
Abstract
Purpose
Total hip arthroplasty (THA) is rarely recommended in skeletally immature patients. The goal of the present study was to report our short- to mid-term results of THA in a series of children aged 16 years or younger, including clinical outcomes and post-operative complications, signs of radiographic loosening of the prostheses, and revision rate.
Methods
The 18 children (two male and 16 female patients, 24 hips) underwent cementless THA at a mean age of 14.6 years (11 to 16). Five patients had a bilateral, one-stage surgical procedure. Clinical assessment of these hips used the Merle d'Aubigné et Postel scale modified by Charnley to facilitate assessment of the function of walking. Clinical and radiographic follow-up was conducted at six weeks, six months and then yearly for the first three years. All post-operative complications were recorded.
Results
No intra-operative or early post-operative complications occurred. At a mean follow-up of 3.8 years (1 to 8), all patients had greatly improved pain and function scores. All children in the present study improved from severely impaired gait, including four children who were wheelchair-bound, to completely unrestricted gait. All hips demonstrated good alignment with no evidence of wear or radiographic lucencies. No revision of components has been required. One patient had persistent adductor contracture which was addressed with adductor tendon release.
Conclusions
THA is a successful procedure for unsalvageable hip arthritis in children at a mean follow-up of 3.8 years. Long-term follow-up will be needed to determine implant longevity of the components in these children.
Introduction
Total hip arthroplasty (THA) is rarely recommended in children. Concerns about implanting prostheses in skeletally immature patients along with a myriad of technical difficulties including poor bone stock, severe bony deformities, leg length discrepancies, and small femoral canals usually preclude THA from being considered as an option. 1 In addition, surgeons are wary of the need to revise the prostheses as most paediatric patients will likely outlive their implants.2,3 Therefore, young patients with hip disease will often undergo various other surgical procedures which attempt to extend the survivorship of the paediatric hip and thus postpone THA. 4 Despite the advances in hip conserving techniques, there are still children in whom the hip disease progresses to disabling joint degeneration; and when all conservative measures have been exhausted THA becomes the only viable option allowing painless movement of the hip joint.
There is very little information available on THA in children to guide surgeons, patients and caregivers in making an informed decision in the treatment of end-stage joint disease of the paediatric hip. Much of the early literature on THA in younger patients has lost its use for current practitioners, since it primarily focused on the use of cemented prostheses in patients with rheumatoid arthritis.5–12
In more recent literature, the outcomes of contemporary cementless THA in young patients have been much more optimistic than those of cemented THA.13–15 However, most recent studies have focused on adolescents and young adults, with only a few that included patients under 16 years of age.16–22 The data from these children were grouped together for analysis with the older study subjects, with a higher proportion of THA performed in the older patients. Information on the outcome of the contemporary THA in the very young patient with end-stage hip disease is therefore missing.
The goal of the present study was to report our short- to mid-term results of THA in a series of children aged 16 years or younger, including clinical outcomes and post-operative complications, signs of radiographic loosening of the prostheses, and revision rate.
Materials and methods
Patient selection
Institutional Review Board approval was obtained before initiation of this retrospective study. The medical records of all patients that underwent THA at our institute performed by a single surgeon (L. Donnan), with maximum age of 16 years at the time of THA and minimum follow-up of one year, were reviewed.
Between November 2005 and May 2016, 24 THAs were performed in 18 patients (Table 1). In total, 16 patients were female and two were male. The age of the patients at the time of THA ranged from 11 to 16 years, with a mean age of 14.6 years.
Baseline demographic characteristics
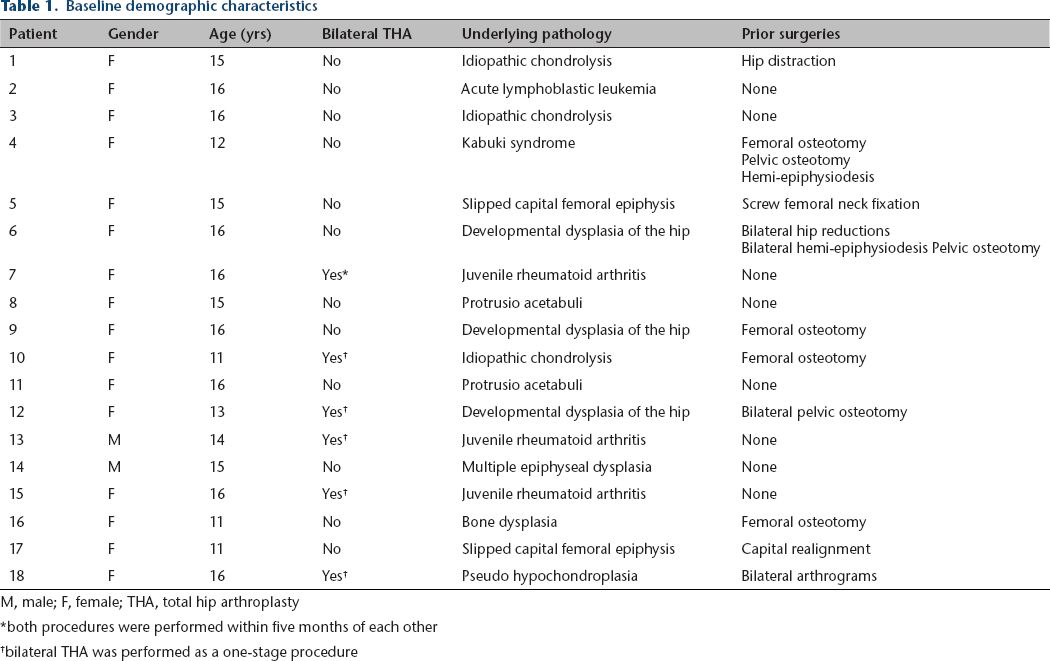
M, male; F, female; THA, total hip arthroplasty
both procedures were performed within five months of each other
bilateral THA was performed as a one-stage procedure
Surgical data
All patients received general anaesthesia during surgery. Intravenous cefazolin was given before incision and for 24 hours peri-operatively. A direct lateral approach with the patient in lateral decubitus position was used in all patients. Positioning of the acetabular component was challenging especially in those children with significant fixed flexion deformity of the hip causing extension of the hemi-pelvis. Acetabular components were positioned using the transverse acetabular ligament as reference but the orientation of the components was adjusted for initial stability, taking into account the reversal of the pelvic orientation to normal over time once the hip is mobile. A porous tantalum cementless acetabular component (Continuum Acetabular System; Zimmer Biomet, Warsaw, Indiana) was used in all patients. Acetabular components ranged from 42 mm to 64 mm. A cementless fully coated conical stem with longitudinal ribs for rotational stability (Wagner Cone Prosthesis; Zimmer Biomet) was used in 23 hips, and a cementless proximally porous-coated stem in one hip (VerSys Fiber Metal Taper Hip Prosthesis; Zimmer Biomet). Femoral stem sizes ranged from 12 to 22 mm. All components were inserted press fit and supplemental screw fixation of the acetabulum was used whenever appropriate. The bearing surface used was metal-on-polyethylene in all hips. Head sizes included 22 mm (two hips), 28 mm (21 hips) and 32 mm (one hip).
Outcome measures
The pre-operative and post-operative clinical assessment of these hips used the Merle d'Aubigné et Postel scale 23 modified by Charnley to facilitate assessment of the function of walking. 24 This scale considers pain, range of movement and ability to walk. Radiographic evaluation included digitally scaled pelvic radiographs as well as anteroposterior and lateral views of the involved hip. Clinical and radiographic follow-up was conducted at six weeks, six months and then yearly for the first three years. All post-operative complications were recorded. When patients turned 18-years-old, their care at our children's hospital was transferred to colleagues at a hospital with adult orthopaedic care. The Australian Orthopaedic Association National Joint Replacement Registry was consulted to confirm no revision surgeries were performed in those patients that were discharged from our follow-up.
Radiographs taken at the last follow-up were examined for radiolucent lines and osteolysis according to DeLee and Charnley zones. 25 Definitely loose components were defined as those that demonstrated a complete lucent line on any radiograph, femoral subsidence of 2 mm or more, or acetabular component migration or tilt compared with the radiographs obtained immediately post-operatively. 26 Possible loose components were defined as those with > 50% but < 100% lucent line on any radiograph or those with a progressive radiolucent line. 20 Femoral remodelling was assessed as a change in bone density, either as cortical or endosteal bone formation, with a decrease in bone density recorded as atrophy. 27 The radiographs taken at the last follow-up were further evaluated for bone defects using Paprosky's classifications 28 and for signs of eccentric polyethylene wear.
Statistical analysis
A paired Student t-test was used for the determination of statistically significant differences in the pre-operative and post-operative Merle d'Aubigné et Postel scale scores for pain, function, and ability to walk. A p-value < 0.05 was considered significant.
Results
Peri-operative difficulties and complications
Bone quality was fair to poor in 11 hips, necessitating bone graft in four hips (two hips with developmental dysplasia of the hip, two hips with juvenile rheumatoid arthritis). There were no intra-operative or early post-operative complications.
Clinical assessment
The mean duration of follow-up was 3.8 years (1 to 8). All patients had significantly decreased pre-operative scores for pain, hip function and ability to walk (Table 2). At the latest follow-up, all patients were pain free and were able to ambulate without any restrictions or crutches, perform outdoor activities (with one patient doing farm work, including climbing fences and lifting engine blocks) and attend school uneventfully. No patient required analgesics. Three hips had a slight Trendelenburg after THA, one of which was already present due to abductor damage at the time of prior pelvic osteotomy. Two hips had some paraesthesia in the distribution of the lateral femoral cutaneous nerve that was present pre-operatively. There were no complaints of leg length discrepancy.
Pre-operative and post-operative modified Merle d'Aubigné et Postel scores
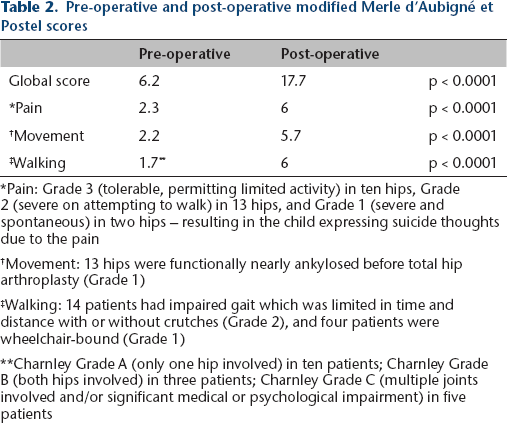
Pain: Grade 3 (tolerable, permitting limited activity) in ten hips, Grade 2 (severe on attempting to walk) in 13 hips, and Grade 1 (severe and spontaneous) in two hips - resulting in the child expressing suicide thoughts due to the pain
Movement: 13 hips were functionally nearly ankylosed before total hip arthroplasty (Grade 1)
Walking: 14 patients had impaired gait which was limited in time and distance with or without crutches (Grade 2), and four patients were wheelchair-bound (Grade 1)
Charnley Grade A (only one hip involved) in ten patients; Charnley Grade B (both hips involved) in three patients; Charnley Grade C (multiple joints involved and/or significant medical or psychological impairment) in five patients
One patient reported late post-operative problems with persistent adductor contracture that was addressed with adductor tendon release. One other patient reported a non-specific plaque over the incision site which did not require treatment.
Radiographic evaluation
All hip prostheses demonstrated good fixation and alignment with no evidence of radiographic lucencies, atrophy or bone defects at last follow-up. Gross polyethylene wear, indicated by eccentric position of the femoral head, was not present in any hips at this short- to mid-term follow-up.
Revision rate
At the latest follow-up, no revision of components was required or scheduled.
Discussion
The principal finding of the present study was that THA significantly improved the pain, range of movement and ability to walk in children 16 years of age and younger with unsalvageable arthritic hips. At a mean follow-up of 3.8 years (1 to 8), all hips demonstrated good alignment with no evidence of wear or radiographic lucencies, and no revision of components was required.
The substantial improvement in pain, function and mobility in all patients following THA in the present study is reminiscent of the early reports of THA in children with juvenile rheumatoid arthritis.5–11 Despite complications including dislocations and femoral fractures,9–11 excessive blood loss, 6 radiolucencies around the acetabular components in nearly 50% of prostheses at intermediate follow-up7,10 and failure rate up to 42% at long-term fol- low-up,9,29 the restoration of independent mobility and relief of pain in these patients during emotionally and cognitively formative years justified the recommendation of THA for many authors.6–8,10,11 In contrast to the earlier studies, no major complications occurred in the present study, except for one patient who reported with persistent adductor contracture which was addressed with adductor release. In addition, we did not encounter complaints of post-operative leg length discrepancy as predicted leg length discrepancy was taken into account in the arthroplasty. The hip pathology in the youngest patients was bilateral, with growth arrest of both proximal femurs at the time of THA. Further acetabular growth was arrested as the cementless acetabular component effectively produced an epiphysiodesis of the acetabulum.
In the present study, all components were fully integrated and did not show any evidence of wear at one- to eight-year follow-up. This finding is comparable with the reports on contemporary cementless THA in adolescents and young adults, which have shown stable implant fixation of femoral stems and acetabular components at intermediate follow-up.15,19,21–23
Since the long-term results are not yet known, we remain cautious when recommending THA in children. However, when faced with a child with disabling hip pain and progressive loss of independent mobility, the options are limited. The patients in the present study had exhausted all non-operative and hip preserving measures, as evidenced by the large numbers of surgeries preceding the THA (Figure 1). A total of 16 surgeries were performed in the 24 hips, including femoral osteotomies, pelvic osteotomies and hip distraction.
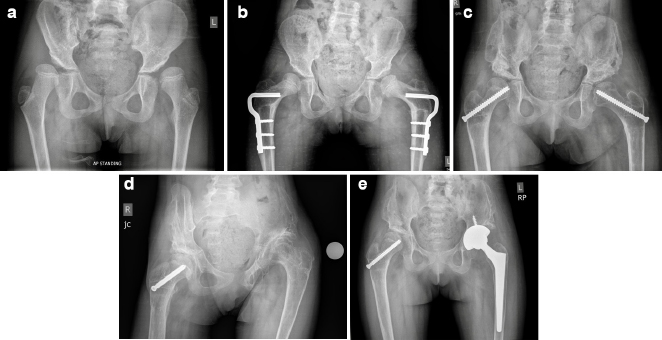
A series of pelvic radiographs of the same patient, illustrating the progression of hip pathology despite surgical attempts at preserving the hip: (
The most evident surgical alternatives that could be considered would be femoral head resection and arthrodesis of the hip. Among nonambulatory children with cerebral palsy and chronically painful, unreconstructable subluxated or dislocated hips, femoral head resection is certainly a viable solution with good pain relief and low risk of complications. 30 For the young labourer with noninflammatory, monoarticular hip arthritis, hip arthrodesis remains a valid option.31,32 In the present study, three patients had bilateral hip involvement and five patients had multiple joints involved and/or significant medical or psychological impairment - rendering hip arthrodesis unfeasible.33,34 For the remaining ten patients, hip arthrodesis could have been considered. However, in our own experience, the results of takedown arthrodesis have been markedly inferior to primary THA. This experience is consistent with the report by Richards and Duncan, 35 in which takedown arthrodesis patients experienced poor clinical outcomes and high complication rates compared with primary and even revision THA.
Longer follow-up is necessary before definite recommendations could be given regarding THA in this very young population. Furthermore, we are unable to comment on alternative implant materials such as ceramic. The bearing surface used in the present study was met- al-on-polyethylene in all hips as a predictable bearing surface with minimal chance of inducing teratogenic effects in a fertile population. We were concerned about using small or thin ceramic bearing surfaces in an active paediatric group who could potentially fracture the material. Nevertheless, we believe the present data on the short- to mid-term outcomes of THA is useful for the informed decision in the treatment of end-stage joint disease of the paediatric hip.
In conclusion, THA is a successful procedure for unsalvageable hip arthritis in children at a mean follow-up of 3.8 years. Clinical outcomes were greatly improved after THA in all children. All hips demonstrated good alignment with no evidence of wear or radiographic lucencies. No revision of components was required.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.