
Abstract

This case of a young lady with chronic pancreatitis mimicking pancreatic cancer demonstrates how genetic testing helps surgical management.
The authors have no competing interests and have received no specific funding or sponsorship for this submission
None declared
This work was not part of a trial and so ethical approval was not required
The authors have contributed to this paper as follows: Nicholas Faure Walker – involved in care of patient and main author; Oliver J. Warren – involved in care, reviewer of manuscript and of literature; Lynsey Gawn – involved in care of patient, information collection and review of manuscript and Long R. Jiao – consultant in charge of care and senior author
Michel Kahaleh
Case history
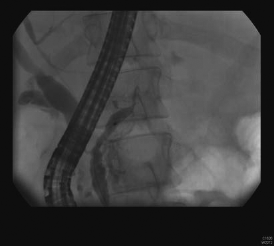
A 26-year-old Gujarati lady nine months pregnant with her first child, presented to her local emergency department with severe epigastric pain radiating to the back, vomiting and a fever. She had no history of cholelithiasis, was on no regular medication, had never drunk alcohol and had no family history of chronic pancreatitis, cystic fibrosis, hyperlipidaemia or chronic abdominal pain. Investigations showed raised amylase, but normal calcium, lipid profile and renal function. An abdominal ultrasound did not reveal any biliary calculi. Blood cultures were positive for Klebsiella. The patient underwent an emergency caesarean section, delivering a healthy child but required intensive care unit admission for 14 days. A computed tomography (CT) scan showed focal interstitial pancreatitis with extensive calcification, and a bulky inflammatory mass associated with an ectatic pancreatic duct at the tail of the pancreas. She was admitted again two months later with a further bout of acute pancreatitis and recurrent Klebsiella septicaemia, and following discharge experienced ongoing abdominal pain over the next year. When she presented with a third acute flare of pancreatitis she was referred to our regional Hepato-Pancreato-Biliary (HPB) unit for further investigation and management. Upon admission she had a normal full blood count, urea and electrolytes. Her C-reactive protein was 19, amylase 130, anti-neutrophil cytoplasmic antibodies (ANCA) PR3 40 (normal <26), anti-beta-2 glyco protein 1, IgG 11 (normal <7). Malaria parasites, blood cultures, rheumatoid factor, anticardiolipin IgM, ANCA IF, ANCA MPO, anti-GBM, cytoplasmic antibody (Hep-2) and HIV tests were all negative. C3 and C4 levels were normal. A CT scan of her abdomen showed signs of acute on chronic pancreatitis with extensive calcification at the body and head of pancreas, and a bulky inflammatory mass associated with an ectatic pancreatic duct at the tail (Figure 1). Endoscopic retrograde cholangipancreatography (ERCP) was attempted (Figure 2) but it was not possible to insert a stent to bridge the disrupted pancreatic duct at the proximal body of the pancreas. Given the CT appearance, we were concerned that she might have developed pancreatic cancer (PC) at the tail of her pancreas on the background of chronic pancreatitis. Clinically, the patient continued to experience persistent severe epigastric pain refractory to pharmaceutical management. She underwent a laparoscopic distal pancreatectomy with spleen preservation. She was found to have a severely inflamed tail of the pancreas and a giant mass around the tail involving the colonic mesentery, the stomach and the splenic vessels. However, it was still possible to safely dissect the mass from the splenic vessels to preserve the spleen and prevent the sequelae of splenectomy as no definitive diagnosis of cancer was made pre-operatively. Histology demonstrated the pancreatic parenchyma to have been completely replaced by fibrous tissue, but no malignant change was identified. Postoperative recovery was unremarkable and the patient was discharged on day 5. At outpatient follow-up six weeks later she was asymptomatic and taking no analgesia. Subsequent genetic testing revealed that she was positive for the serine peptidase inhibitor Kazal type 1 N34S gene mutation (‘SPINK-1 N34S’) but negative for the cationic trypsinogen gene R122H mutation (‘PRSS1 N34S’).
Computed tomography of the abdomen showing enhancement of the tail of the pancreas and pancreatic duct dilation and new retroperitoneal fat streaking Endoscopic retrograde cholangiopancreatography showing obstruction of the pancreatic duct
Discussion
Chronic pancreatitis is a destructive inflammatory process which can lead to total destruction of the pancreas with subsequent malabsorption, secondary diabetes and severe unrelenting pain. Alcohol is the commonest causative factor for the development of chronic pancreatitis, accounting for 70% of cases in the UK. 1 However, almost a third of cases are classified as idiopathic as no obvious cause is found. Increasingly, a genetic predisposition is believed to be contributory in this group of patients. The serine peptidase inhibitor Kazal type 1 (SPINK-1) N34S mutation, the cystic fibrosis transmembrane conductance regulator (‘CTFR’) gene and the R122H and N291 mutations in the cationic trypsinogen gene (PRSS1) have all been shown to be risk factors for the development of chronic pancreatitis. 2 SPINK-1 is thought to lower the threshold for the development of pancreatitis by preventing premature accelerated autolysis of trypsin 3 thus reducing trypsin activity by as much as 20%. 4 The N34S mutation has been found in 13–37% of those with intrahepatic cholestasis of pregnancy (ICP) compared with 2.5–5.1% in normal populations.3,5 In Threadgold et al.'s study including 91 patients with ICP, 15 (16%) were positive for the N34S mutation. They found the mutation did not statistically affect age of onset, pancreatic exocrine deficiency, duration of illness, frequency of exacerbations, hospital admissions or the need for surgery. 5 However Sandhu et al.'s study from 2011 including 35 ICP patients, of whom 37.1% were SPINK-1 N34S positive, showed that this subgroup were more likely to suffer acute flares compared with controls without the mutation (11.8 [+1.5] versus 4 [+0.98]) over a 9.6 year follow-up. No statistical difference in age of onset, exocrine insufficiency or magnetic resonance cholangiopancreatography or ERCP scoring was demonstrated and none of their cohort developed PC in the time of the study. 3 Piepoli et al.'s 6 2006 case control study of 61 Italian patients with PC and 106 healthy controls found no relation between SPINK-1, UGT1A7, UGT1A9, ARP or CFTR gene polymorphisms and PC. SPINK-1 has not shown to be an independent risk factor for the development of PC to date.
The risk of developing PC with chronic pancreatitis is difficult to estimate but Malka et al. 7 estimated their cohort (85% with alcoholic chronic pancreatitis) to have a standardized incidence ratio (SIR) of developing PC of 19.0 although earlier studies have shown the SIR to be lower. Lowenfels et al. 8 found in 2006 that the SIR of developing PC in patients with hereditary chronic pancreatitis (HCP) was 50 representing a risk of one in 1066 person years. The EUROPAC study is the largest study of patients with hereditary pancreatitis to date with 527 subjects: 82% of the 399 genetically tested had a PRSS mutation and the R122H was the commonest. They found the cumulative risk of developing PC was 1.5% at 20 years, 2.5% at 30, 8.5% at 40, 14.6% at 50, 25.3% at 60 and 44% at 70 years after the onset of HCP but the risk was not significantly altered by the PRSS mutation status even though 78% of their cohort had a PRSS mutation. 9
Chronic pancreatitis is clearly a risk factor in the development of PC but chronic pancreatitis can also present with weight loss, abdominal pain, nausea, diarrhoea and steatorrhoea which mimic PC. PC five-year survival is less than 5% so a low threshold for operative intervention is needed. It can be very difficult to distinguish between malignant and inflammatory masses from chronic pancreatitis on CT. Twelve percent of isolated pancreatic duct strictures identified on CT have been found to be malignant. 10 The EUROPAC study also found that pancreatic calcification was found more often in whose with HCP who went on to develop PC. 9 The decision to operate is further complicated by the relatively high operative morbidity and mortality.
This was the first patient with chronic pancreatitis to be found positive for the SPINK-1 N34S mutation at our tertiary referral HPB unit in London. The SPINK-1 and PRSS1 gene mutations have been well investigated and should now be offered to patients with chronic pancreatitis of unknown aetiology as they help quantify the lifetime risk of developing PC and hence the need for total pancreatectomy in patients with chronic pancreatitis (Table 1). In this case, the patient was spared TP as she was found to be SPINK-1 N34S positive and PRSS1 gene mutation negative.
Summary of gene mutations and their associated risks of pancreatic cancer

Footnotes
Acknowledgements
The authors have no further acknowledgments