
Abstract
This case demonstrates how hyperpigmentation of the nipple due to Paget's disease can imitate malignant melanoma presenting a diagnostic dilemma.
DECLARATIONS
None declared
None
Written consent for publication was gained from the patient or next of kin.
RB
Samuel Leinster
Case report
A 62-year-old woman was referred by her GP to the West Sussex Breast Unit with a pigmented lesion on her left nipple that had been increasing in size for six months. She had recently moved back to the UK after living in Australia. She did report recent bleeding from the nipple that had resolved completely. She had no previous breast disease and there was no family history of breast or ovarian cancer. On examination, there was an area of hyperpigmentation of the left nipple measuring 4 × 3 mm with irregular margins, with a couple of bleeding spots on top of this (Figure 1). No breast masses were felt nor was there any evidence of axillary lymphadenopathy She was referred to dermatology and a diagnosis of possible malignant melanoma was made.
Clinical appearance of hyperpigmented left nipple
She underwent an excision biopsy of the left nipple-areola complex that involved excision of the nipple, areola and central ducts. Immunohistochemistry demonstrated that the tumour cells were strongly positive for Cam 5.2 (Figure 2), cytokeratin (CK) 7 and epithelial membrane antigen (EMA). In addition, Alcian blue and diastase PAS were both positive. Immunochemistry was negative for S-100 and Melan-A. Histopathology demonstrated a 0.7 mm focus of high-grade ductal carcinoma in-situ (DCIS) and oestrogen receptor negative. There was Pagetoid extension along the ducts with involvement of the overlying epidermis.
Pigmented variation of Paget's disease with cytokeratin (CAM 5.2) staining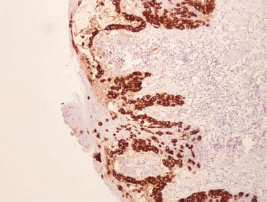
She made a good recovery postoperatively and underwent an MRI scan, six weeks following the initial surgery, that showed no evidence of widespread DCIS or any discrete lumps. A central quadranectomy – wide local excision with removal of nipple-areola complex – was done with Grisotti flap reconstruction. Final histopathology revealed no residual DCIS or invasive carcinoma.
Discussion
Sir James Paget 1 first described how clinical signs of the nipple such as itching, excoriated nipple, erythema and nipple drainage are associated with underlying breast cancer. It is an uncommon presentation of breast cancer, representing 1–3% of all new breast cancer diagnosis. 2 Cutaneous and nipple involvement from Paget's disease is believed to be due to tumour cells proliferating along the central ducts of the breast subsequently involving the nipple-areola complex.
Hyperpigmentation of the nipple due to Paget's disease is an unusual manifestation of underlying breast cancer, causing a diagnostic clinical dilemma for dermatologists,3–5 surgeons 6 and histopathologists. 7 Melanoma of the nipple is very rare, Papachristou and colleagues 8 reported the first case study of fourteen patients with primary malignant melanoma. Other studies have used radiolabeled monoclonal antibodies and external photoscanning to differentiate from Paget's disease, 9 and the first case report of malignant melanoma of the nipple was recently reported in Japan. 10
Melanocytes are usually located along the basal layer of the epidermis and melanin pigment in a similar location. In melanoma the melanocytes are found at all levels of the epidermis and in some cases the dermis. 6 Full thickness biopsy including the dermis and epidermis and immunochemistry is essential to differentiate Paget's disease from melanoma. Immunochemistry staining of Paget's disease is positive for CK7, EMA, CEA and mucin whereas Melan-A, HMB-45 and protein S-100 are negative in Paget's disease but positive for melanoma. 7
The surgical treatment for Paget's disease depends on the type of underlying breast cancer and the size of the breast. If a large invasive cancer is present or extensive DCIS, a mastectomy and staging axillary surgery with or without immediate reconstruction is normally recommended. If the cancer is small and limited to the nipple-areola, complex breast-conserving surgery with en-bloc removal of nipple, areola and central ducts may be offered. Adjuvant treatment is an adjunct to surgery and depends on the type of cancer and staging. Radiotherapy is commonly offered after breast-conserving surgery; endocrine therapy and chemotherapy may be offered depending on the extent of the disease and prognostic factors.
Conclusion
Hyperpigmentation of the nipple secondary to Paget's disease is an unusual presentation of underlying breast cancer. It is a diagnostic dilemma as it is difficult to differentiate from cutaneous melanoma. Histopathology including immunohistochemical staining is essential for correct diagnosis. Surgery and adjuvant therapy depends on the type of cancer and stage of disease.
Footnotes
Acknowledgments
None