
Abstract
Objectives
To study the effect of an educational intervention on paediatricians’ knowledge, attitudes and practices regarding children's environmental health and to identify the sources of information and common environmental history taking constrains.
Design
Before and after study.
Setting
Zagazig University Paediatric Hospital.
Participants
Practising paediatricians from all specialty units.
Main outcome measures
The outcome of a specifically designed educational programme about paediatric environmental health was assessed using structured pre- and post-test questionnaires.
Results
Nearly half the participants were aware about most of the paediatric environmental health-related topics. Textbooks/guidelines (85.7%) and the Internet (64.3%) were the main sources of information. The participants demonstrated relatively strong positive attitudes towards the importance of children's environmental health. However, less than half of them (44.6%) reported environmental history taking as a routine practice; where lack of time (94.6%), wide range of hazardous exposures (91.1%) and lack of expertise and training (91.1%) were the main constrains. Significant improvement in participants’ knowledge, attitudes and practices was revealed after the educational programme.
Conclusions
There is a demand for continuous medical education about environmental health in paediatric practice, particularly environmental and occupational history taking.
Introduction
There are 2.18 billion children under the age of 18 years in the world; out of them 1.9 billion live in developing countries (552 million are under age 5).1,2 Infants and children confront a wide range of potential environmental hazards and are especially susceptible to toxic effects because of their developing organ systems, high rates of respiration and calorie consumption per kilogram of body weight, immature biological defences and increased exposure due to small size, diet, behaviours and other factors.3–6 Moreover, children are more susceptible to longer term and intergenerational effects of bioaccumulation. 7
DECLARATIONS
None
None
Proposal acceptance was obtained from the Zagazig Faculty of Medicine Research Ethics Committee. Informed verbal consent was obtained from all the participants during interviews
RAA
RAA designed the study and the tools, determined the objectives, analysed the data, wrote the manuscript, participated in educational intervention and submitted the manuscript. AAA revised the tools of the study and conducted the pilot study and the educational intervention. All the authors have revised and approved the final version of the manuscript
Amal Saad-Hussein
Over 10 million children aged less than five years die every year; 98% of them in developing countries. The ‘big killers’ in children under five years of age are diseases that have a strong environmental component: unsafe water and food as well as poor sanitation (cause diarrhoea that kills 1.6 million children/year), indoor air pollution from biomass fuels and tobacco smoke (causes acute respiratory infections that kill one million children/year), the proliferation of vectors in the environment (causes various diseases such as malaria that kills one million children under five/year, mostly in Africa) and unintentional physical injuries (kill 300,000 children annually attributed to drowning, fires, falls, poisoning, road traffic incidents and other injuries).5,8–10 Moreover, a combination of environmental hazardous exposures from heavy traffic, toxic waste sites and industrial effluents can cause or aggravate diseases as diverse and as common as asthma, dermatitis, psychosocial and behavioural conditions and cancer that are termed the ‘new paediatric morbidity’.2,6
Diseases strongly linked to environmental threats are present in places where children grow, live, learn and work. In the poorer regions, the adverse effects are further exacerbated or magnified by poverty, malnutrition and stress.8,9,11,12
Environmentally related paediatric illnesses have high social and economic costs, including increased medical expenses, sick days away from school, productivity lost by parents away from work and personal agony of families.10,13,14
Recently, ‘Children's Environmental Health’ has attracted considerable attention.3,15 This field has been defined as ‘the diagnosis, treatment and prevention of illness due to perinatal and paediatric exposures to environmental hazards’, together with ‘the creation of healthy environments for children’. 7 However, paediatric medical and nursing education currently lacks the environmental and occupational health content necessary to appropriately prepare paediatric healthcare professionals to prevent, recognize and manage environmental-exposure-related diseases.12,16,17
Paediatricians’ performance regarding preventive practices such as history-taking, vaccination and lead screening is significantly affected by their knowledge, attitudes and beliefs.18,19 Hence, this study was designed to assess the outcome of an educational intervention about children's environmental health on paediatricians’ knowledge, attitudes and self-reported practices in an Egyptian university hospital and to identify the sources of information and common environmental history taking constrains.
Methods
Study design and setting
A before and after study was carried out during the period from November 2011 to March 2012 at Zagazig University Paediatric Hospital with 150 bed capacity.
Study sample and procedures
The total number of practising paediatricians in all specialty units at the time of study was 119, out of them 34 were on extended leave and 13 were excluded as they either had less than one year clinical experience (n = 7) or had participated in the pilot study (n = 6). Thus, 72 paediatricians were invited to participate in the study, where they were informed about the procedures of educational intervention. Out of the 72 paediatricians, 56 agreed to participate with a response rate of 77.8%.
Data collection and measures
Pre-test and post-test questionnaires
A structured pre-test questionnaire was used, based on those of other relevant studies and literatures review.2,4,5,11,16,20 It included four main domains. The first domain included personal and occupational data. The second domain assessed respondents’ knowledge about important paediatric environmental health-related topics, where don't know or incomplete answers were considered as wrong answers. Moreover, it included a list of different sources of information about children's environmental health. The third domain enquired about respondents’ attitudes towards children's environmental health, with emphasis on environmental history taking. The respondents were asked to rate their agreement regarding each of the nine attitude statements on a Likert scale of 1–5, from ‘strongly disagree’ to ‘strongly agree’. In the fourth and final domain, the participants were asked whether they took environmental history as a routine practice or not. Furthermore, they were allowed to choose item(s) that is/are usually included in their histories from a list of important categories of environmental exposures. Moreover, it included a list of commonly reported environmental history taking constrains in paediatric practice. A post-test questionnaire was also used to assess the outcome of the educational programme and it was similar to the pre-test questionnaire except for sources of information about children's environmental health and environmental history taking constrains.
Educational intervention
Paediatricians were invited to attend two educational sessions, one month apart, lasting approximately two hours for each. At the beginning of the first session, the respondents were personally interviewed by the investigators and were asked to fill the pre-test questionnaire after taking their consent. Then, the investigators presented a specifically designed educational material about paediatric environmental health that was prepared from three readymade power point presentations10,21,22 and from other relevant sources.11,20,23 Brainstorming, open discussion and group work were used during each session. At the end of each session soft copies of the educational material were distributed to all the participants. Two months later, the participants were interviewed personally and were asked to answer the post-test questionnaire to assess the outcome of educational intervention.
Pilot study
Before carrying out the study, the designed questionnaire and the educational material were tested on six paediatricians, where some modifications were done to improve clarity and convenience.
Data management
Data were computerized and statistically analysed using SPSS version 19. 24 A paired t-test was used for the paired quantitative data, whereas Mc Nemar's χ2 test was used for the paired qualitative data. The significance level was considered at P value <0.05.
Results
Personal and occupational data
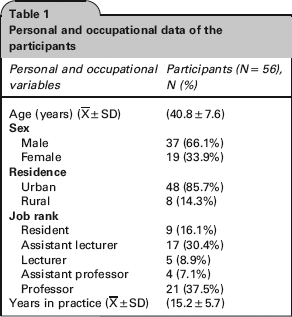
Out of the 72 practising paediatricians, 56 agreed to participate with a response rate of 77.8%. All the job categories and paediatric specialties were represented in the study. The mean age and years in practice for participants was (40.8 ± 7.6 and 15.2 ± 5.7, respectively). Men represented the majority among participants (66.1%). Moreover, the majority of participants were from urban residence (85.7%) (Table 1).
Personal and occupational data of the participants
Sources of information about children's environmental health
The participants of the present study reported that textbooks/handbooks/guidelines (85.7%), Internet (64.3%), conferences and workshops (42.9%), and journals and newsletter (41.1%) were the main sources of information about children's environmental health. Continuous medical education classes (26.8%), colleagues’ opinion (12.5%) and videos (5.4%) were reported as less important sources for participants’ information (Figure 1).
Percentage of participants according to their main sources of information about children's environmental health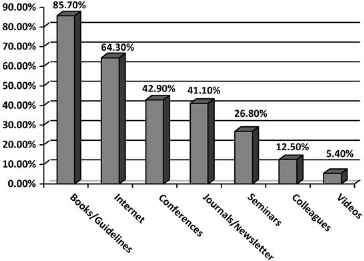
Paediatricians’ knowledge, attitudes and practices before and after educational intervention
Pre-test results revealed that the majority of the participants gave correct answers about gene–environment interactions (85.7%), causes of increased children's vulnerability (69.6%) and chronic illnesses associated with environmental pollution (66.1%). Moreover, about half the participants were aware about the other paediatric environmental health-related topics except ‘the importance of environmental history taking’, where only 41.1% gave correct answers about this issue. After educational intervention, the post-test results revealed statistically significant improvement in participants’ knowledge in all previously mentioned paediatric environmental health-related topics (Table 2).
Frequency distribution of participants according to their knowledge about environmental health before and after educational intervention

Pre-test results revealed relatively high scores of attitudes in most of the children's environmental health statements. Also, the participants reported strong disagreement towards the negative statement ‘taking environmental history is just a more work load and time consuming activity’ (1.9 ± 0.5). After educational intervention, the post-test results revealed statistically significant improvement in attitudes’ scores in all the children's environmental health and history taking statements (Table 3).
Average scores of self-reported attitudes of participants towards children's environmental health before and after educational intervention

The results of the present study revealed that less than half the participants reported environmental history taking as a routine practice (44.6%), which was significantly improved after educational intervention to (66.1%) (P < 0.001) (Figure 2).
Percentage of participants according to environmental history taking before and after educational intervention
The results of our study showed that nearly half the participants reported routinely asking in their histories about environmental tobacco smoke (57.1%), whereas much lower proportions of participants reported asking about pesticides (41.1%); proximity to industrial/waste disposal sites (41.1%); proximity to major highways (37.5%); water and food contamination (28.6%); and animals, plants and pets in houses (26.8%). Proximity to farms, exposure to radiation, exposure to specific toxic chemicals, moulds, exposure to other household toxic chemicals, lifestyle-related exposures and children's as well as parents’ occupations and hobbies were rarely included during history taking. After educational intervention, statistically significant higher proportions of participants reported routinely asking about most of the mentioned common environmental exposures except the history of exposure to specific toxic chemicals and children's or parents’ occupations and hobbies (P > 0.05) (Table 4).
Frequency distribution of participants according to the commonly asked environmental exposures before and after educational intervention

Environmental history taking constrains
The participants of the present study were allowed to choose one or more of multiple environmental history taking constrains in paediatric practice; lack of time (94.6%), wide range of hazardous exposures (91.1%) and lack of expertise and training in this field (91.1%) were the main reported constrains, whereas, a lower proportion of participants (48.2%) considered the absence of widely used, valid and reliable history taking forms as an important constrain (Figure 3).
Percentage of participants according to common environmental history taking constrains
Discussion
Our results regarding the participants’ main sources of information about children's environmental health partially coincide with those of other survey studies; where the American Academy of Pediatrics’ handbook/guidelines (89.0%, 89.9%), newsletter and professional literatures (67.5%, 71.8%) and government agencies’ publications (58.8%, 57.8%) were the preferred sources of information more than Internet-based sources. However, the results of these studies revealed that continuous medical education classes can also be considered as one of the most helpful sources in obtaining further information.2,16 This partial discrepancy may be attributed to the growing use of computers and Internet overtime. Moreover, the studied paediatricians in both American studies were from different practice setting sectors (private, public, teaching and research) and from different levels of health care (primary care, specialty and emergency care).
Regarding participants’ knowledge about paediatric environmental health, our results disagree with those of another study in which a few paediatricians were found to have sufficient knowledge about environmental and occupational health issues despite the high public concern for environmental hazardous exposures and the associated health effects. 8
Paediatricians can help limit children's exposure to environmental hazards, but few studies have assessed their attitudes towards discussing and dealing with environmental and occupational health issues. 25 In an American survey study, paediatricians reported less strong attitudes than in our study; where the mean scores of attitudes towards positive statements ranged from 3.91 ± 0.69 to 3.97 ± 0.7 and towards negative statements ranged from 3.06 ± 1.12 to 3.53 ± 0.97. 16 This finding may be due to the fact that paediatricians included in the American survey were from different practice setting sectors and from different levels of healthcare practice; whereas the participants of our study were staff members of a university hospital who are usually more qualified and trained than paediatricians in other health sectors. However, similar to the finding of our study, New York paediatricians agreed relatively strongly that the role of environment in children's health is significant (4.44 ± 0.72) and assessing environmental exposures through history-taking in paediatric practice is of great importance (4.09 ± 0.98). Moreover, they agreed relatively strongly that environmental history-taking would help parents protect their children from hazardous environmental exposure (3.99 ± 0.72) and would help identify exposures related to health concerns (4.07 ± 0.75). Also, there was overwhelming disagreement regarding some important statements as environmental history-taking is not necessary (1.57 ± 0.73) and time consuming (2.49 ± 1.01) as well as paediatricians have control over environmental health hazards (2.89 ± 0.84). The authors of the American study attributed their findings to the high interest level of the majority of their participants (88.1%) in learning more about environmental health. 2
Clinical practice plays an important role in advancing and protecting children's environmental health. The environmental and occupational history is readily included in the routine medical history. Yet healthcare providers seldom elicit an environmental or occupational history from their patients. 26 Our finding partially agrees with that of another study which investigated paediatricians’ self-reported interview practices; where about half the participants reported taking history as a routine practice that included asking about cigarette smoking around the child, parental occupation and housing. 2 In the present study, after educational intervention a statistically significant higher proportion of the participants reported environmental history taking as a routine practice. This result can be explained as it was revealed that paediatricians who are confident about environmental history-taking (high self-efficacy) and who expect useful information from this part of the history (high outcome expectancy) are more likely to take a history than other physicians without these attitudes. 16
The results of the current study revealed that environmental tobacco smoke, exposure to pesticides, proximity to industrial/waste disposal sites and proximity to major highways were the most commonly asked environmental exposures during history taking. After educational intervention, significant higher proportions of participants reported routinely asking about most of the common environmental exposures except for exposure to specific toxic chemicals and children's or parents’ occupations and hobbies. Our findings partially coincide with those of another study that investigated paediatricians’ self-reported interview practices in Georgia, where the majority of respondents reported routinely asking about cigarette smoking around the child (88.2%), pets in home (73.7%), source of drinking water (65.4%), lead (59.6%) and housing (54.4%) while about half the respondents reported asking about sun exposure, lifestyle factors, parental occupation, moulds, home heating sources and indoor air. Moreover, fewer than 5% of the participants reported asking about outdoor air pollution, hobbies and specific toxic chemicals. 16 The discrepancies in the results of both studies may be attributed to cultural differences as in Western countries presence of pets in homes is more common than in our countries. Moreover, countries’ differences regarding sources of environmental pollution can be a logical explanation, where widespread environmental contamination from pesticide usage in agriculture, industrial and waste disposal sites, as well as from motor vehicle exhausts emitted near highways are major environmental problems in our country.
Our finding supports that of another study which revealed routine questions about different environmental exposures during history taking by high percentages of paediatricians, where this finding was attributed to received training on environmental history taking before conducting the study. 2 Furthermore, another study revealed that relatively few physicians were specifically trained to recognize or prevent environmentally or occupationally induced illness in children, despite its importance because of either children's work or family members’ work ‘take home contamination’. Hence, it is documented that most of the environmental and occupational illnesses may go unnoticed. 27
Regarding environmental history taking constrains in paediatric practice, lack of time, wide range of hazardous exposures and lack of expertise and training in this field were the main constrains reported by participants of this study. Our finding coincides with those of other studies, where the paediatricians reported perceiving some logistic barriers, such as lack of expertise and training in the field of paediatric environmental health as well as time, effort and cost, to incorporate environmental history in their routine practice.16,28 Paediatricians in other studies also indicated a significant demand for continuous medical education regarding environmental health issues especially as hundreds of new chemicals are developed every year and released in varying quantities into the environment.2,25,29
Limitations of the analysis
The results of the present study are based on paediatricians’ self-reported attitudes and practices, where the social desirability of the ‘right’ answers may overstate the level of attitudes and practices.
Implication for future research and clinical practice
Our findings indicate a significant demand for integrating environmental and occupational health into paediatricians’ education, training and research. Moreover, our data point to the urgent need of strengthening the role of governmental health agencies in providing paediatricians with the necessary information and guidelines regarding children's environmental health that enables paediatricians to address environmental conditions that may prevent a child from reaching optimum health. Investing in researches in the field of children's environmental health should be given priority in our country emphasizing on interventional studies.
Conclusions
It could be concluded that improving paediatricians’ awareness, attitudes and practices about children's environmental health is an urgent need, yet it is not a difficult task. Improving history taking of child exposure to specific toxic chemicals as well as of children's or parents’ occupations and hobbies still needs more training and educational programmes.
Footnotes
Acknowledgements
The authors of the study would like to thank the head and the staff members of Zagazig University Paediatric Hospital for their cooperation