
Abstract
Purpose
Describe the surgical technique of talocalcaneal coalition resection using live CT navigation.
Methods
A ten-year-old female with left talocalcaneal coalition hindfoot pain refractory to conservative management underwent surgical coalition resection using live CT navigation. The procedure and discussion of this technique is described in detail.
Results
With minimal radiation exposure to the patient, CT navigation for this complex talocalcaneal coalition was both helpful and potentially timesaving by allowing immediate localization and guided resection of the coalition.
Conclusion
In the case of a complex subtalar coalition resection, CT navigation poses minimal patient radiation exposure and allows immediate localization and guided resection of the coalition.
Level of Evidence
Level V
Introduction
Tarsal coalition is felt to be the result of failed segmentation of the primitive hindfoot mesenchyme during development. This subsequently results in failure of normal joint formation and subtalar stiffness. 1 Tarsal coalitions have a prevalence of 1% to 2% and should be suspected in preteen or teenage patients presenting with insidious or acute onset of hindfoot or midfoot pain and an associated decrease in subtalar movement.1,2 Initial workup should include plain radiographs that may reveal characteristic findings of a tarsal coalition (C-sign, talar beak sign, anteater sign, among others). 3 Diagnosis can be made with a MRI scan and bony coalition can be confirmed with a CT scan, which can also be useful for preoperative planning. 2
After failing conservative management, operative intervention has generally been indicated in the presence of persistent symptoms, however, the optimal procedure has been a topic of debate. Earlier studies demonstrated success from primary arthrodesis, however, other literature has shown favourable results with coalition excision.4–7 Comfort and Johnson demonstrated that the size of the coalition was inversely correlated with patient outcomes. 8 For talocalcaneal coalitions, Wild et al. associated poor outcomes with greater than 50% involvement of the middle facet on preoperative CT. 7 More recent studies have suggested favourable results with excision of talocalcaneal coalitions with greater than 50% involvement of the posterior facet. 9 As a result, excision of talocalcaneal coalitions is typically the first operative intervention in paediatric patients, with arthrodesis being reserved as a salvage procedure.
Despite numerous operative methods having been previously described, intraoperative identification and complete subtalar coalition resection have remained challenging. Keith needles and flat instruments, in combination with fluoroscopy, can help delineate the location and extent of the coalition.4,5,10 Humbyrd and Myerson 11 published a technique utilizing a laterally inserted guide wire at the level of the sinus tarsi and subsequent use of a cannulated arthroereisis sizing guide to create a fracture through the medial facet coalition. Arthroscopically assisted or complete arthroscopic talocalcaneal coalition resections have also been described but have a steep learning curve, increased operative times and risk of iatrogenic injury to the posterior tibial neurovascular bundle.12–14
There is growing appreciation for the role of advanced imaging and computer-assisted surgery within orthopaedics. This may prove useful in the resection of talocalcaneal coalition resections. Kemppainen et al 15 retrospectively looked at 12 patients with an intraoperative CT scan to assess talocalcaneal coalition resection. They found that intraoperative CT scans altered the operative management in three of the 14 feet (21%) and on blinded review resulted in an ‘excellent’ resection for 57% as compared with 25% in the control group without an intraoperative CT scan. In a seven patient consecutive case series to evaluate a new operative technique, de Wouters et al 16 found that the use of 3D-printed patient-specific cutting guides resulted in easier and more reliable talocalcaneal coalition resection.
We propose a novel operative technique utilizing real-time operative navigation to assist in the localization and complete resection of talocalcaneal coalitions. While operative navigation is becoming more common within all of orthopaedics, to the best of our knowledge, there is no literature looking at coalition resections.
Clinical vignette
This patient is a ten-year-old female with left talocalcaneal coalition (Fig. 1) and hindfoot pain refractory to conservative management. The risks, benefits and alternatives to surgery were discussed and the patient and family elected to proceed with coalition resection.
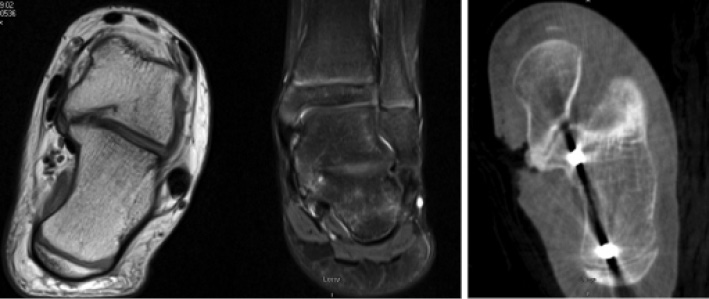
Preoperative MRI. T1 (left) and T2 (middle) imaging demonstrated the talocalcaneal coalition. The coalition appears mostly fibrous, however, as appreciated on the intra operative CT for navigation (right), the medial most aspect of the coalition is primarily osseous.
Operative technique
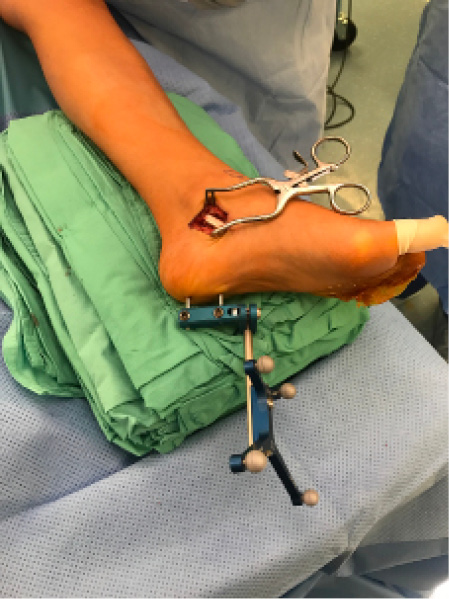
The patient was positioned supine with a bump under the hip of the nonoperative side, a thigh tourniquet and was protected with lead prior to standard sterile preparation. The lesser toes where wrapped in Iobanand (3M, Maplewood, Minnesota) and greater toe with the cut finger of a glove, to aid tendon identification, and a large bump was utilized for a working surface (Fig. 2). A straight operative approach was made down to the subtalar joint where the flexor digitorum longus tendon and flexor hallucis longus tendons where identified, confirmed by pulling and seeing the corresponding toes flex and retract (Fig. 3). Electrocautery was then used to expose the medial aspect of bone, presumably over the subtalar joint. The coalition could not be identified.

The patient was positioned with a blanket bump under the nonoperative hip and a large sterile bump was utilized as a working surface.

Exposure of talocalcaneal coalition. The flexor digitorum longus tendon and flexor hallucis longus tendons are retracted posteriorly in the left of the image. The coalition could not be identified.
Two 3.2 mm Kirschner-wires were placed into the calcaneus and the Medtronic Array (Memphis, Tennessee) was then fastened to this (Fig. 4). An intraoperative CT scan was performed with the Array in place (Fig. 5). Placement of the Array, intraoperative CT and imaging processing adds approximately five minutes to the surgery time. Following this, the location and trajectory of the coalition could be determined with the use of the operative navigation probe (Fig. 6). The coalition was removed with a small 4 mm burr. We intermittently checked location and trajectory with a navigation probe. The coalition was confirmed when the subtalar joint was cracked open with a lamina spreader. The subtalar joint capsule was then released with scissors posteriorly and medially; which greatly improved visualization and increased subtalar movement. Any remaining coalition was then removed with a burr and rongeur. With direct visualization and use of navigation complete coalition resection was assured (Fig. 7). The wound was irrigated and the bone was treated with bone wax. Subcutaneous tissue was closed with 2-0 Vicryl (Ethicon, Somerville, New Jersey) stitches. The skin was closed with 3-0 Monocryl (Ethicon, Somerville, New Jersey). Dermabond (Ethicon, Somerville, New Jersey) and Steri-Strips (3M, Maplewood, Minnesota) were applied followed by 0.25% bupivacaine hydrochloride. A 4 × 4 inch gauze and an elastic bandage wrap was applied. Patient could partially weight-bear for the first two weeks, while the incisions healed, and then transitioned to full weight-bearing as tolerated.
Two 3.2 mm Kirschner-wires were placed into the calcaneus to secure the Medtronic Array (Memphis, Tennessee).

An intraoperative CT scan was performed. Two sterile drapes were temporarily used to cover the operative field. Note, however, that the Array (white arrow) must be visible to the navigation camera during the CT scan.
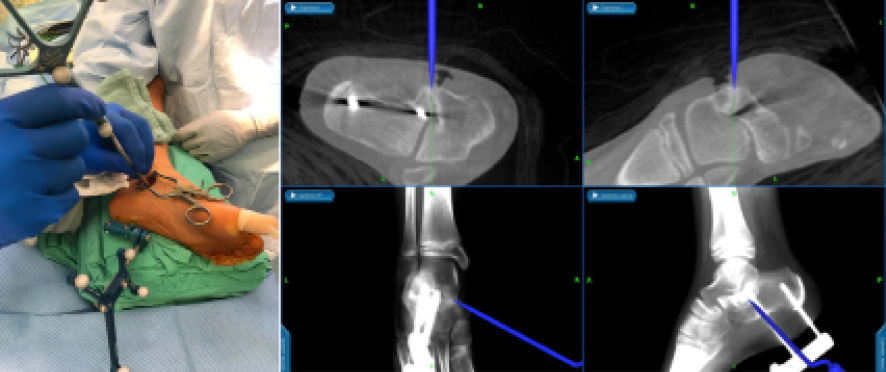
The navigation probe, held in the surgeon's hand, allows for real time localization and orientation of the probe tip on the axial, sagittal and coronal CT images.
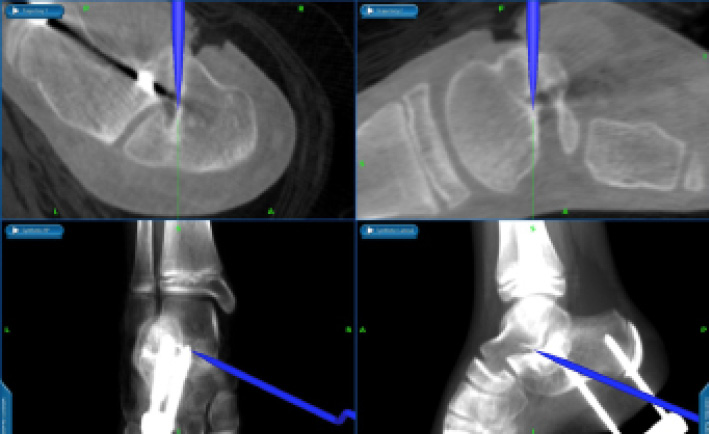
Using the navigation probe, it is possible to assess the extent and location of coalition resection intraoperatively.
Discussion
Identification and complete resection of tarsal coalitions can be quite challenging. With the use of CT-guided operative navigation in this patient, the coalition was immediately identified and its trajectory was easily followed. The live feedback of axial, coronal and sagittal CT imaging is intuitive. Kemppainen et al 15 posited that intraoperative CT scan should be considered to assess the completeness of challenging talocalcaneal collation resections. Although the use of operative navigation necessitates an intraoperative CT, it provides the benefit of real-time imaging from the point of coalition identification and continuously throughout the case. We used the navigation probe to confirm the location and orientation and followed with a high-speed burr, which was not registered to the navigation system. Some systems have a drill that is registered to the navigation system and can be used to document its location while removing the bone.
While de Wouters et al 16 found patient-specific cutting guides to aid in talocalcaneal coalition resection, this technique requires appropriate cutting guide fit on the bony surfaces and thus necessitates greater soft-tissue dissection and periosteal stripping. Additionally, once cuts are made or the bony landmarks are altered, the cutting guides are no longer accurate. Navigation allows for continued intraoperative coalition assessment and resection while respecting the unaffected anatomy.
Over-utilization of radiation studies, particularly in a young patient population, should be avoided. Fortunately, the foot is remote to the more radiation-sensitive organs resulting in a very low effective dose. The CT requires localizing fluoro (dose area product of 0.458 Gycm2) while the CT calculated effective dose was 0.012 mSv. 17 For perspective, the average adult has 3.1 mSv of background radiation from natural sources each year. 18 Thus the intraoperative CT scan equates to less than 1.5 days of naturally occurring radiation exposure.
Even with operative navigation, there are many nuances in the operative technique that aid in the coalition resection. The lamina spreader can crack through any small remaining coalition fragments, combined with release of the adjacent subtalar joint capsule, can greatly increase visualization and subtalar range of movement. These are both essential for intraoperative assessment of coalition resection.
In summary, computer-assisted surgery is quickly gaining popularity within orthopaedic surgery and its indications are growing. In the case of a complex subtalar coalition resection, this technique was both helpful and potentially timesaving by allowing immediate localization and guided resection of the coalition.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.