
Abstract
Objectives
To conduct an exploratory study to learn about the experiences of GPs who have undertaken international work.
Design
Cross-sectional survey
Setting
Online survey of UK-based GPs. Members of all UK RCGP faculties were invited to participate by email and the survey was publicised on the RCGP website
Participants
All UK-based GPs
Main outcome measures
Types of UK and international work undertaken, barriers, competencies gained, influence on career and future plans.
Results
The study identified 439 respondents, in a variety of GP roles at all career stages, who had undertaken international work in their role as a doctor. GPs are undertaking international work in both high and low/middle-income countries, engaging in a wide range of clinical and non-clinical activities. Respondents reported gaining a range of competencies from international work, which could be transferred back to the UK setting to a variable degree. Commonly cited barriers to international work were having to leave friends and family, and concerns regarding future employment and pension. Most reported that engaging in international work had influenced the direction of their career, with the largest proportion stating that they wish to work predominantly in the UK, with some international work in the future.
Conclusion
The study highlights the variety of ways in which UK GPs are combining UK general practice and international work, competencies gained with such work, and ability to transfer these back to the UK setting. Historical barriers to international work still exist and future research could further examine the value of such work.
DECLARATION
Authors are members of the RCGP Junior International Committee and have a keen interest in international medical work
The authors are grateful to the RCGP for funding the cost of Survey Monkey questionnaire software
The study design was discussed with the NIHR Research Design Service who indicated that formal ethical approval was not required. The study did not involve any direct patient contact
CS, LP, HS, and JD
Chris Smith (NIHR In-Practice Fellow, Imperial College) conceived the study. LP, HS, and JD contributed to writing the questionnaire, performing the analysis, and writing the manuscript
Introduction
Doctors from the UK have a long tradition of working overseas for part of their careers, both in high and low/middle-income countries. 1 Recent years have seen a growing interest and opportunity to engage in global health, reflected in the expansion in UK Health Links, Global/International Health BSc and MSc programmes, and organizations such as Alma Mata, MedSin, and the Royal College of General Practitioners (RCGP) Junior International Committee.2–5
A number of reports have highlighted the potential role of the UK government and NHS in addressing global health issues, including the 2007 Crisp report, ‘Global health partnerships: the UK contribution to health in developing countries’, and the subsequent UK government's responses. 6 9 These highlighted both the healthcare human resource crisis affecting many developing countries, and the potential benefits, particularly non-clinical, to individuals and the NHS resulting from overseas work.
Within the UK policy context, there has been a growing emphasis on leadership in the NHS, and the identification of the competencies doctors need to become more actively involved in the planning and delivery of services for patients. 10 12 This has most recently been expressed in the NHS Leadership Framework, informed by analysis of existing NHS leadership data and leadership literature. 13 The introduction of revalidation may focus attention on the identification and documentation of such competencies.
However, little is known about international work undertaken by UK GPs. The aim of this exploratory study was to learn about experiences of GPs who have combined UK general practice and international work, in particular:
Types of UK and international work undertaken;
Barriers to undertaking international work;
Competencies gained with international work and ability to transfer competencies back to the UK;
Influence on career and future plans.
Methods
We conducted an online questionnaire-based descriptive study of UK-based GPs and GP trainees using Survey Monkey software. We designed a questionnaire consisting of 12 questions that sought to address the study aims using a mixture of scale items and free text boxes. Questions relating to competencies gained included those outlined in the NHS Leadership Framework; established as a single overarching leadership framework for all NHS staff (Figure 1). 13 We piloted the questionnaire with small groups of GPs on three occasions and made adjustments, particularly scale items. An invitation to participate in the survey appeared during August 2011 on the homepage of the RCGP website and an email invitation to participate was sent to all UK RCGP faculties requesting these to forward the invitation to all RCGP members in their catchment area. The email invited all UK-based GPs to respond regardless of whether they had or had not undertaken international work. Although there are approximately 44,000 RCGP members, it was not possible to estimate a response rate, as it was not possible to determine how many people viewed the RCGP website link and whether all RCGP faculties effectively cascaded the invitation.

Domains of the NHS Leadership Framework (taken with permission from the NHS Leadership Framework)
Questionnaire data were exported into Microsoft Excel for analysis. Quantitative data were presented as proportions. For the qualitative (free text) results we conducted a thematic analysis using NVIVO software. 14 Recurring themes were independently identified by two authors and subsequently compared.
Results
There were 594 responses (approximately 1.4% of the RCGPs total membership), of whom 439 (74%) had undertaken international work in their role as a doctor. Responses were received from doctors at all career stages ranging from those in GP specialty training (19%), less than 5 years post-qualification (28%), 5–15 years post qualification (20%), 15–35 years post-qualification (27%), >35 years post-qualification (1.9%), through to retirement (4.6%).
Types of UK GP work undertaken
Respondents were asked what type of UK GP work they predominantly undertook before and after undertaking international work (Figure 2). The top three reported types of UK work undertaken by respondents in the six months immediately prior to working abroad were GP speciality training (24%), work in another speciality (21%), and GP partner (19%). The top three reported types of UK work undertaken by respondents in the six months immediately after working abroad were GP locum (23%), GP speciality training (21%) and GP partner (20%).

Reported UK roles during the majority of time in the six months before and after undertaking international work (numbers rather than percentages displayed)
A number of themes arose from the free text analysis. Some respondents undertook international work as part of their GP training or took advantage of natural breaks between career changes. Some GP partners indicated use of sabbaticals for international work:
‘[I was a] full time GP partner - did it as part of my sabbatical and now go every year. ’
A higher proportion of respondents had worked as locums after time abroad (23%) compared to before (14%). Some respondents reported difficulties in finding work on returning:
‘It was a very difficult transition finding work after returning from working abroad.’
In contrast, a few respondents commented that the GP retainer scheme was helpful on returning from abroad:
‘The thing that really helped me to get back into General Practice was the GP Returner Scheme - fantastic - I had six months full time paid job through this scheme and then joined a partnership.’
Several respondents reported returning to work as locums in specialties other than general practice and some respondents were still abroad at the time of completing the questionnaire.
Types of international work undertaken
Many respondents (47%) had not spent more than a year abroad in total as part of their career. However, 39% reported spending between one and five years abroad, with a further 15% having spent more than five years abroad.
Respondents reported undertaking a variety of lengths of international placements. Long-term visits of greater than six months were more commonly reported (65%) than medium term visits of under six months (38%), or short visits of less than a month (37%). However, of those who had undertaken short visits, 33% had done so more than five times.
Respondents reported undertaking a wide variety of international work in both high and low/middle income settings (Figure 3). The top three reported roles were clinical service delivery (non-relief setting) in a high-income country, clinical service delivery (non-relief setting) in a low/middle-income country, and teaching in low/middle-income settings. Overall, working in low/middle income settings was more common.

Type of international work undertaken
Respondents reported having worked with a variety of different non-governmental organizations such as Médecins Sans Frontières; missionary organizations; the British Armed Forces; or in government hospital posts.
Barriers to undertaking international work
The commonest reported barriers (to a moderate or significant degree) were having to leave family and friends in the UK (45%), concerns on being able to secure a job on return to the UK (26%), and loss of pension (22%).
Other reported concerns regarding appraisal/revalidation (21%), loss of earnings (21%) and lack of support from employer, GP partners or training deanery (21%).
A few respondents commented specifically that deaneries or Primary Care Trusts (PCTs) acted as barriers to their plans to go overseas, or made it difficult to obtain a job in return:
‘[The] PCT … seem to have no idea what their policy is and make up the rules as they go along. They caused significant delays in me getting back to work in [the] UK [as a] GP’
‘The threat of having to ‘retrain’ is ludicrous when I am working in a developed country in a primary care setting essentially modeled on the British system.’
A few stated that they had organized jobs to return to prior to leaving the UK; some reporting that they would not have left the UK had they not managed to secure this.
Competencies gained with international work and ability to transfer competencies back to the UK
Respondents reported developing a range of competencies through undertaking international work (Figure 4). In particular, moderate or significant development was reported in NHS Leadership Framework domains; 13 personal qualities such as self-awareness (89%), working with others (87%), setting direction (60%), managing services (59%), and improving services (56%). Moderate or significant development was also reported in clinical care (79%), teaching (56%), and to a lesser extent, research (19%).
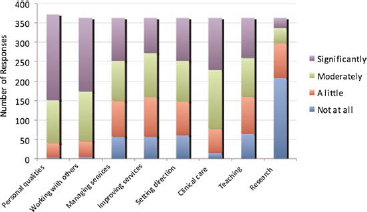
Competencies gained through international work
Additional emerging themes included reported improvement in confidence, increased ‘appreciation of the NHS’ and new ways of working:
‘One of the most significant aids to competence development was discovering that there are equally effective ways of practising medicine other than those taught in the UK’
Respondents reported being able to transfer competencies gained through international work back to the UK setting to various degrees (Figure 5).

Degree to which able to transfer competencies gained to the UK setting
Areas where respondents reported that they were most able to transfer competencies gained back to the UK setting to a moderate or significant degree were the ‘personal qualities’ (82%) and ‘working with others’ (81%) aspects of the NHS Leadership Framework, as well as ‘clinical care’ (62%), for example:
‘I now provide national and international training on quality and safety improvement’
‘I cannot emphasize enough how seeing a mind-bogglingly large number of seriously ill people has helped me in my subsequent career’
In contrast, respondents reported more difficulty in transferring competencies gained in the NHS Leadership domains of ‘setting direction’ (45%), ‘managing services’ (43%), and ‘improving services’ (41%) back to the UK setting. One challenge identified included returning to UK sessional/ locum work that offered ‘little opportunity to express the skills … learned’, for example:
‘[It] hasn't yet been possible to put some of the skills into action in a GP locum role but hopefully will be useful if I am able to become involved in commissioning or take a greater role in a practice in the future. ’
Others mentioned facing ‘narrow-minded bureaucracy and lack of recognition of what is done abroad.’
A minority reported that few competencies gained abroad were transferable back to the UK setting:
To be honest, not much was transferable back to the UK i.e. I developed culturally-specific skills most relevant for the developing country I was working in.’
Others who had worked overseas early in their careers reported difficulties in identifying competencies gained, for example:
‘Very difficult to objectively evaluate which competencies gained early on in a career have proved influential on making me the doctor I am today.’
Influence on career and future plans
Approximately two-thirds of respondents indicated that working overseas had influenced the direction of their career in some way. Some reported an increased desire to undertake more international work, or that international work initiated or confirmed their choice to go into general practice, for example:
‘My experience overseas taught me where I could be most useful in the UK for patients (i.e. GP rather than surgeon).’
Others subsequently actively chose to work serving a multicultural population in the UK as a result of their overseas experience. There was also increased interest in teaching, research and public health, in some cases followed up with further relevant qualifications.
‘I recognised the need [for] teaching, so trained as a GP trainer.’
‘I first started teaching abroad and I am now an Associate Postgraduate Dean and have a Masters degree in medical education.’
Others reported a ‘positive impact’ on UK work due to ‘renewed enthusiasm’:
‘I was feeling tired and jaded before the sabbatical, but returned feeling energized and invigorated for my work as an NHS GP, which helped me to decide to stay in this line of work.’
However, some respondents indicated feeling that their career had been negatively affected by international work. Examples for this included loss of partnerships and difficulty getting a substantive post on returning. Some appeared to resign themselves to the notion that having been out of the country for over two years, it would be very difficult to come back:
‘significant bureaucratic barriers… regarding returning to UK practice - in effect I have probably burnt my bridges now that I have been overseas for more than 2 years.’
The breakdown of respondents ideal future career was as follows; predominantly UK GP work with some international work (52%), UK-based work only (18%), international work only (6%), predominantly international work with some UK work (4%), an equal amount of UK and international work (12%).
Examples given of international work that people wanted to combine with UK work included teaching, clinical work in low-income countries, and humanitarian work.
Some gave examples of how they would ideally like to combine both; a ‘couple of years in the future’, or to ‘find a long term job in the UK where I will be able to combine short-term voluntary working trips abroad in the future.’
Discussion
Summary of main findings
The study identified a number of UK GPs undertaking a variety of international work, both in high and low-income countries, engaging in a wide range of clinical and non-clinical activities. Many of the respondents undertook work as a non-principal GP before and after undertaking international work, which suggests that international work is often undertaken at an early stage of a GP career, and that non-principal work may offer more flexibility to allow such work to be undertaken. Furthermore, the findings suggest that overseas work may occur at times of transition between different roles. It may also reflect the uptake of out-of-programme experiences and the flexibility early in GP careers before long-term professional and personal commitments are established.
These findings exist despite a number of barriers identified. Some respondents reported significant difficulties in obtaining local support to go overseas and lack of appreciation of such work on return to the UK.
Respondents reported gaining a number of clinical and non-clinical competencies from working overseas, in particular relating to the NHS Leadership Framework. 13 Respondents reported being able to transfer competencies such as ‘personal qualities’ and ‘working with others’ back to the UK setting to a greater extent than those concerned with ‘managing and improving services’. This might reflect lack of opportunity to undertake service improvement roles if returning to purely clinical roles in the UK. However, other examples were provided where such competencies had been transferred to the UK setting.
Engaging in international work does appear to have influenced respondents’ careers and in many cases results in a desire to undertake more overseas work, or work with underserved populations. However, perhaps encouragingly for NHS workforce planners, the most popular future plan is to undertake predominantly UK work, with some international work.
Strengths and limitations of the study
A strength of this study was that it was distributed via a variety of channels and likely reached many of the GPs who are RCGP members or access the RCGP website. However, the extent to which the survey was distributed by the different RCGP faculties was likely to have been variable. Selection bias was likely, with those more familiar with email, using online surveys, or who had undertaken international work more likely to respond. It is likely that the age profile of respondents was younger than the average for UK GPs. 15 However, the survey was not intended to estimate the proportion of UK GPs who have undertaken international work, rather to identify those that have and explore their experience. It was not apparent that only those with particular experiences or opinions responded, as a wide range of responses were received. However, recall bias may have influenced responses, particularly from those whose overseas work was many years previous, and when self-reporting competencies. Given the exploratory nature of the study, it was not possible to use other measures of leadership competencies, for example detailed behavioural self-assessment or multi-source feedback. However, using a mixed method approach allowed respondents to clarify their responses, allow examples to be provided, and identify further themes.
Comparison with existing literature
To the authors’ knowledge this is the first cross-sectional survey exploring the types of international work UK GPs are undertaking. In 1996, the British Medical Association ran a workshop exploring barriers preventing UK doctors from volunteering for overseas work. Key problems identified included training and accreditation issues, and lack of opportunities for combining an NHS career with overseas work. 16 The findings from this survey suggest that many of the same challenges still exist.
The potential benefits in terms of personal development and enhanced clinical skills from international work have been well documented. 16 18 A previous study found that UK GPs who had undertaken international travel scholarships reported increased involvement in research and service development activities suggesting transference back to the UK. 1 However, to the authors’ knowledge, this is the first study that has sought to measure those competencies against an established framework, in this case the NHS Leadership Framework. Finally, consistent with our findings, previous studies have indicated that although many doctors wish to undertake international work, most doctors return to the NHS, often engaging with underserved populations.16,19
Implications for future research or clinical practice
As interest in global health continues to increase, it is likely that the number of UK healthcare professionals undertaking international work will also increase. This study adds to the growing body of evidence that suggests that engaging in international work can aid development of a wide range of competencies that can benefit both the individual and the NHS. GPs may wish to highlight such competencies when undergoing appraisal and revalidation. However, at present, many GPs return from overseas work to purely clinical posts with limited opportunity to utilize new competencies such as managing and improving services. To benefit from GPs who have returned from international posts, GP practices, clinical commissioning groups and other NHS services could consider creating innovative posts that allow time for management or service improvement activities. Greater opportunities for job-sharing could allow GPs to integrate international work with partnerships or salaried roles whilst maintaining a degree of continuity of care for patients in the NHS.
Future research areas could include further exploration of why international work provides a unique context for learning, how competencies can best be transferred to the UK setting, and the impact of revalidation on GPs going overseas.
Footnotes
Acknowledgements
We would like to thank Liz Brown, Liz Crawford, Graham Easton, Val Wass, Dor Seo and Azeem Majeed for their assistance and advice, and all of the doctors who responded to the questionnaire