
Abstract

Although rare, spontaneous oesophageal rupture is a well described and serious cause of chest pain. Endoscopic intervention should be considered.
DECLARATIONS
None declared
None declared
Written informed consent to publish the article was obtained from the patient
ADF
All authors participated in the direct clinical care of the patient. EF wrote the manuscript; ADF revised the manuscript
Sanjay Gupta
Case report
An 83-year-old Caucasian man presented to our institution with a 16-hour history of eight episodes of vomiting which was later associated with frank haematemesis and severe epigastric/chest pain. There was no past history of note and he denied consumption of non-steroidal anti-inflammatory medications or alcohol. On clinical examination he was haemodynamically stable and there was no stigmata of surgical emphysema. Digital rectal examination did not show any evidence of melaena or haematochezia. Routine haematological, biochemical and inflammatory markers were normal. An erect chest radiograph was normal. He underwent an oesophago-gastro-duodenoscopy (OGD) within 24 h of admission, which revealed a 7.5 cm tear within the mid-oesophagus, 27 cm ab oral, with views into the mediastinum (see Figure 1a).
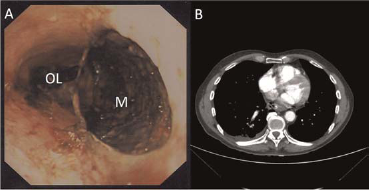
Demonstrates the endoscopy (a) and computed tomography (CT) (b) appearances at presentation. The mediastinum (M) is clearly visible and distinct from the oesophageal lumen (OL). The CT thorax demonstrates the oesophageal perforation with the presence of mediastinal air in the absence of pleural effusions
A diagnosis of Boerhaave's syndrome was made. An urgent computed tomography (CT) scan revealed free mediastinal air, in keeping with a full thickness tear of the oesophagus, (see Figure 1b). A covered metal oesophageal stent was inserted (Boston Scientific, Hemel Hempstead, UK), with a surgical feeding jejunostomy sited the following day and broad-spectrum intravenous antibiotics instituted. A water-soluble contrast study one month postadmission showed no leakage, (see Figure 2) and he was discharged five weeks after admission. The oesophageal stent was removed six weeks after presentation.
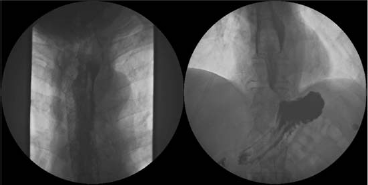
Contrast swallow after stent insertion showing no mediastinal leak
Discussion
Spontaneous oesophageal rupture, secondary to barogenic trauma, as a consequence of a rapid rise in intraluminal pressure caused by vomiting against a closed glottis, was first described by Herman Boerhaave, a Dutch botanist and physician, in the early 18th century. It has a reported mortality of between 20% and 40% and is considered by many authorities to be the most serious of all gastro-intestinal perforations. 1 Ninety percent of ruptures occur in the lower oesophagus, with the average tear being 2.2 cm in length. 2 Putative risk factors include high alcohol intake, peptic ulcer disease and eosinophilic oesophagitis.3, 4 Non-spontaneous causes of oesophageal rupture include iatrogenic perforation or rupture associated with malignancy. The former of these is associated with a better prognosis due to earlier detection, usually in a fasted patient, prompting early surgical repair. 5 Mallory–Weiss syndrome is characterized by upper gastrointestinal bleeding secondary to vomiting induced oesophageal trauma, but involves the mucosal layer only. Due to the superficial nature of the oesophageal trauma, unlike Boerhaave's syndrome, this usually runs a benign course. Diagnosis is made at endoscopy and radiological imaging is typically unremarkable. 6
Presenting symptoms are often non-specific and physical examination may not be helpful, consequentially a delay in diagnosis is common, thus greatly increasing mortality. A plain chest radiograph is almost always abnormal from the outset, commonly demonstrating free mediastinal air. A CT thorax will usually confirm the diagnosis, with contrast studies confirming the location and extent of the oesophageal leak. As a diagnostic modality, the role of OGD is controversial as insufflating air into the lumen of the oesophagus can result in further trauma and subsequently introduce more air into the mediastinum.
There are a paucity of international evidence-based guidelines and current recommendations are based on expert opinion. 7 Traditionally, expeditious surgical intervention within 24 h of perforation has been recommended to limit the degree of mediastinal contamination. 8 The type of surgical intervention depends on the size and site of the tear and the presence or absence of any associated complications, with primary repair considered by many to be the optimal surgical intervention. 9 Endoscopic management has an emerging and efficacious role, particularly with the advent of covered, self-expanding metal stents. 10 Conservative management has been trialed in patients with a contained perforation; they require close monitoring and parenteral nutrition for several weeks, with rapid treatment of infections and drainage of collections. Nevertheless, given the relative rarity of this condition, most physicians’ experience with this condition will be limited, and thus decisions on best therapeutic approach can be very challenging.
Our case highlights the initial diagnostic challenge, and management of an extremely large spontaneous oesophageal rupture using non-surgical techniques in an elderly patient. We are of the belief that prompt endoscopic intervention and early institution of enteral feeding contributed to a positive outcome. Although rare, chest pain in a patient with a history of vomiting must arouse the suspicion of Boerhaave's syndrome in the general physician, prompting early investigation, appropriate referral and specialist management.
Footnotes
Acknowledgements
The authors thank Dr R A Manns for his contributions to the images