) had an associated neurological disorder (both presenting with seizures), and although they were domestic ambulators, they required the use of wheelchair. One of these patients had a unilateral fixed dislocation. Two patients (13%) presented with clunking episodes while walking, associated with falls. The remaining 12 patients (75%) were able to walk independently with a notable limp. Only one patient had a history of bilateral previous surgery, which included open reduction, capsuloplasty, shelf acetabuloplasty and femoral varus derotational intertrochanteric osteotomy, but the left hip remained unstable.
Postoperative notes were reviewed to assess clinical hip stability, complications and any further additional hip surgery besides implant removal. Complications that did not change the postoperative course and complications that required pharmacological treatment or close monitoring were considered minor complications. 19 Complications requiring inpatient or invasive treatment, those involving high morbidity and risk of residual disability and death were considered major complications. 19
The radiographic parameters were measured in the anteroposterior and false-profile 20 views in the preoperative radiograph, early postoperative (up to three months after surgery) and latest radiograph. Preoperatively, the triradiate cartilage was wide open in all hips and in ten out of 21 (48%) hips the arch of Shenton was discontinued. No patient had hip osteoarthritis on preoperative radiographs according to the Tönnis grading system. 21 Radiographic measurements included the lateral centre-edge-angle (LCEA), 22 Tönnis acetabular angle 21 and extrusion index. 23 In hips with severe subluxation or frank dislocation, the Visser method 24 was used for LCEA measurements. In the latest postoperative radiographs, the ilium, ischium and pubis osteotomies were classified as complete bone healing or nonunion.
Surgery was performed by one of the two senior authors (Y.-J.K, E.N.N) according to a previously described technique. 18 Briefly, a medial approach is performed with a longitudinal incision over the posterior border of the adductor longus which is retracted anteriorly. The anterior branch of the obturator nerve is protected and the nerve is traced to the obturator foramen. The pectineus muscle is retracted proximally and the ischium is palpated. A blunt retractor is placed medially toward the ischial spine using fluoroscopic guidance (Fig. 1a). Similarly, a lateral window is created with the blunt elevator to protect the sciatic nerve. A complete oblique osteotomy of the ischium is performed using a modified Ganz-type chisel toward the greater sciatic notch, above the ischial spine and sacrospinous ligament (Fig. 1b). Using an oblique anterior hip approach, the muscular fascia of the tensor fascia lata is opened parallel to the interval between the sartorius and tensor, avoiding the exposure of the lateral femoral cutaneous nerve. Dissection is carried out through this interval to the direct rectus origin. The aponeurosis of the abdominal external oblique muscle is released from the iliac apophysis, which is divided and the medial wall was exposed. The iliopsoas muscle is retracted medially and the superior pubic ramus is exposed while preserving the periosteum intact. The pubic osteotomy is performed with a Gigli saw at the lateral limit of the obturator foramen. The supra-acetabular osteotomy is performed with an oscillating saw up to 1 cm of the pelvic brim. An angle chisel completes the iliac osteotomy towards the sciatic notch. A 3.5-mm Schanz screw is inserted in above the anterior inferior iliac spine. The completely free acetabular fragment is anteverted and adducted to correct the posterior acetabular deficiency (Fig. 1c). The degree of acetabular anteversion depends on the hip stability. Typically we correct the fragment into anteversion to the point that the posterior wall is lateral to the centre of the femoral head. Hip stability is tested in flexion and internal rotation. If the hip persists with instability, further anteversion is performed. Fixation is performed with a minimum of three 3.5 mm cortical screws. Stability of the hip is tested flexing and internally rotating the hip (Fig. 1d). A spica cast (18/21 hips) or an above-knee immobilizer (3/21 hips) was applied for six weeks postoperatively and a night-time abduction brace was recommended up to the sixth month postoperatively. Currently, we prefer the use of the spica cast to assure a safe hip positioning. In addition to the triple osteotomy, open reduction, capsuloraphy and femoral varus derotational osteotomy were performed to help achieve a concentric reduction in the one hip that remained subluxated after triple osteotomy. For the only patient with a preoperative non-reducible hip, it was possible to reduce the hip under anaesthesia after the triple osteotomy with no need for arthrotomy and capsuloraphy. This hip was posteriorly stable in internal rotation, but with slight subluxation in external rotation. A femoral derotation osteotomy was required to improve stability. For a total of three hips in this series, a femoral intertrochanteric varus and derotation osteotomy was performed to decrease the excessive femoral anteversion and improve the hip stability, when a residual intraoperative instability was observed after the triple osteotomy. The excessive femoral anteversion was identified after the completion of triple osteotomy, when the hip was anteriosuperiorly unstable in external rotation of the femur. The mean estimated blood loss (and sd) for the procedure was 151 mL sd 95 (50 to 500). The mean surgical time was 2.9 hours sd 1.4 (2.0 to 8.0), including casting and femoral osteotomy when present.
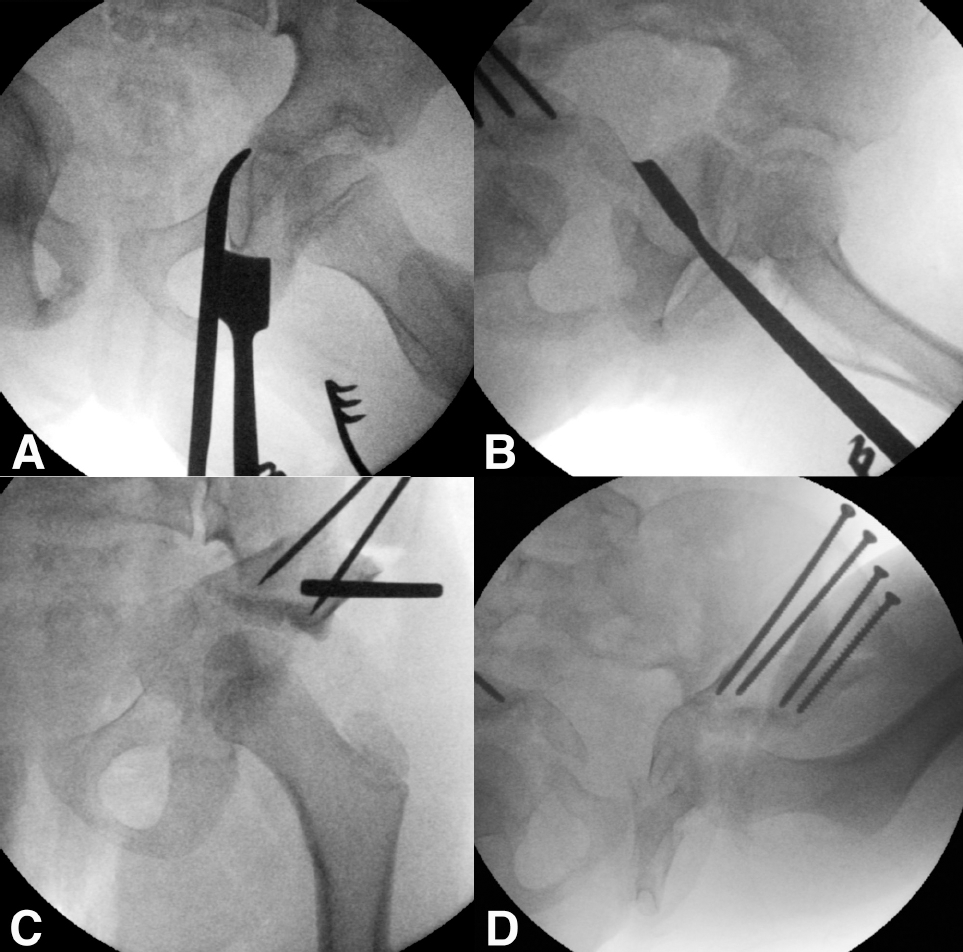
Anteverting triple periacetabular osteotomy in a girl with Down syndrome and left hip instability: (
The antibiotic prophylaxis consisted of the use of endovenous cefazolin 25 mg/kg (18 of 21 hips, 86%) or clindamycin 10 mk/kg (three hips, 14%). We followed the regular recommendation of our institution, with no need for extra antibiotic coverage.
A total of 15 of 21 hips (71%) in this series had more than two years of follow-up.
Statistical analysis
A descriptive analysis was presented for demographic data. To address repetitive bilateral measurements, and measurements collected for the same subjects across time, generalized estimating equation regression models were used for group comparison testing such as pre-surgery versus post-surgery. For the progression of arthritis estimation, Tönnis grades 2 and 3 were used to define the presence of arthritis, and grades 0 and 1 as absence of arthritis. A p-value < 0.05 was considered statistically significant. SAS software (version 9.4, SAS Institute, Cary, North Carolina) was used for the analysis.
Results
Patients were followed for a mean of 4.1 years sd 2.6 (1.0 to 8.9), and the mean age at final follow-up was 11.7 years sd 3.9 (6.9 to 20.4). A total of 20 (95%) out of 21 hips were stable without episodes of instability at final follow-up, including the hip with preoperative fixed dislocation. Postoperatively, one hip out of 21 was occasionally painful, and the other 20 hips had no specific pain or discomfort. A total of 12 patients (75%) were walking without an obvious limp or requirement for assistive aids, while three patients (19%) had a slight limp, and one patient (6%) required a walker as an assistive mobility device.
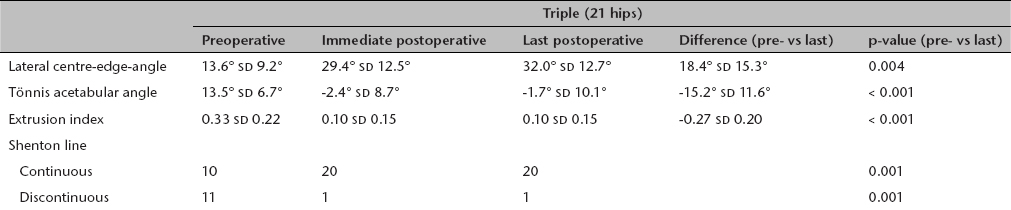
Radiographic improvement was observed when comparing measurements on the preoperative radiograph with those from the immediate postoperative and last follow-up (Table 1). There was a mean increase of 18.3º sd 15.3º on LCEA (p < 0.001). The Tönnis angle showed a mean decrease of 15.2º sd 11.6º (p < 0.001) and the extrusion index had a mean decrease of 0.27 sd 0.20 (p < 0.001). There was no significant difference between immediate postoperative and final follow-up measurements on LCEA, Tönnis angle and extrusion index (p > 0.05 for all comparisons), suggesting a permanent correction. There was no significant progression on the Tönnis grade of arthritis (p = 0.13) (Fig. 2).
Radiographic parameters described as means and sd in hips that underwent anteverting periacetabular triple osteotomy, and hips without the triple osteotomy. Frequency was described for the Shenton line
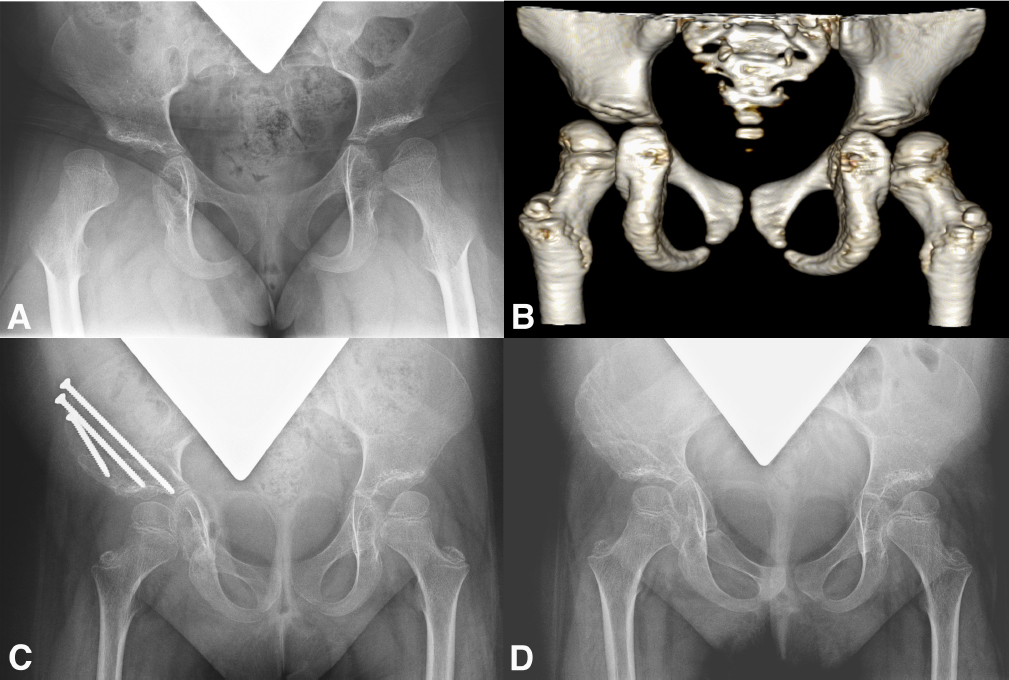
Female patient with Down syndrome and right hip instability, characterized by habitual dislocation with non-concentric reduction, who underwent the anteverting periacetabular triple osteotomy with excellent clinical and radiographic outcomes: (
As minor complications, we identified three (14%) of 21 hips with transitory instability during the early postoperative follow-up, but the instability spontaneously resolved with conservative treatment (an abduction brace at night time for the first six months after surgery). One of 21 hips (5%) had a superficial infection treated with oral antibiotics and wound care. The same hip had a mild a transient finding of radiographic lucency in the femoral head that did not require treatment changes and did not compromise the femoral head sphericity. One hip had isolated ischium nonunion, one had isolated pubis nonunion, and three hips developed combined ischium and pubis nonunion, for a total of five out of 21 (24%) hips with nonunion. Stress fractures were observed in three (14%) of 21 hips, and a stress reaction over the ischiopubic synchondrosis was found in seven hips (33%). Nonunions and stress fractures were asymptomatic and we could not find a clinical correlation with a pain or other specific symptom. One (5%) of 21 hips presented with a major complication, characterized by a deep infection, requiring a single surgical drainage and endovenous antibiotics with satisfactory evolution. There was a complete resolution without further complications.
One (5%) of 21 hips was considered a surgical failure seven years after triple osteotomy. Before triple osteotomy, this patient had undergone bilateral capsule plicature, shelf acetabuloplasty and femoral varus derotational osteotomy, which failed to stabilize the hip, and subsequently underwent triple osteotomy on the left hip that progressed to residual acetabular dysplasia, subluxation and osteoarthritis (Fig. 3). This patient was a household ambulator before the triple osteotomy and required a stroller for mobility according to the last follow-up. Nevertheless, there was no complain of pain and a revision surgery has not been performed at the time of writing.
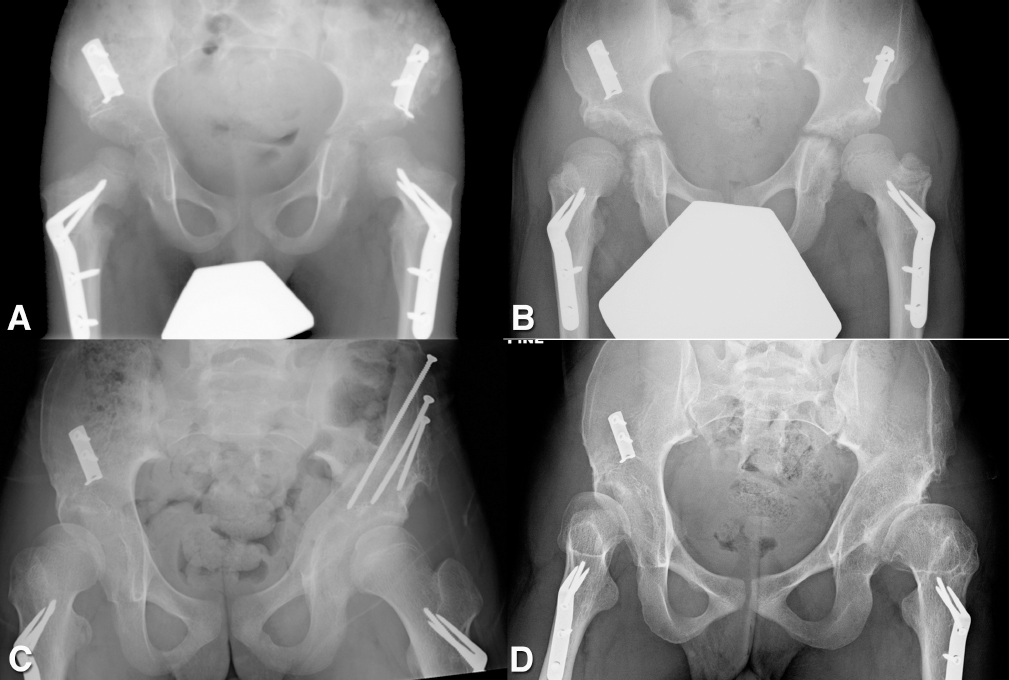
Male patient with Down syndrome and associated neurologic disease, presenting initially with bilateral hip instability, and prior femoral osteotomies and shelf acetabuloplasty. The left hip remained unstable, and underwent the anteverting periacetabular triple osteotomy: (
Discussion
Surgical treatment of hip instability in patients with Down syndrome is challenging, controversial and associated with a high rate of complications. In this study, we investigated the preliminary results of an anteverting triple periacetabular osteotomy in 16 patients (21 hips). After a mean four years, 20 out of 21 hips (95%) remained stable without the requirement of revision surgeries for instability and most patients were walking independently with minimal symptoms. However, one-quarter of the hips had a nonunion of the pubic or the ischial osteotomy.
Hip instability occurs in only 7% of patients with Down syndrome.1–4 Given its rarity, there are few studies reporting the results of treatment and most included a limited number of patients. Although Greene 25 reported successful results in a five-year-old patient treated with prolonged immobilization in abduction bracing and a four-year-old treated with casting and bracing, one study 1 reported a high rate of failure with non-surgical treatment. Bennet et al 1 showed that following closed reduction and casting, four of five children had persistent hip instability.
Surgical management is the mainstay of treatment of hip instability in Down syndrome. In the past, several surgical strategies including capsular plication, femoral osteotomy and pelvic osteotomy were reported to not only fail to systematically stabilize the unstable Down hip but also to be associated with a high rate of complications.1,2,4,10,11,15,26 The rarity of this problem, the lack of complete understanding of the anatomical factors leading to instability and the inexistence of a surgical treatment algorithm make treatment of hip instability in Down syndrome a difficult task for the paediatric orthopaedic surgeon. Although generalized muscle hypotonia and ligamentous laxity may play a role, the hip is a deep and tridimensional complex joint whose stability is mostly influenced by the cartilaginous and bone anatomy. One study 8 reported no relationship between ligamentous laxity and the migration of the hip, suggesting that the joint laxity may not be the major risk factor for hip instability in Down syndrome. Hence, isolated soft-tissue procedures including capsular plication have a limited role. Gore 27 reported a case treated by a posterior capsular plication with good stability and acetabular development two years after surgery. However, this patient ended up with hip subluxation and osteoarthritis in long-term follow-up. 26
Conflicting data exist regarding the underlying anatomical abnormalities leading to hip instability in Down syndrome. Femoral deformities including coxa valga have been reported, 11 however one study showed that the valgus appearance of the proximal femur is a consequence of excessive femoral anteversion. 4 A recent tomographic study using reformatted images through the anatomical axis of the femoral neck, showed no difference in the neck-shaft angle between patients with Down syndrome and matched-control individuals. 16 Recent evidence suggested that the acetabulum is retroverted in Down syndrome, leading to an insufficient posterior support to the femoral head.9,12,16 One study described the posterior acetabular wall as deficient and aggravating the retroversion of the acetabulum, leading to further posterior hip instability. 14 A recent study reported a global insufficiency of the acetabulum in patients with Down syndrome and hip symptoms, and that the acetabulum is more retroverted and shallower compared with healthy individuals. 16
Considering that the main factors leading to instability are the morphology of the acetabulum and femur, it is intuitive to believe that combined femoral and pelvic osteotomies would successfully stabilize the Down syndrome hip. However, one study reported a higher rate of failure of femoral and pelvic osteotomy compared with a complete redirectional osteotomy of the acetabulum. 17 Further, Bennet et al 1 reported the results of 18 patients treated with single or combined procedures including closed or open reduction, casting, capsular plication, femoral and pelvic osteotomies. Dislocation or subluxation occurred in 11 of 24 hips (46%), and a proportion (19%) of patients developed infection. Aprin et al 10 reported on six patients treated by isolated or combined femoral varus osteotomy, Salter innominate osteotomy and capsular plication. Three of the six patients required further surgery to stabilize the hip, and at the final follow-up, two patients had hips with subluxation. Failure associated with the Salter, Pemberton or Dega pelvic osteotomies may occur because they were designed to improve anterior and lateral coverage of the femoral head typically secondary to developmental dysplasia of the hip and do not correct the posterior deficient acetabular coverage found in Down syndrome. In order to increase posterior coverage of the femoral head, Woolf and Gross 14 described a modification of the Pemberton osteotomy in the treatment of two patients with successful stabilization of the hip.
Isolated intertrochanteric osteotomy for varization of the proximal femur has recently been reported to achieve hip stabilization when performed in young patients (aged seven years or younger). 11 Knight et al 11 reported stabilization of the hip in nine patients (16 hips) treated by a femoral osteotomy to create 105o of varus combined with derotation, with a minimum follow-up of 3.8 years. Two hips required further periacetabular osteotomy to achieve stabilization. A relatively high rate of complications, including peri-implant femoral fractures (12%), varus bowing of the femur (88%), arthritis (6%) and persistent abductor insufficiency gait (6%) were noted.
In our study, 20 (95%) out of 21 hips were stable at an average of four years following the anteverting triple periacetabular osteotomy. Two previous studies discussed the role of a complete redirectional periacetabular osteotomy to stabilize the hip in Down syndrome.17,18 Rebello et al 18 described the technique of the anteverting triple osteotomy for the treatment of neuromuscular hip dysplasia including two patients with Down syndrome. Sankar et al 17 noted that complete redirectional periacetabular osteotomy, including five hips treated by a triple osteotomy, achieved hip stability in 92% of the patients compared with 50% of patients treated with femoral osteotomy with or without incomplete acetabuloplasty. In this study, stability was achieved in most patients, however, we found a relative high proportion of asymptomatic nonunion of the ischium and pubic osteotomies and stress fracture around the ischiopubic synchondrosis. We believe that the high rate of nonunions is secondary to the substantial amount of internal rotation and/or adduction of the acetabular fragment, leading to a rotational diastasis at the ischium and pubis osteotomy sites. Although no specific treatment was required for nonunions, recently we recommend adding bone grafting to the pubis and ischium to reduce the risk of nonunion.
This study has some limitations. First, this is a preliminary report of the application of triple pelvic osteotomy for hip instability in Down syndrome and further follow-up is recommended to determine the long-term outcomes of the triple osteotomy. We acknowledge that most patients in this study have not reached skeletal maturity age and we plan to follow these patients in the future to determine whether the short-term stability achieved with the triple osteotomy is maintained in the long-term. Secondly, considering the long period of this study it is possible that an evolution of the surgical technique and surgeon's learning curve may have impacted our findings. Thirdly, given the low prevalence of hip instability and Down syndrome we were limited to a retrospective, relatively small case series study without a control group for comparison. Finally, although stability was achieved in the vast majority of patients, three out of the 21 hips (14%) required a femoral osteotomy. Further research is necessary to clarify the pathomorphology of the hip in Down syndrome and the factors associated with instability development. Currently, we recommend a preoperative tridimensional study of the hip using MRI or CT in order to achieve satisfactory understanding of the complex hip anatomy in these patients.
Treatment of hip instability in Down syndrome is challenging and controversial. Although one recent study 11 reported that a high proportion of hips were stable following an isolated femoral varization osteotomy, we prefer surgical correction of the posterior acetabular deficiency associated with acetabular retroversion.9,12 This study demonstrates that an anteverting triple periacetabular osteotomy improves the global acetabular deformity and achieves short-term hip stability in Down syndrome unstable hips with a relative low rate of major complications. However, a relatively high proportion of patients developed nonunion or stress fracture of the pubis and ischium. Further, our results are limited to short-term assessment of stability. Future multi-centre, long-term prospective studies comparing the anteverting triple periacetabular osteotomy versus femoral varus osteotomy will be necessary to determine the best strategy to achieve hip stability with the lowest rate of complications in patients with Down syndrome.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Y.-J. Kim has received honoraria from Orthopediatrics. D. A. Maranho received a post-doctorate scholarship (Grant 2016/04376–3) from the São Paulo Research Foundation (FAPESP). All other authors have no conflict of interest to declare.