
Abstract
Background
Theoretically, dynamic thoracic compliance (DTC) should be reduced by vertical expandable prosthetic titanium ribs (VEPTR) since titanium rods, scar tissue and ossifications increase stiffness of the rib cage. The effect of VEPTR on thoracic compliance has not yet been elucidated. The impact of VEPTR on the development of sagittal balance has not been fully investigated.
Patients and Methods
In a retrospective study, we investigated 21 consecutive children who were treated by VEPTR from 2004 to 2011 and three control groups. We compared the development of thoracic compliance during growth to Nr1. Development of sagittal balance during growth was compared to Nr2 and to Nr3 (which has been instrumented from ileum to rib). Mean follow-up was 60.67 months (standard error of the mean (SE 4.77).
Results
The difference of change of DTC during growth of VEPTR group versus a control group was not significant (p < 0.05). However, initial DTC and DTC at last follow-up of VEPTR group were lower than DTC of the control group. The difference was significant (p < 0.05). Mean correction of Cobb angle after the first operation was 16.41° (SE 3.01). Until last follow-up, we saw a loss of correction of 8.23° (SE 3.22). The differences between the development of parameters of sagittal balance during growth between the VEPTR group, control group 2 and control group 3 were not significant (p > 0.05).
Conclusions
VEPTR treatment should start as early as possible since VEPTR seems to lead to an increased rate of DTC that is similar to healthy controls. Sagittal balance showed a similar development as in healthy children.
Introduction
Early onset scoliosis (EOS) bears the risk of rapid progression and may lead to thoracic insufficiency syndrome (TIS) if left untreated. 1 TIS is defined as the inability of the thorax to support normal respiration and/or lung growth and is diagnosed by clinical signs of respiratory insufficiency and loss of chest wall mobility. 2
The correction of spinal deformity by vertical expandable prosthetic titanium ribs (VEPTR) and the impact of VEPTR on thoracic volume, space available for lung (SAL) and forced vital capacity (FVC) are positive and documented in several reports.3–6
What has not yet been elucidated is the effect of VEPTR on thoracic compliance: VEPTR implantation causes thoracic scar tissue, the longitudinally implanted titanium rods produce additional stiffness of the thoracic wall and unintended bone fusions of the ribs.7,8 These constrictive mechanisms on the thoracic mobility may reduce thoracic compliance which forces infants to use more energy for respiration.
VEPTR was primarily applied with thoracostomy in patients with thoracic malformation that induced scoliosis.3,4 With VEPTR instrumentation osteotomies of rib synostosis were performed and thoracic compliance theoretically improved because the bony elements of the thorax became less rigid. Implantation of stiffening VEPTR may dilute or even counter that effect. It is reported that thoracic volume was increased acutely (Fig. 1). 4 The effect on thoracic compliance is not reported.
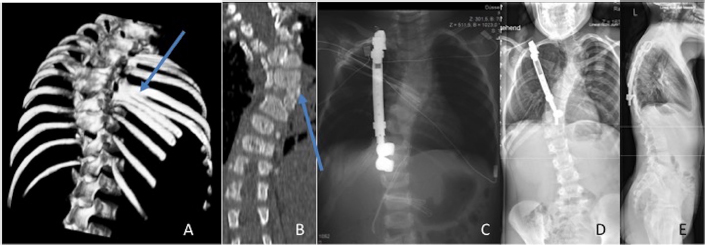
A female child with congenital scoliosis combined with rib synostosis. Treatment with vertical expandable prosthetic titanium ribs (VEPTR) was started at the age of 2.5 years. The child was not enrolled in the study. (
Since the growing rod technique 9 (instrumentation spine to spine, ileum to spine) may cause spontaneous spinal fusion. Also, the use of VEPTR in patients without thoracic induced scoliosis 10 by instrumentation from rib to rib, ileum to rib or spine to rib (Fig. 2) was established because it was thought to avoid spinal fusion. Recent reports contradict this theory by stating that VEPTR regularly causes spontaneous spinal fusion. 8
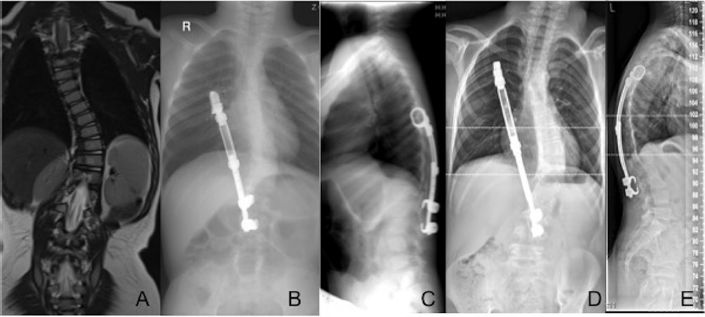
A male child with idiopathic EOS. Treatment with vertical expandable prosthetic titanium ribs (VEPTR) was started at the age of 3.5 years. (
Thus, the theoretical advantage of avoiding spontaneous spinal fusion by correcting spinal deformity with VEPTR instrumentation, rather than with growing rods, is in doubt. 8
A disadvantage of VEPTR instrumentation may be the impact on thoracic compliance. To investigate the effect of an intervention, it has to be compared to natural history.
The aim of our study was to investigate the impact of scoliosis on thoracic compliance and also to analyse the quality of deformity correction in the coronial plane and the impact of VEPTR on sagittal balance (sagittal plane) since this procedure is applied by a growing number of institutions.
Patients and Methods
In a retrospective study, 21 consecutive children (treatment group) who were treated by VEPTR technology between January 2004 and July 2011 were analysed. The mean age at initial surgery was 5.26 years (standard error (SE) 0.68).
Our inclusion criteria were children aged one to ten years with a rib–vertebra angle difference ≥ 20°, 1 a Cobb angle ≥ 40° or a progression of the Cobb angle of ≥ 5° in six months. We excluded patients with pre-operative rib synostosis. After initial surgery, these patients had elongation procedures every six months. Follow-up was 60.67 months (SE 4.77).
Data for analysis were clinical characteristics, complications, initial Cobb angle and Cobb angle before and after surgery for elongation, weight before each surgical procedure and dynamic thoracic compliance (DTC) directly before each surgical procedure, ten minutes after orotracheal intubation in supine position and always with the same respirator (Primus Draeger). We did not use muscle relaxation for our patients.
Compliance
We measured the dynamic total compliance, not the static compliance. Dynamic total compliance is the combined compliance for the lung and chest wall (C total dyn = dV/ dP). Since Sharp et al 11 and Zapletal, Paul and Samanek 12 found that the change of compliance in lung development is dependent on weight and age, compliance was standardised in relation to weight in kilograms. The difference between initial and last compliance in mL/mbar was related to the difference between initial and last weight in kilograms.
A control group of 16 consecutive patients who had more than two operations for other reasons (non-spinal, non-chest) were analysed.
Age, diagnosis and compliance before each surgery (ten min after orotracheal intubation in the supine position and always with the same respirator as in the scoliosis group) were recorded. Diagnoses that led to first operation were clubfoot (six patients), hip dislocation (four patients), cartilaginous exostosis (two patients) and slipped capital femoral epiphysis (four patients).
The mean age of the control group was 5.3 years (SE 0.94). We performed a mean of 3.4 (SE 0.42) operations in these patients. The mean follow-up was 55.4 months (SE 7.0).
We excluded patients with neurologic or anatomic impairment of pulmonary function.
Sagittal balance
We compared the change of sagittal balance to a control group of five patients that received more than one standard radiograph of the spine and in whom spine and hip disease were excluded. Reasons for the radiograph were blunt traumata. The mean age of the control group was 6.1 years (SE 2.3). The mean follow-up was 32.4 months (SE 14.2).
For additional analysis of any effect of ala hooks (ilium to rib) on sagittal balance compared with spine to rib instrumentation, we also measured a control group of eight patients who received an instrumentation from ileum to rib (the VEPTR group did not include any patients with ala hooks). The mean age at initial surgery was 8.78 years (SE 0.91).
Statistical methods
Statistical analysis was performed with SPSS 22 (IBM). Kolmogorov–Smirnov test was performed and showed normal distribution for compliance, Cobb angle, weight and parameters of sagittal balance. An ANOVA was performed for parameters of sagittal balance; Student's t-test for unrelated variables was performed for the other parameters. Results were regarded as statistically significant if p < 0.05. Descriptive data are given as mean and standard error of the mean (SE).
Results
Thoracic compliance
In a one-sided t-test, the difference between the initial compliance of the VEPTR group versus the control group and the difference of the compliance at last follow-up (LFU) of the VEPTR group versus the control group was significant (p < 0.05).
Initial and last measured compliance of the VEPTR group was lower compared with the initial and last measured compliance of the control group (Table 1).
Thoracic dynamic compliance

VEPTR, vertical expandable prosthetic titanium ribs; SE, standard error
The difference of the change of the compliance in relation to weight gain during growth in the VEPTR group versus the control group was not significant (p > 0.05).
The result is illustrated in Figure 3: pre-operative (Pre) and post-operative (POP) compliance of the VEPTR group is lower than that of normal controls, but the slope of improvement matched that of normal controls.
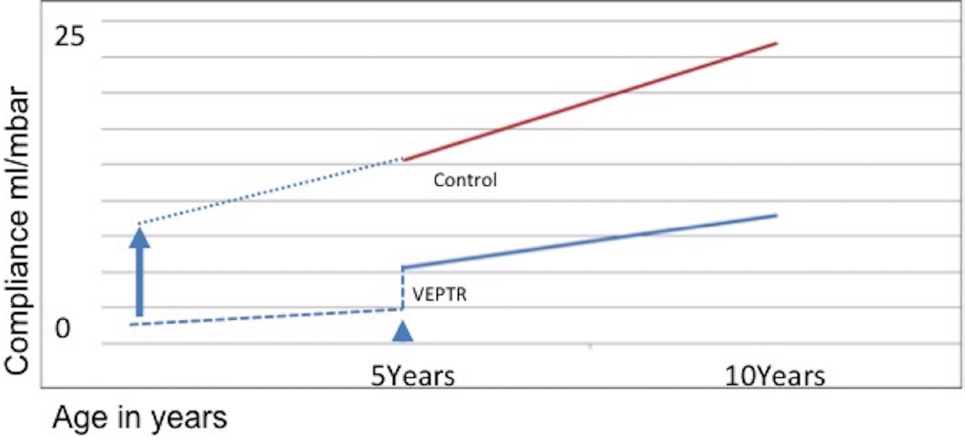
Development of thoracic compliance during growth. The vertical expandable prosthetic titanium ribs (VEPTR) group showed a lower thoracic compliance than the control group at the beginning of treatment and at the end of treatment. Increase rate of thoracic compliance during growth did not show any statistically significant differences. Assuming that treatment would begin earlier, the same increase rate of thoracic compliance during growth could lead to a ‘normal’ thoracic compliance at the end of treatment. The arrow head indicates start of treatment (mean age in this study). The dotted line at the left of the arrow head indicates assumed thoracic compliance before treatment. The arrow indicates the theoretical start of treatment as early as possible. The dotted line right to the head of the arrow indicates theoretical thoracic compliance of patients whose treatment started as early as possible. VEPTR, thoracic compliance of VEPTR group; Control, thoracic compliance of healthy control group.
Differences in age and follow-up period between both groups were not significant (p > 0.05).
Sagittal balance
Apart from initial pelvic incidence (PI), pelvic tilt (PT) and sacral slope (SS) (p < 0.05), we did not find any statistical significant differences between the development of parameters of sagittal balance during growth between the VEPTR group, the group who received ala hooks and the healthy control group: SS Pre-POP difference, PT POP to PT Pre-POP difference, PI POP to PI Pre-POP difference, SS at LFU, PT at LFU, PI at LFU, SS POP – SS LFU difference, PT POP – LFU difference, PI POP –LFU difference (p > 0.05). Table 2 shows the descriptive data.
Parameters of sagittal balance of vertical expandable prosthetic titanium ribs (VEPTR) group, control group sagittal balance and control group ala hook
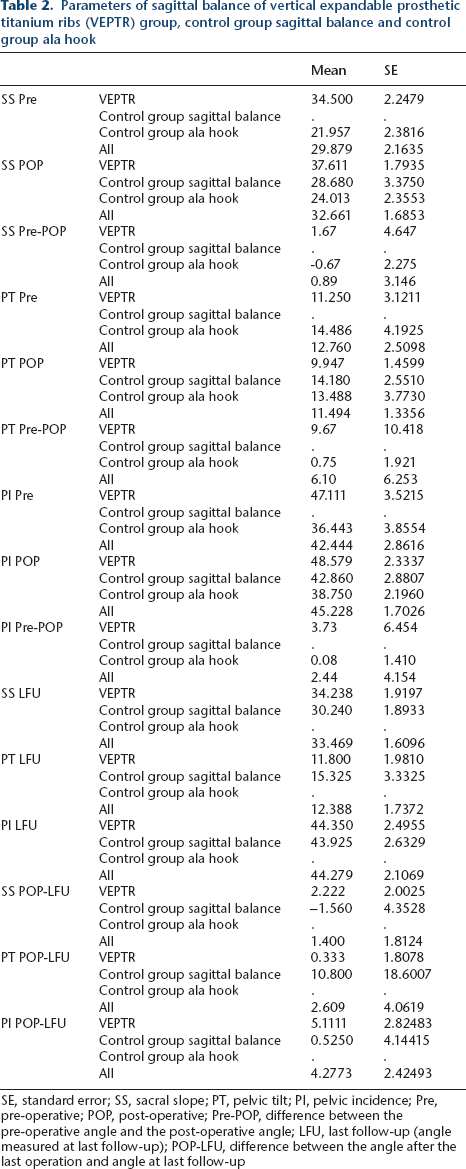
SE, standard error; SS, sacral slope; PT, pelvic tilt; PI, pelvic incidence; Pre, pre-operative; POP, post-operative; Pre-POP, difference between the pre-operative angle and the post-operative angle; LFU, last follow-up (angle measured at last follow-up); POP-LFU, difference between the angle after the last operation and angle at last follow-up
Correction of frontal Cobb angle
In the VEPTR group, we saw a mean correction of Cobb angle after the first operation of 16.41° (SE 3.01). We saw a loss of correction of 8.23° (SE 3.22) at LFU. Data are shown in Tables 3 and 4.
Cobb angles of the vertical expandable prosthetic titanium ribs (VEPTR) group
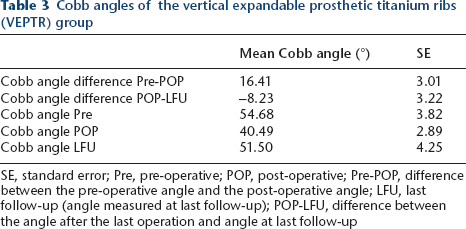
SE, standard error; Pre, pre-operative; POP, post-operative; Pre-POP, difference between the pre-operative angle and the post-operative angle; LFU, last follow-up (angle measured at last follow-up); POP-LFU, difference between the angle after the last operation and angle at last follow-up
Cobb angles of ala hook group
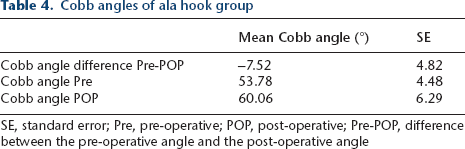
SE, standard error; Pre, pre-operative; POP, post-operative; Pre-POP, difference between the pre-operative angle and the post-operative angle
Complications
Complications were recorded in seven patients in the VEPTR group.
Five patients sustained mechanical complications: three rib–anchor dislocations, one lamina hook dislocation and two rod breakages.
Three patients sustained soft-tissue complications from implant-related ulcers. Two patients could be managed by local revision and one patient received defect repair by a local musculocutaneous flap. All complications could be managed without further recurrent complications.
Discussion
Thoracic compliance
Other study groups reported that thoracic volume, SAL and FVC increased with the same rate as in healthy children after surgery with VEPTR.3–6
Thoracic volume and space available for lungs are static parameters and measurement of FVC is dependent on the interaction with the patient who has to be cooperative and very motivated for the required tests. For patients with a mean age of five years it seems very difficult to obtain valid results.
We measured DTC by applying a method that does not depend on the co-operation or motivation of the patient (who was under general anaesthesia) and therefore investigated valid dynamic parameters over a period of 60.67 months (SE 4.77).
We measured dynamic and not static compliance in our patients since it was more accessible for this study. Popow and Simbruner 13 stated that dynamic and static compliance are strictly correlated to each other, so the choice of either parameter did not cause any bias.
A group of untreated patients with EOS would have been the ideal control group to compare the intervention (VEPTR implantation) with natural history, but not treating EOS patients who are admitted to our unit is not an option. This is why we chose a control group of healthy patients. The aim of our treatment is to enable our patients to have functional capacities as close to normal as possible and our results show how far we get by applying VEPTR.
Scar tissue, titanium rods and unintended ossifications at the ribs (which are reported to occur in 50% of EOS patients with VEPTR) 7 theoretically increase stiffness of the thoracic wall. Despite that, in our group of patients who were treated with VEPTR, we found an increase of dynamic compliance during growth in the same rate as in healthy controls, thus VEPTR seems to support children with EOS in developing their compliance as positively as healthy controls. Possible reasons for VEPTR allowing the total compliance to increase even when scar tissue and the titanium rods and ossifications theoretically counter that effect may be the mechanics of VEPTR. The pressure force vector of the VEPTR clamps is oriented cranially in the cranial clamp and caudally in the caudal clamp, resulting in forces that do not counter expansion of the thoracic wall.
We performed an additional analysis and compared the subgroups of patients with unilateral (7/21 patients) and bilateral (14/21) VEPTR implantation. In a two-sided t-test, the difference between the groups was not significant (p < 0.05), which further supports the finding that the rib cage with VEPTR shows a similar improvement of thoracic compliance during growth than those without.
On the other hand, in our control group, there was a higher level of lung compliance than in the scoliosis group before the first surgical procedure and this difference remained until the end of follow-up.
In our study, patients with EOS showed a lower initial thoracic compliance compared with healthy children that would subsequently deteriorate without treatment and may have ended up in a TIS. 2 By surgically correcting these children, we could prevent deterioration of thoracic compliance. Also, an increase of total compliance similar to that of a healthy control group could be shown but without catching up to the higher level of the controls. A similar effect was described for thoracic volume, SAL and FVC in recent studies.3–6 The reason may be that pulmonary development is strongly influenced by thoracic volume and structure in a very young age1,2,14–16 and we do not operate on our patients before the age of one to two years. In patients without rib synostosis, thoracic compliance is impaired by reduced thoracic height (cranio-caudally) and spinal rotation. 2 Having shown a similar increase in compliance after the initial procedure, we should consider treating our patients as early as possible and try to achieve the highest degree of initial correction of the spinal deformity as possible to support pulmonary development (Fig. 3).
Coronal balance and complications
In our study, the initial correction of Cobb angle by VEPTR instrumentation was 16.41° (Tables 3 and 4). The complication rate was 33% (7/21). Elsebai et al 17 reported an initial correction of 21° and a complication rate of 42% with the growing rod technique with a lower mean time of follow-up (four years vs five years). Bess et al reported a complication rate of 58%. 18 Comparing both techniques, VEPTR shows an acceptable correction of the deformity with a slightly lower rate of complications.
Sagittal balance
Mac-Thiong et al 19 reported a change in PT and PI during growth in healthy children. We did not observe a significant difference in these parameters between the VEPTR group and the control group, which may indicate that ‘VEPTR patients’ show a development of their sagittal balance which is comparable with healthy children. Initial pelvic parameters of sagittal balance were different in the ala hook group compared with the VEPTR group. Since these parameters (PI) seem to be a ‘spinal fingerprint’, a different result in each patient was to be expected.
The main limitation of our study is the low number of patients and the fact that we could not analyse the C7 plumb line as full spinal radiographs were not available in our control group.
However, we did analyse a control group for every parameter of main interest (DTC, impact of VEPTR on sagittal balance, impact of ala hooks on sagittal balance) and our control group for thoracic compliance did not show a significant difference in age and time of follow-up compared with our VEPTR group, which reduces the bias. Mac-Thiong et al 19 reported a change in PT and PI during growth in healthy children, which is why we concentrated on these parameters and the bias caused by the missing C7 plumb line is reduced.
VEPTR seems to lead to an increased rate of DTC that is similar to healthy controls, but the difference could only be stabilised and not be reduced in patients with a mean age of 5.26 years. Therefore, VEPTR treatment should be initiated as early as possible. Sagittal balance showed a similar development compared to healthy children.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
The study was conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki and its later amendments. For this type of study formal consent is not required.