
Abstract
Purpose
Physiological range of tibiofemoral angle (TFA) is poorly defined and may lead to unnecessary therapeutic interventions. Studies on TFA developmental pattern suggest that racial and ethnic differences are present; children in north-east India who have not yet been studied need to be evaluated.
Patients and methods
Cross-sectional study of clinical TFA, intermalleolar distance and intercondylar distance in 1020 healthy north-east Indian children aged from 2 to 18 years was done. Height, weight and body mass index were also recorded.
Results
At two years of age the mean TFA was valgus. The values reached a peak of 8.55° (standard deviation (SD) 1.01) valgus at seven years of age. The TFA then gradually stabilised to 3.18° (SD 1.18) valgus by 18 years of age. There was no significant difference in TFA between male and female patients.
Discussion
The present study is the largest and only the third such study on Indian children and the first on healthy northeast Indian children. By the end of two years most children had valgus angulation. This, along with the peak angulation observed, was similar to most of the other studies. The age at peak angulation and subsequent stabilisation of valgus angulation varied greatly among children of different origins, especially non-Indian children.
Conclusions
Data can be used to identify children who require further follow-up/evaluation and can serve as guidelines during deformity correction and future studies. The development of TFA in this cohort is not different from other children of India but differs from children of other ethnic origins.
Keywords
Introduction
The tibiofemoral angle (TFA), or knee angle, is defined as the angle between the anatomical axis of femur with the anatomical axis of tibia. 1 The angle may also be expressed indirectly as intercondylar distance (ICD) and intermalleolar distance (IMD). 2 This alignment is subjected to the effects of genetic factors, intrauterine posturing, nutritional status, hormones, ligamentous laxity, anatomical peculiarities of femur and tibia which change with age, adaptive changes to weight-bearing and differential growth of the physis.3–10
Genu valgum and varum are commonly encountered paediatric orthopaedic problems, particularly after children begin to walk,1,11–13 and are a source of great apprehension among parents. These angular deformities may be physiological or pathological14,15 as during normal development the knee undergoes sequential physiological changes which leads to change in lower limb axial alignment from varus to valgus.1,2,11,16,17 However, such angular deformities may also develop on account of pathology at the epiphysis, the physis or the metaphysis This may in turn lead to abnormal loading of the joint and, if uncorrected, may predispose to painful knee, degenerative arthritis and joint instability.15,18
Several groups have studied the developmental pattern of knee angle on different paediatric populations. However, in spite of all the literature on the subject, misunderstandings regarding the physiological range of knee angles persist and often lead to unnecessary therapeutic interventions on the part of the surgeon such as bracing, corrective osteotomies and, more recently, physeal modulation, all of which may be unwarranted and in some cases may even prove harmful.1,11,17
The results from previous studies suggest that differences in the physiological range of TFA may arise with race and ethnicity, apart from age, gender, height, weight and body mass index (BMI).1,2,11,13,17,19–24 Hence, sound knowledge of the developmental pattern of knee angle in children of the specific population is necessary.
To our best knowledge, only two Indian studies have dealt with this subject on two ethnically different Indian sub-populations.1,11 However, there is no such literature describing the normal physiological development of knee angle in northeast Indian children who are ethnically different from the rest of the country. The present study is aimed at addressing this problem by studying the development of TFA in healthy north-east Indian children, comparing it with other populations and defining the normal range of TFA in this specific population.
Patients and methods
The study was conducted over a period of one year between July 2015 and June 2016. In this community-based cross-sectional study, a total of 1020 healthy children, with 60 in each age group, were included after obtaining informed consent from the parents or the school/day-care centre (Anganwadi) authorities. Permission was obtained from the Ethical Committee prior to the commencement of the study.
Calculation of sample size
The sample size was calculated using data from previous studies and applying appropriate statistical formula. Considering the mean TFA (± standard deviation (SD)) among males and females to be 4.61° ± 2.96 and 5.39° ± 2.45, respectively, 11 and α (alpha) as 0.05 and β (beta) as 90%, the minimum sample size for the present study was calculated to be 904. Sample size was equally divided into 17 age groups which deduces to around 53.17 per group. Rounding off to 60 children per group, the total sample size was determined to be 1020.
Study population
Children were selected from normal accompanying attendants of patients attending the outpatient department, vaccination clinics of the institution, day-care centres and schools in the city.
Study sample
After taking a detailed clinical history and performing a thorough general, systemic and local examination of the lower limbs, patients were selected according to the following criteria.
Inclusion criteria:
children aged 2 to 18 years with normal general, systemic and lower limb examination were included in the study.
Exclusion criteria:
children with skeletal (such as developmental dysplasia of hip, skeletal dysplasia, neuromuscular disorders, cerebral palsy, foot deformities) or extraskeletal/metabolic disorders which may affect the lower limbs were excluded from the study; children with family history of musculoskeletal disorders; any surgery of the lower limbs; leg length discrepancy > 2 cm; height and weight deviation > 2 SD from the age- and gender-matched norm; children outside the normal 5th to 85th percentile of body mass index (Centers for Disease Control and Prevention).
Methods
The age of the children was verified by examining documents of vaccination centres and school authorities. The chronological age of the children was rounded off to the nearest integer. Each participant was first examined clinically to exclude the presence of any pathology of the lower limbs or any other exclusion criteria. The children were specifically examined for the presence of short stature, gait abnormality, any rotational abnormalities (tibial torsion), ligamentous laxity, enlarged epiphysis and physis, relative lengthening of fibula compared with tibia, pes planus or in-toeing/out-toeing of feet which may point to a pathology.7,25,26 Children with signs of rickets and other suspect cases underwent radiographic and metabolic workup. If any abnormality was found, the participant was excluded from the study.
All measurements were taken by a single examiner (SK, junior author). The clinical TFA of the right lower limb was measured using a goniometer (Fig. 1) in a standing position. The children were made to stand with the hips and knees in full extension and neutral rotation and with the knees or ankles touching each other. The anterior superior iliac spine (ASIS) was marked with a skin marker pen. The centre of the patella was identified with the aid of concentric circles of increasing diameters and then marked with a pen. The midpoint of the ankle joint was identified using a Vernier calliper and marked with a pen. The occiput, buttocks and heels were all confirmed to be touching the wall before readings were taken (Fig. 2). The modified goniometer was then placed with its hinge at the centre of the patella. Each expandable arm of the goniometer was adjusted so that the tip of the proximal limb touched the ASIS and the tip of the distal limb touched the midpoint of the ankle (Fig. 3). 1 The TFA was then noted. The device could measure a minimum difference of 1°. All measurements were rounded off to the nearest degree. A valgus TFA was given a positive value, while a varus TFA was given a negative value. 1
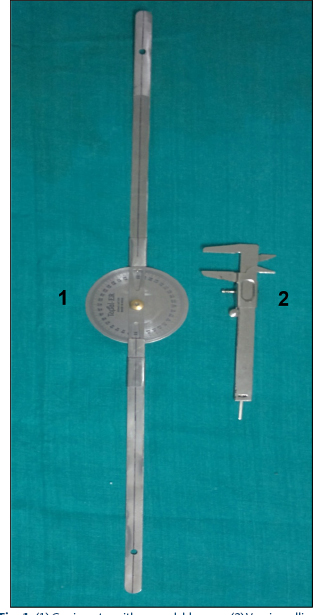
(1) Goniometer with expandable arms, (2) Vernier calliper.

Photograph showing position of child at the time of taking clinical measurements with the anterior superior iliac spine (ASIS), centre of patella and midpoint of ankle joint marked.

Measurement of the tibiofemoral angle (TFA) of the child using goniometer with expandable arms.
The ICD and IMD were also measured with a standard Vernier calliper which could measure a minimum difference of 0.1 mm. The IMD was measured as the distance between the medial malleoli with the medial femoral condyles in contact (Fig. 4). In cases where the IMD was 0, the ICD was measured as the distance between the medial femoral condyles with the medial malleoli touching.

Measurement of intermalleolar distance of the child using Vernier calliper with the femoral condyles touching each other.
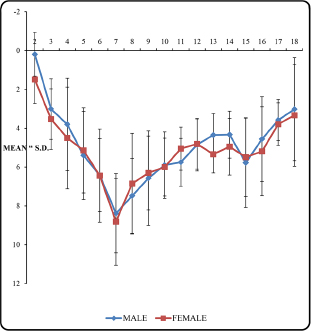
Mean TFA ± SD distribution among male and female children at different ages. Age in years.
Height was measured with the participant standing without shoes against a wall using a long measuring tape which could measure a minimum difference of 1 mm. Weight was recorded using a simple weighing scale which could measure a minimum difference of 0.1 kg. BMI was calculated using the formula weight/height 2 where weight is in kilograms and height is in metres. Limb length was measured as distance from the ASIS to the medial malleolus on both sides using a measuring tape.
The mean difference of TFA between males and females was assessed using Student's t-test. Correlation between TFA and age, height, weight, limb length, BMI and IMD was assessed with Pearson's correlation coefficient and significance assessed with Student's t-test. A p-value < 0.05 was considered significant. All calculations were done with Microsoft Excel version 2010 (Armonk, New York) and SPSS for Windows, version 21.0 (IBM, Chicago, Illinois).
To assess intra-observer variability, the TFA of any 20 children who were assessed on a single day underwent re-measurement a second time after six hours in a random order and the data were assessed.
Results
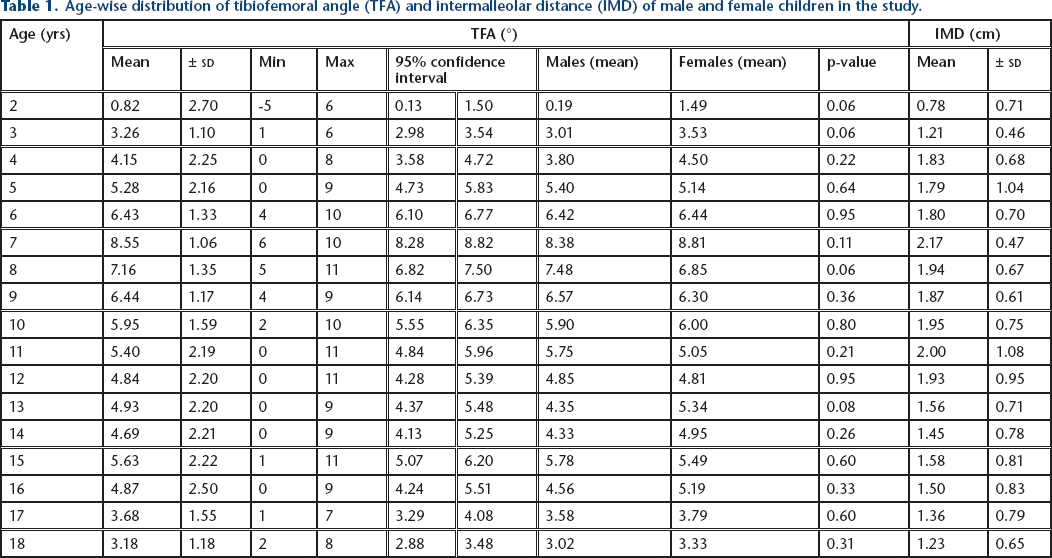
There were 516 (50.59%) male compared with 504 (49.41%) female patients in the study. Height, weight and BMI of each participant were found to be within the normal range for that age according to World Health Organization (WHO) and Indian growth charts. No limb length discrepancy was noted during examination of each participant in any age group. Table 1 and Figure 5 show that the - minimum mean TFA of 0.82° (sd 2.70) was seen at the age of two years whereas the maximum mean TFA of 8.55° (sd 1.06) was seen at the age of seven years. The minimum SD in TFA was 1.06° which was seen at seven years of age whereas the maximum SD in TFA was 2.70° which was seen at two years of age. The minimum individual TFA was 5° varus (taking varus as negative) which was seen at two years of age whereas the maximum individual TFA was 11° valgus which was seen at eight, 11, 12 and 15 years of age. There was no significant difference (p > 0.05) in TFA between males and females in any age group (Table 1). TFA showed significant but weak positive correlation with height, weight and limb length and significant moderate positive correlation with IMD. TFA also showed significant weak negative correlation with BMI.
Age-wise distribution of tibiofemoral angle (TFA) and intermalleolar distance (IMD) of male and female children in the study.
The graph plotted between the difference in angle measured (R1 - R2) and the mean angle ([R1 + R2]/2) measured by a single observer showed that most of the points lie between the -1° and +1° axes, indicating minimal intra-observer variation (Fig. 6).
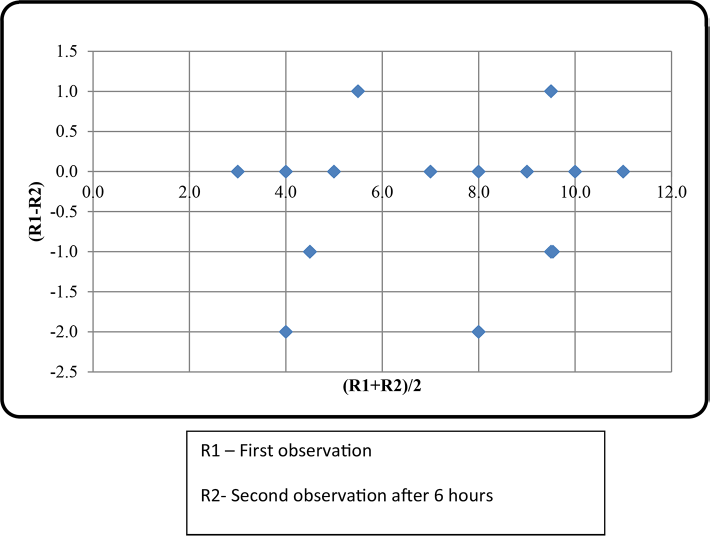
Determination of intra-observer variability.
Discussion
The knowledge of normal developmental pattern of knee angle/TFA in young growing children and its range of variation with respect to age, sex and race is important so that the surgeon is able to differentiate a physiological pattern from a pathological one (supplementary material). Based on these facts, parents may often need repeated reassurances. Knowledge about this angulation will help the surgeon to identify children who require close monitoring or further evaluation. It also provides the surgeon with normative data for deformity correction.
Knee angle abnormalities may also affect physical activity participation, postural control and bone density. Kaspiris et al 16 showed that valgus deformity negatively impacts physical activity participation which may affect bone density. Also genu varum deformity may increase postural sway, affecting balance control and increasing the risk of falling and injury during sports activities. 27
The radiographic method using full-length anteroposterior radiographs of both lower limbs used by Shopfner and Coin, 28 Salenius and Vankka, 19 Sabharwal et al 29 and Yoo et al 17 is an accurate method of determining TFA and also detects any associated bony abnormalities. 6 Accurate positioning and preventing malrotations of limbs are prerequisites for this method. However, subjecting normal children to radiation may not be ethical and was hence not preferred in this study.
A photographic method of determining TFA was used by Engel and Staheli 30 and later by Heath and Staheli, 31 by measuring the angle between the mid-longitudinal axis of the thigh and the tibia on a photograph of the patient with bony prominences that had already been marked. However, this method had potential sources of error, such as improper positioning of the camera which may cause improper profiling of limbs and errors during marking of axes and taking measurements. 6 It has been shown to be less accurate than clinical methods 6 and was hence not preferred for the present study.
The clinical method of measurement of TFA has been used by several researchers. The axis which has been drawn between fixed bony points instead of using imaginary lines reduces the probability of error. 1 The use of goniometers with expandable arms that reach up to the bony landmarks further reduced the chances of error. Moreover, this technique is cheap, easily performed and does not carry any radiation hazard. It has also been shown to correlate well with the anatomic TFA.19,32 The measurements in this study were assessed for intra-observer variation, which, even though was found to be minimal, may be responsible for the sizable sds noted in each age group and the change in TFA after skeletal maturity. The reliability of this method has also been established in previous studies.1,11,13,33 The ease, repeatability, reliability and validity of this measuring technique combined with standardisation of position of the patient during the clinical measurement procedure to minimise errors makes it ideal for use in clinical practice and was hence used in this study.
It has been well established from previous studies that children are born with a varus angulation of the knee which gradually decreases and attains a maximum valgus. This valgus angulation then decreases and becomes stabilised at a value which persists into adulthood as normal valgus alignment of knee. The age at which these changes occur, however, has been shown to vary with ethnicity. 11
The present study included children aged 2 to 18 years. In the two-year age group, it was seen that the majority of children had a valgus angulation with a mean of 0.82° ± 2.70. Varus angulation persisted in 15 of the 60 children in this group, with a maximum varus angulation of 5°. But by the end of three years, all children had valgus angulation with no varus persisting. This observation of disappearance of varus and appearance of valgus by the age of two to three years is similar to other studies and also to the only two other studies on Indian children (Mathew and Madhuri 1 and Saini et al 11 ) as seen in the supplementary material. Oginni et al 22 also concluded that varus knee alignment was uncommon after two years of age in Nigerian children and large knee angles between two and five years of age suggested rickets. Heath and Staheli 31 also concluded that the presence of varus between the ages of two to 12 years was abnormal. Thus, a varus alignment after the age of three years needs detailed evaluation.
The mean valgus angulation in the present study increased from 0.82° ± 2.70 at two years to reach a maximum of 8.55° ± 1.06 at seven years. The peak valgus angulation was 8.38° ± 1.11 in boys and 8.81° ± 0.96 in girls, both seen at seven years of age. These results were comparable with the peak valgus angulation seen in other studies. It ranged from 6.7° ± 1.3 (south Indian boys) 1 to 9.8° ± 1.4 (Turkish girls). 13 Kaspiris et al 34 also concluded that Greek children aged three to nine years exhibit < 8° physiologic valgus and a measurable angle higher than that should be considered abnormal and further evaluation should be deemed necessary. Salenius and Vankka 19 also concluded that there is a wide range of normal development of the knee angle which is physiological, so an operative procedure to correct the angle in normal children is seldom indicated.
The age at which peak valgus angulation was seen, however, differs greatly. The peak valgus angulation in the present study in boys and girls was seen at seven years of age. This was somewhat comparable with the two other studies on Indian children, Mathew and Madhuri 1 and Saini et al, 11 where it was seen at five to six years of age and also to Turkish children where it was seen at six to seven years age. 13 The peak however was seen earlier in other studies.
The valgus angulation after reaching a peak gradually decreased to reach a valgus angulation of 3.18° ± 1.18 (3.02° ± 1.13 in boys and 3.33° ± 1.23 in girls) at 18 years of age in the present study. In the two other studies on Indian children the angle stabilised to about 4° to 5° after ten years 11 and 3.18° ± 1.74 for boys and 4.43° ± 0.68 for girls at 17 to 18 years of age in south Indian children. 1 It was observed that with the exception of Indian and Turkish children this angulation stabilises earlier in most children of other origin.
The overall results of the present study are thus comparable with the two other studies on Indian children, by Saini et al 11 and Mathew et al, 1 and are somewhat comparable with results obtained by Arazi et al 13 on Turkish children. The differences observed between the present study and the other studies may be due to different methods employed to measure TFA, racial differences, the non-homogeneity of the study participants between different studies or observer-related factors.
Girls showed a higher mean tibiofemoral angulation across most of the age groups; however, the difference was not significant. Similar results were observed in Chinese, 20 Iranian, 35 Caucasian, 19 White 31 and Korean 17 children. Significant difference with respect to gender was seen in certain age groups in Turkish, 13 European, 21 Malaysian 33 and Saudi 24 children. This difference was more consistently seen in the adolescent age group.13,21 However, this aspect requires further research as studies by different researchers on similar populations have yielded different results, as seen in Indian and Nigerian children.22,32 Mathew and Madhuri 1 report significant differences at two to three years, 11 to 12 years and 17 to 18 years between males and females, which is contradicted by Saini et al 11 and the present study. Higher valgus angulation seen in adolescent females has been attributed to the shape of the female pelvis, wide angle between the pubic rami at the symphysis and larger pelvic outlet. 36
The TFA in the present study shows significant positive correlation with height, weight and limb length, but significant negative correlation with BMI. However, the degree of correlation is weak. Bafor et al 32 reported significant negative correlation between TFA and weight as well as TFA and BMI in Nigerian children. They concluded that axial loading, as represented by BMI, does not contribute to the increasing magnitude of knee angles in normal, healthy-weight children, but it may not necessarily be the case with overweight children. Kaspiris et al 16 also reported significant negative correlation of TFA with height and weight and non-significant negative correlation between TFA and BMI in Greek children. Arazi et al 13 found a fair degree of correlation between TFA and weight in Turkish children, whereas Cahujaz et al 21 found no correlation between weight and TFA in Caucasian children. Both, however, observed the largest IMDs in overweight children. Cahujaz et al 21 suggested that this could possibly be due to differences in soft-tissue thickness at the knees. Mathew and Madhuri 1 noted significant correlation of TFA with standing height and limb length although no correlation was seen with weight in their study on south Indian children. They observed that from the age of five years the TFA decreased with increase in standing height significantly. They attributed a significantly lower TFA in adolescent boys than girls due to their increased height. However Saini et al 11 did not note any significant correlation of TFA with height in Indian children. Hence, further research may be required to clearly accept or refute these associations.
Moderate significant correlation was found between TFA and IMD in the present study. The IMD followed a somewhat similar trend to TFA with respect to age (Table1). Our results were somewhat similar to observations made by Mathew and Madhuri 1 who reported a maximum IMD of 3.3 cm in the five- to six-year age group and a significant positive correlation between TFA and IMD in south Indian children. Saini et al 11 also noted a fair degree of positive correlation between TFA and IMD. They observed the highest mean IMD of 4.5 cm in children aged five years, with a minimum mean of 1 cm at the age of nine years, which apart from the highest mean values follows the trend seen in the present study.
Cheng et al 20 noted that ICD/IMD measurement was easier to apply clinically and was as reliable as TFA measurement. This was, however, contradicted by Cahujaz et al, 21 who although found significant correlation between these two measurements but concluded that TFA measurement was more accurate as SD of IMD was more than the mean. Arazi et al 13 suggested that the TFA measurement was easier and more reliable than distance measurement. In spite of their data showing a fair correlation coefficient between the TFA and distance measurement, they suggested the need for further investigations for the evaluation of reliability of distance measurement as they observed some difficulties in the positioning of the participants when the distance measurement was performed. A similar conclusion was made by Mathew and Madhuri. 1
One of the limitations of the present study was the cross-sectional nature of the study. A cohort study would have been more meaningful and reliable to assess the developmental pattern and degree to which spontaneous correction of knee alignment takes place with age, but that would have required repeated examinations of the same cohort of children over a much longer period of time. A second limitation of the study was the wide range of data and the large SDs encountered in the results obtained, which prevent the establishment of a ‘normal cut-off’ value for different age groups. Only the general trend in knee angle changes with age were detected by the study. The determination as to whether a specific limb is malaligned or not and requires some sort of therapeutic intervention is difficult.11,17 However, the present study, to our best knowledge, being the largest and only the third such study on Indian children and the first one in north-east India, does provide us with vital information regarding development of knee angle in children, especially for this ethnic population. Further radiographic and biochemical evaluation along with regular follow-up should be carried out in children whose TFA vary markedly when compared with the range/SD described for each age in the present study.1,11,37 Also, the values obtained for TFA at various ages for the population under study can serve as a practical and accurate reference for future studies. Third, the population under study might not be the true representative sample of north-east Indian children and only a randomised multi-centric study from all parts of the region involving children belonging to all ethnic subgroups can exactly predict the normal development of the knee angle in healthy children of north-east India. Fourth, since the study was a clinical one, observer bias may be an issue. Though we attained minimal intra-observer variation and excluded suspect cases with any lower limb anomalies, bias cannot be completely ruled out. Finally, we could not study children aged under two years as it was difficult to hold them in position for the duration of examination.
The measurement of TFA by clinical methods using a goniometer is a practical, reliable and valid method of assessing knee alignment abnormalities in children when standard positioning methods are followed while taking measurements. The study showed that no varus angulation persists in healthy children beyond three years of age and the reversal of physiological varus in most children occurred by the age of two years. The TFA then increased rapidly to reach peak valgus angulation of 8.55° ± 1.06, which was seen at seven years of age. Thereafter, a gradual decline in TFA to 3.18° ± 1.18 valgus by 18 years of age occurred. The study reaffirms racial differences; however, there was no significant difference in TFA with respect to gender. Even though there are limitations in the present study, the study gives us the mean TFA at each age along with SD and 95% confidence interval data for healthy children of north-east India which was yet unknown. These data can be used to identify children who require further follow-up and evaluation and can also be used as guidelines during deformity correction surgeries in this population.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
No funding was received for this study.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent was obtained from all individual participants included in the study.