
Abstract
New pathophysiological insights
Based on improved knowledge of the vascular supply of the proximal femur, a safe surgical dislocation of the hip joint was established allowing direct insights to the pathomorphological malfunctioning of the joint. One insight was that slipped capital femoral epiphysis (SCFE) impingement leads to substantial damage of the chondrolabral rim area, even in the presence of minor slips. A further surgical development was the extended retinacular flap allowing for correction of the deformity with calculable risk for iatrogenic necrosis.
Consecutive surgical concept
In 20 years of experience, a treatment concept for SCFE could be established which replaces classic pinning in situ and indirect correction of the deformity with subcapital re-alignment when the physis is still open, with true femoral neck osteotomy for hips with closed physis. Pinning in situ still has a place in minor slips but should be combined with open or arthroscopic recreation of an anterior metaphyseal waisting.
Unexpected complication
Loss of joint stability is a rare complication of anatomic re-alignment. It can be disease-related when the impingement has induced severe destruction of acetabular cartilage. It can be related to the surgical procedure, especially when the neck was excessively shortened and refixation of the trochanter was not advanced. Finally, in cases with severe and long-lasting deformity, the acetabulum may undergo adaptive flattening, being the cause of joint destabilisation with the correction of the deformity. Advancement of the greater trochanter and/or peri-acetabular osteotomy may be discussed to restabilise the joint.
Introduction
Very early in the evolution of the impingement concept, 1 slipped capital femoral epiphysis (SCFE) was recognised as a prototype showing both inclusive and impacting impingement depending on the degree of the slip. 2 Safe surgical hip dislocation 3 allowed the visualisation of the pathomechanical process producing cartilage and labral damage even in mild slips. 2 Trial impingement on the open joint makes clear that the damage pattern is not only deformity-dependent, but the velocity of the motion (impact) is equally important. It also discloses that increased motion due to remodelling is not a preferable advancement but rather changes the impingement mode from impaction to inclusion, which is more deleterious for the joint cartilage. Such findings put another complexity on reports about good results achieved with the pinning in situ technique4,5 and are supported by more recent reports with similar findings 6 and less favourable outcomes of pinning in situ. 7 The conclusive pathomorphological findings imposed a change of treatment concept towards a newly developed extended retinacular flap approach as the centre piece.2,8,9 Meanwhile this approach has been adopted by several surgeons.10–15 The overall concept includes pinning in situ, subcapital re-alignment, correction at the level of the neck and acetabular re-orientation in cases with joint instability after anatomic slip correction. In this overview, typical examples of indication, description of surgical execution and results are presented.
Pinning in situ combined with arthroscopic anterior osteoplasty
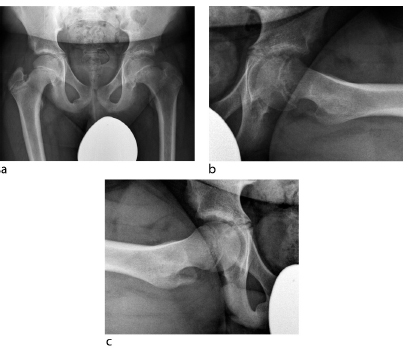
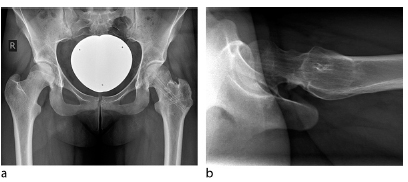
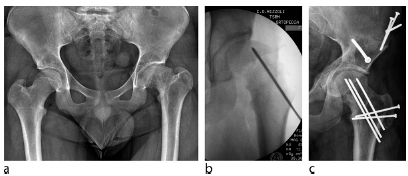
SCFE with slip angles of 30° or less may not be detected with anteroposterior (AP) radiographs and may need a lateral view (Fig. 1). However, internal rotation in flexion is limited and when forcefully executed it is painful. Pinning in situ remains a valuable treatment for such hips. However, if executed as an isolated procedure, even very minor slips may lead to femoroacetabular impingement (FAI) to become eventually symptomatic at a later stage.16,17 Therefore, it should be combined with an anterior osteoplasty to recreate a normal head-neck waisting (Fig. 2). The osteoplasty, which can be performed arthroscopically, or an anterior capsulotomy should lead to internal rotation with flexion of 20° or more without impingement between the acetabular rim and the anterior neck. The scarce literature shows good short-term to mid-term results.18,19
(
(
Moreover, one should pay attention to hips with anterior overcoverage due to retroversion of the acetabulum, a morphological finding which seems to be not rare in SCFE hips. 20 Under such circumstances, even a decent osteoplasty may not be sufficient and the level of impingement may just shift more distally; therefore such hips may be better treated with subcapital re-alignment. Leg shortening, even in these mild SCFEs, cannot be compensated by the above procedure and the patients have to be informed about mild but persisting shortening (Figs 3 and 4).
Five-year follow-up: (

Same case as in figures 1, 2 and 3. Bilateral standing long-leg orthoradiographs demonstrate a shortening of the left femoral neck due to premature closure of the physis and slip of the epiphysis on the left side. A bilateral valgus deformity of the tibia was treated with temporary hemiepiphyseodesis.
With SCFE angles greater than 30°, the epiphysis insufficiently corresponds with the anterosuperior acetabulum under axial loading, a mechanical situation which may be similar to an anterior insufficiency of coverage. We therefore do not recommend using this combined technique in slips greater than 30°.
Subcapital re-alignment for stable SCFE
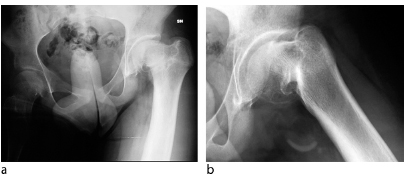
The majority of moderate and severe stable SCFE have a slip angle in the range of 30° to 60° (Fig. 5). In addition, they show a substantial posterior shift of the epiphysis against the metaphysis; the pathophysiological consequence is a bone apposition at the posterosuperior margin of the metaphysis. Range of motion (ROM), and internal rotation in particular, is limited and painful. When the subcapital deformity is corrected at the inter-/subtrochanteric level, e.g. with an Imhäuser-type osteotomy, AP radiography may appear satisfactory, however FAI is not addressed sufficiently, an aspect which was not considered in the recent literature. 21 Provided the growth plate is still open, subcapital re-alignment is the best way for anatomic reconstruction of the proximal femur.
(
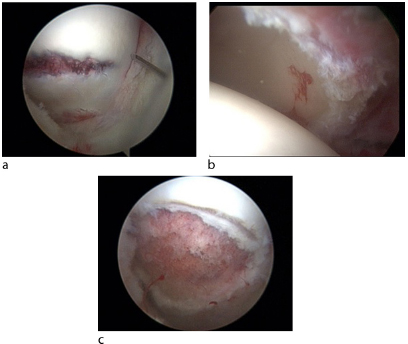
The first step is the surgical hip dislocation approach. 3 In brief, the patient is in a lateral position with a mobile extremity (Fig. 6a). After a longitudinal incision centred over the greater trochanter, the fascia lata is divided anterior to the gluteus maximus muscle. The greater trochanter is osteotomied and flipped anteriorly together with the attached gluteus medius and vastus lateralis muscles. This is generally more difficult in SCFE, as internal rotation is limited due to the slip and care must be taken to avoid unintended large anterior trochanteric osteotomy. To avoid injury to the deep branch of the medial femoral circumflex artery and its anastomoses with the superior and inferior gluteal artery, the joint capsule is dissected between the piriformis and gluteus minimus muscles. After a Z-shaped capsulotomy, the joint is inspected for free blood and eventual epi-metaphyseal instability. In doubt of physeal stability, two K-wires secure a stable connection. Before dislocation, the epiphyseal perfusion is to be tested using a simple drill hole to see brisk bleeding or to use laser Doppler flowmetry or a probe for measuring intracranial pressure. With external rotation of the femur, the joint is dislocated; in severe slips, dislocation may become possible only after piecemeal resection of the stable part of the greater trochanter (see below). With dislocated hip, the integrity of the retinaculum is checked and the damage pattern of labrum and adjacent cartilager is documented.
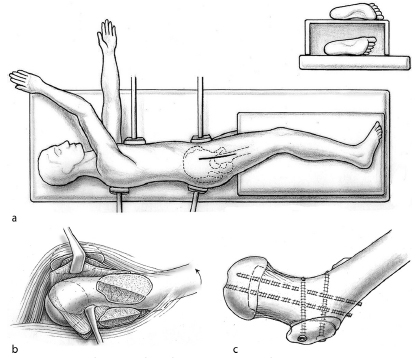
For the modified Dunn procedure, (
The preparation of the retinacular flap has to be done strictly subperiosteally and an essential element is the piecemeal resection of the stable portion of the greater trochanter. Occasionally, one can mobilise the entire fragment through the scattered physis. Further subperiosteal mobilisation follows a co-axial incision of the neck periosteum just anterior to the retinacular fold and a periosteal incision anterior to the gluteus maximus tendon, both allowing presentation of the posterior neck from the head-neck junction down to the lesser trochanter (Fig. 6b). Care must be taken that the flap is not detached from the epiphysis. The medial periosteum, including Weitbrecht's ligament and the medial branch of the medial femoral circumflex artery, is dissected in a similar way; in contrast to the lateral flap, the dissection is easier with the femoral head dislocated. The dissection of both flaps is completed when a curved instrument can go around the posterior neck from medial and lateral dissection.
Before disengagement of the epiphysis, a swab is positioned in the acetabulum to avoid inadvertent reduction of the mobile epiphysis. With a curved osteotome, the physis is opened first at the anterior aspect. Disengagement is easier after the medial portion of the posterior metaphyseal bone is resected in an external rotation-flexion position of the femur. A careful external rotation manoeuvre in extension allows to push the mobile epiphysis more posteriorly and to inspect the entire metaphyseal stump. The bone apposition on the posterior neck can be palpated easily and must be resected evenly to the surface of the original surface. Residual tissue of the growth plate is debrided from the neck and epiphysis, together accounting for a shortening of about 5 mm. Thereafter, some bleeding from the epiphyseal bone may be observed; however, a spasm of the retinacular vessels not infrequently leads to a delay. Manual reposition of the epiphysis takes into consideration a circumferential offset. Retinacular tension must be under constant control while the reposition manoeuvre must be easygoing. Forceful reposition has to be avoided; nevertheless, additional shortening of the neck is rarely necessary when the retinacular flap is prepared down to the lesser trochanter. The first fixation is with a retrograde fully threaded Kirschner wire. After fluoroscopic control of optimal epiphyseal position and joint congruency, two more antegrade wires are inserted. Capsular closure should not be tight and refixation of the greater trochanter should be executed with slight distal advancement (Fig. 6c).
In the rare valgus slip, the surgical steps are basically identical. However, it is wise to take some more bone from the anteromedial metaphyseal surface to avoid inadvertent tension of the retinaculum during reposition of the epiphysis into a more varus-/flexion-free correction of the valgus-/retro-tilt of the head in a more varus/flexion position.
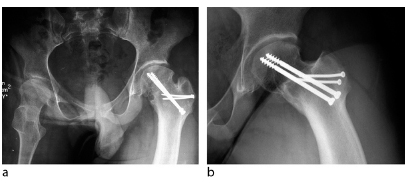
In 86 chronic slips treated with subcapital realignment as described above, 89% had acetabular cartilage damage from superficial to full thickness destruction at the time of open surgery; interestingly, there was no association with higher slip angle or chronicity. 22 With a follow-up of one to 15 years, there was no necrosis of the epiphysis 22 and no other major complication (Fig. 7); two hips showed delayed union of the trochanteric osteotomy.
Five-year follow-up: (
Subcapital re-alignment for disconnected epiphysis
Clinical classification systems of SCFE use the terms ‘acute’ or ‘unstable’ to indicate mechanical disconnection of the epiphysis, a condition which is associated with a high risk of avascular necrosis. However, verification with open surgery revealed false-positive and false-negative correlations, indicating the need for additional imaging techniques such as ultrasound or MRI. 23 Intra-operative findings in 33 hips with disconnected epiphysis showed less severe cartilage damage than in stable slips, a phenomenon which may have to do with a shorter and faster course of the slipping process. 22 Today, suspected or proven epiphyseal disconnection is an indication for urgent surgery. Previous attempts could not prove that the time factor from incident to surgery influences the rate of necrosis 24 because it was hidden behind closed reduction and also the fixation was performed as a closed procedure. Actual intra-operative observation of the vascular pathophysiology at the mechanically unstable epiphysis and of the phenomenon of intra-operative reperfusion immediately after re-alignment support this concept. 22 The evidence that bone apposition at the posterior neck can be demonstrated even in hips without clinical prodromes allows the speculation that a silent early phase of slippage is more regular than the exception: only in two of the group of 35 hips was posterior callus reported to be absent, while for three hips no information is given. 22 As a consequence, one should refrain from attempts to reduce the epiphysis before callus resection at the posterior neck, be it closed or open, be it gentle or forceful. In the mentioned series of 35 slips with disconnected epiphysis, six hips showed no signs of perfusion at capsulotomy, but perfusion returned with re-alignement. Four hips had no perfusion at capsulotomy and after re-alignment although the retinaculum was intact; one of these showed perfusion at the occasion of refixation for broken wires six weeks after the initial surgery. 25 Three hips went on to necrosis, one showing complete avulsion of the retinaculum at capsulotomy; the other two had a delay of surgery of more than one week.
Re-alignment of slips with closed physis
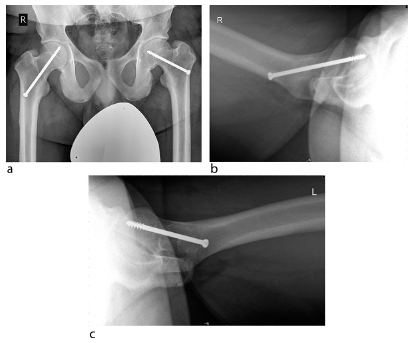
It is rather infrequent that slips have to be corrected when the growth plate is closed (Fig. 8). Under such conditions, subcapital re-alignment is difficult and is associated with a higher risk of detaching the retinacular connection with the epiphysis; on the other hand, subperiosteal presentation of the mediocervical bone is rather easy. The amount of the anterolaterally based wedge resection should be executed in a way to allow maximal cortical contact of the fragments. Fixation at this level is best with two (or even three) 4.5 mm cortical lag screws (Fig. 9).
(
Four-year follow-up: (
Care must be taken to avoid undesired rotation of the head fragment during insertion of the screws. Refixation of the greater trochanter should be more distal and take into consideration that the neck after such osteotomy is shorter. The healing time of a neck osteotomy takes about three months compared with two months at the subcapital level.
Joint instability after anatomic re-alignment: The role of the acetabulum
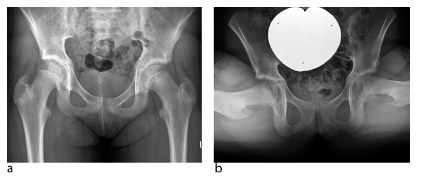
With increasing experience using anatomic re-alignment techniques, anterolateral migration, instability and even dislocation of the reduced femoral head have been occasionally observed. For two reported cases, chondrolabral damage, transsection of the round ligament, large capsulotomy and loosely resutured capsule were speculated as causative interaction. 26 A further reason for joint instability could be excessive shortening of the neck, leading to a loss of joint coherence and/or trochanteric impingement if distal avancement has not been added. It has been observed that a large area of acetabular cartilage destruction has led to femoral head migration into the cartilage defect. 2 Acetabular retroversion was found to be frequently associated with SCFE; 27 however, it was more discussed as a possible co-factor for the origin of SCFE and does not seem to be responsible for the instability of the joint. Pre-existing acetabular dysplasia has not been described in the context of classic SCFE, but seems to exist as a mild form in the rare valgus slip. So far, varus correction of the caput valgum seems to sufficiently compensate for this deformity. More recently, secondary flattening of the acetabular roof has been observed in severe slips (Fig. 10) with early onset and long duration. 28 The deformity may be understood as adaptive to the femoral deformation, similar to the secondary aetabular dysplasia in Perthes disease, 29 although much less appreciated. In two such cases, anatomic re-alignment of the slip led to intra-operative joint instability and full dislocation as anticipated from the pre-operative radiologies. The instability was successfully eliminated by an immediate peri-acetabular osteotomy. 28 In the future we may also add joint-stabilising peri-acetabular osteotomy in slips with severe acetabular cartilage damage and head migration, as seen occasionally. 2
(
Subcapital re-alignment is the centerpiece of a treatment concept for SCFE and as such is gaining increasing acceptance. The technical execution is demanding, but appreciable. The best way to become acquainted is with a fellowship in an institution with a reasonable case load. With careful execution of the hip dislocation approach and of a sufficiently long extended retinacular flap, the risk of surgically induced epiphyseal necrosis is calculable; nevertheless, rigorous observation and documentation of pathological salience, especially with regard to the epiphyseal perfusion, is of outmost importance for the correct assessment of complications and results.
Arthroscopic osteochondroplasty is a possibility for SCFE hips with a slip angle of 30° or less. When the physis is still open, pinning in situ has to be executed as the first step. The incidence of such hips, however, is less than 10%. The morbidity of subcapital re-alignment for stable slips is small and no epiphyseal necrosis was observed in this group. The three definitive necroses in the group with disconnected epiphysis could be explained by reasons other than the surgical procedure. Additional acetabular re-orientation is a possible way to treat joint instability after epiphyseal re-alignment, a complication which may be seen in SCFE hips with severe acetabular cartilage damage. It was successfully executed in severe and long-lasting slips where adaptive flattening of the roof has allowed the re-aligned head to become unstable.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
No funding has been received for this submission.
Ethical approval: This article does not contain any studies with human participants or animals performed by any of the authors.
ML is a consultant to DePuy and Smith&Nephew., RG has stock options of Examedical S.p.A LT has no conflict of interest. HM reports he is a consultant of Smith & Nephew.