
Abstract
Objectives
To describe the epidemiology of end stage renal disease (ESRD).
Design
Mixed-methods systematic review.
Setting
The countries of the Gulf Cooperation Council (GCC) which consist of Saudi Arabia, the United Arab Emirates, Kuwait, Qatar, Bahrain, and Oman.
Participants
Defined to have ESRD or patients on regular dialysis for a minimum dialysis period of at least three months. Since many outcomes were reviewed, studies that estimated the incidence and prevalence of ESRD as outcomes should not have defined the study population as ESRD population or patients on regular dialysis. Studies where the study population mainly comprised children or pregnant woman were excluded.
Main outcome measures
The trends of the incidence, prevalence, and mortality rate of ESRD; also, causes of mortality, primary causes and co-morbid conditions associated with ESRD.
Results
44 studies included in this review show that the incidence of ESRD has increased while the prevalence and mortality rate of ESRD in the GCC has not been reported sufficiently. The leading primary causes of ESRD recorded in the countries of the GCC is diabetes with the most prevalent co-morbid conditions being Hypertension and Hepatitis C Virus infection; the most common cause of death was cardiovascular disease and sepsis.
Conclusions
This review highlights that the lack of national renal registries data is a critical issue in the countries of the GCC. The available data also do not provide an accurate and updated estimate for relevant outcomes. Additionally, considering the increasing burden of chronic kidney disease (CKD), these results stressed the needs and the importance of preventative strategies for leading causes of ESRD. Furthermore, more studies are needed to describe the epidemiology of ESRD and for assessing the overall quality of renal care.
DECLARATIONS
None declared
Amal Hassanien is funded by a scholarship from Ministry of Higher Education in Saudi Arabia
Not applicable
AH
AH designed and coordinated the study, conducted a systematic review and statistical analysis; and drafted the manuscript. AM contributed to the design and coordination of the study and reviewed the manuscript EV contributed to the design of the study and reviewed the manuscript GY contributed to statistical analysis, and reviewed the manuscript FA conducted a systematic review and reviewed the manuscript
Muhammad Shahid
Introduction
End-stage renal disease (ESRD) is defined as irreversible decline in kidney function, when renal replacement therapy (RRT) is needed for survival. There are two main types of RRT: dialysis and kidney transplantation. 1 Kidney transplantation is preferred for patients with ESRD since it offers a longer life span, superior quality of life, and is more cost effective than long-term dialysis. 2 ESRD has become a public health concern worldwide, with recent reports showing that the total number of ESRD patients has been growing dramatically 3 8 The rising prevalence is due largely to two main factors; the ageing of the population and the global epidemic of diabetes. 3
The countries of the Gulf Cooperation Council (GCC), which consist of Saudi Arabia, the United Arab Emirates, Kuwait, Qatar, Bahrain, and Oman, share a similar background of culture and ethnicity, while their Sociodemographic distributions and socioeconomic development are also similar. 4 Although the countries of the GCC have experienced noticeable advances in delivering healthcare, the burden of non-communicable diseases is increasing rapidly. 5 Many reports have shown evidence of increasing prevalence of the most common causes of ESRD in the GCC: the prevalence of obesity in these countries, which is associated with multi-chronic diseases, exceeds that in the developed countries because of their rapid economic growth and associated changes in lifestyle. 6 8 Furthermore, the International Diabetes Federation reports that five of the countries of the GCC ranked globally among the top ten countries in the world for diabetes prevalence. 9
The growing incidence of ESRD is increasing the use of RRT, as well as generating greater morbidity, and more hospitalizations. These in turn increase healthcare expenditures, placing a heavy financial burden on healthcare providers and general populations to meet the growing needs of patients with ESRD.10,11 However, ESRD has a significant effect on public health in the countries of the GCC, as the policy of these countries provides free health services including RRT to the population based on clinical need without any restrictions in terms of age, gender, or social status. Because the majority of RRT facilities are provided by the governmental sector, any increase in its use would be associated with a significant increase of healthcare expenditures.
ESRD also has a significant effect on quality of life and life expectancy. 12 Most patients receive haemodialysis treatment for ESRD by being connected three times per week to a dialysis machine for several hours at a time. People with ESRD are more likely than those without the illness to develop cardiovascular disease, the most common cause of death in those with ESRD. 13
Scarce data is available on the epidemiology of ESRD in the countries of the GCC. In the absence of national renal registries system in these countries, data that do exist are unsatisfactory and insufficient: most data are either recorded by referring centres rather than community hospitals such as Saudi Centre for Organ Transplantation (SCOT) data; or based on small studies. However, analyses of the epidemiology of ESRD itself in this region are also inconsistent. For example, the prevalence of ESRD decreased between 1986 and 2005, a period when risk factors for the disease became more common; this might be due to underreporting the cases of ESRD14,15 or might be influenced by mortality and renal transplant rate. Other articles report inconsistent results of primary causes of ESRD.11,16 These conflicting analyses of the epidemiology of ESRD mean that synthesizing and assessing the evidence available would be valuable.
This review was conducted to synthesize the results of all relevant studies to describe the epidemiology of ESRD in the countries of the GCC based on: incidence, prevalence, patient characteristics (age, sex, RRT), primary causes, co-morbidities associated with ESRD, mortality rate and causes of death in the ESRD population. This was done by indentifying and reviewing the published epidemiological studies of ESRD in the countries of the GCC.
Methods
Systematic review
A systematic review was conducted by searching Medline and EMBASE databases, to identify all relevant papers published from 1950 until May 2010; using the following keywords in the searching strategy:
End stage, terminal, chronic, renal, kidney, Arab, Middle East, Arabian Gulf, Saudi Arabia, Kuwait, and United Arab Emirates, Oman, Qatar, and Bahrain.
Additionally the reference lists of all identified papers were reviewed to identify other papers, which were not identified in the database search.
All the titles and abstracts of references were reviewed independently by two reviewers to identify relevant papers. Then, the full texts of the papers were reviewed to identify epidemiological studies that fulfilled the following criteria: any observational epidemiological study including cohort studies, case control studies, cross-sectional studies, and ecological studies; reporting ESRD incidence, prevalence, primary causes, co-morbidities conditions, mortality rate/causes were included in this review. In addition, all the studies have been defined by the study population to have ESRD or involve patients on regular dialysis for a minimum dialysis period of at least three months in any of the countries of the GCC. Since many outcomes were reviewed in this systematic review, studies that estimated the incidence and prevalence of ESRD as outcomes should not have defined the study population as ESRD population or patients on regular dialysis. Studies where the study population mainly comprised children, or pregnant woman, or patients on regular dialysis without mentioning the dialysis period or a period less than three months were excluded. In addition, the studies that do not report any statistical information about any relevant outcomes were excluded.
Studies that met the inclusion criteria for the review had data extracted. Data relating to study design, setting, definition of outcomes measure, inclusion and exclusion criteria of study population, methodological quality using the Newcastle Ottawa Scale (NOS) 17 and outcomes were then independently extracted by two reviewers using standardized data extraction form. In methodological quality assessment NOS, the included studies were classified after aggregating the score as follows: scores of seven or higher were chosen to indicate higher methodological quality, a score less than seven indicates a lower methodological quality.
Some outcomes such as primary causes and co-morbidities were classified as follows: primary causes of ESRD were classified as in the ICD9-CM code, which was updated in 2008 because there were no studies in this review used standardized methods to classify the primary causes. Co-morbidities associated with ESRD were classified into three groups: chronic diseases, infectious diseases, and other co-morbidities.
Data analysis
The extracted data for patients’ characteristics, prevalence, incidence, and mortality rate of ESRD were analyzed descriptively. The data related to primary causes, co-morbidities, and causes of death were entered to STATA version 10 for statistical analysis. These data were then used to conduct meta-analysis to summarize the prevalence of each outcome where possible. The degree of heterogeneity was assessed between the studies statistically using meta-analysis to obtain an I-square value. 18 This review combined the results from observational studies, therefore it would be expected that the value of I-square would be high due to sampling, methodological and statistical variation of the studies. To account for the anticipated heterogeneity, the random effect method was used to combine the measure of effect (DerSimonian and Laird model). Subgroup analysis was performed when it was needed to investigate the reasons for heterogeneity between the studies; it was used to assess the differences between locations and time. Furthermore, the measures of uncertainty (95% confidence intervals (CIs) were calculated where meta-analysis was not appropriate to conduct for any outcome especially for those that reported in less than three studies.
Results
Summary of excluded studies
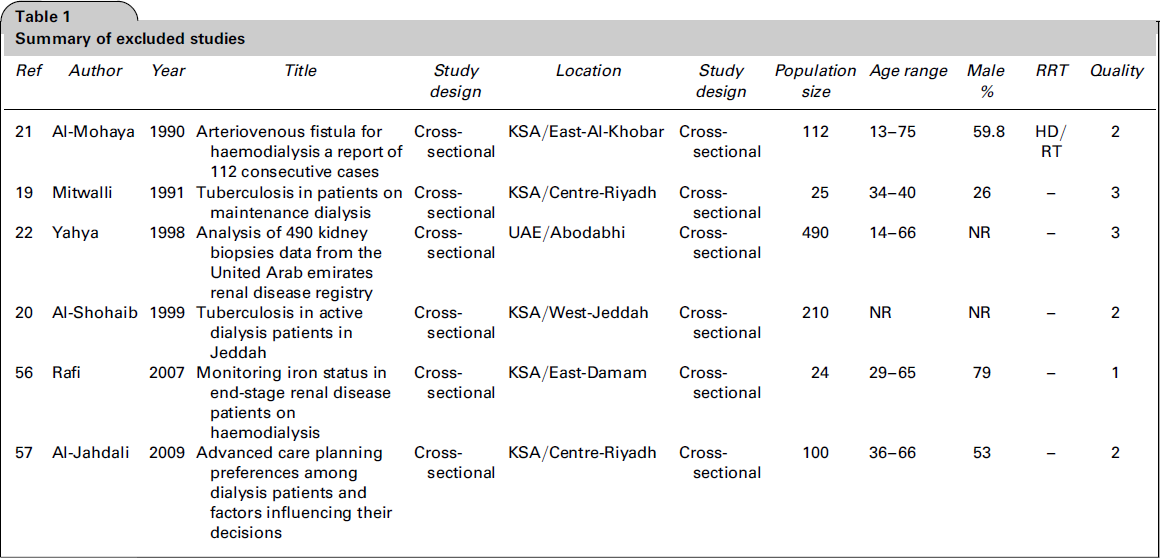
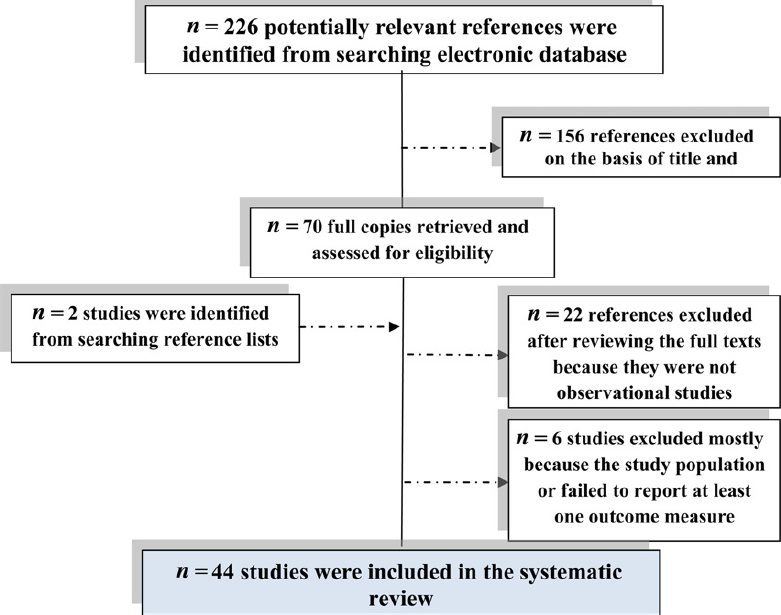
Flow chart shows a summary of the systematic literature review
Characteristics of included studies
Summary of included studies

Epidemiology of ESRD in the GCC countries
Patient's characteristics
The mean age of participants with ESRD in included studies ranged between 33 and 61.9 years some studies included children (aged >18 years old) but in very small proportion compared to adults, and three studies reported neither the age range of the study population nor mean age. 34 36 In the United Arab Emirates, the highest incidence rate of ESRD was reported in Abu-Dhabi city among the 45-55 years age group, 23 while in Kuwait the median of age among ESRD patients was 45 years. 24 In Saudi Arabia, incidence and prevalence of ESRD are linked directly to increasing age.19,37 One study conducted in Asir province found that the incidence rate of ESRD is proportional directly to increasing age as follows: the incidence rate of the patients who were aged between 15-44 years is 199.8 pmp, 45-64 years is 577.7 pmp, and >65 years is 716 pmp. 26 The proportion of males for all included studies was slightly higher than females in most included studies. Only four included studies did not report the proportion of male to female study participants. The study population was defined as haemodialysis patients in 24 included studies, and other studies reported the proportion of haemodialysis patients ranged between 52.1% and 97.8%. In two studies, the study population was defined as peritoneal dialysis, while other studies reported the proportion of peritoneal dialysis ranged between 1.2% and 29.1%. Only five studies reported the proportion of renal transplant ranged between 3.7% and 47.9%. (Table 2)
Incidence, prevalence, and mortality rates of ESRD
Summary of reported incidence rate

The mean of annual growth rate
This estimation based on single study per 100 population
Summary of reported prevalence

Prevalence of ESRD among diabetic patients NR = not reported
Summary of reported mortality rate

Annual death rate
Primary causes of ESRD
meta-analysis showed that the summarized estimate of diabetic nephropathy (DN) prevalence as a cause of ESRD is 17.27% (95% CIs, 11.38-26.21%; 21 studies)30,31,33,39,44-54 and there is no heterogeneity between the studies (I-square = zero%). Subgroup analysis by location shows that the summarized estimate of DN prevalence appears to be higher in urban or more developed areas than rural areas. For instance, in Saudi Arabia the summarized estimate of DN prevalence is 31.41%; (95% CIs, 7.39-133.59; 5 studies)39,44,53,55 in the western region, 29.15% (95% CIs, 9.21-92.24; 5 studies)43,48,51,56,57 in the eastern region, and 24.98% (95% CIs, 7.01-88.98; 5 studies)42,45,47,58 in the central region, compared to 6% (95% CIs, 2-17.8; 3 studies)36,37,44 in the southern region, which is considered a less developed area. These differences between the areas are not statistically significant (P-value = 0.32). Subgroup analysis by period of time shows that the summarized estimate of DN prevalence had significantly increased from 12.38% (95% CIs, 7.38-20.74; 9 studies)30,31,37,44-46,48,53,58 in the period 1990-1999 to 32.26 (95% CIs, 15.90-65.46; 11 studies)33,36,39,42,43,47,51,54-57 in the period 2000-2010 with (P-value = 0.03).
The summarized estimate of glomerulonephritis prevalence as a cause of ESRD is 12.68% (95% CIs, 8.59-18.70; 21 studies)30,31,33,36,37,39,42-48,51,53-59 and there is no heterogeneity between the studies (I-square = zero%). Subgroup analysis by locations in Saudi Arabia demonstrate that the highest estimate of glomerulonephritis (GN) prevalence found was in the eastern region (21.67% [95% CIs, 7.74-60.66; 6 studies),43,48,51,56,57,59 followed by the central region (8.25% [95% CIs, 3.69-18.45; 5 studies])42,45-47,58 western region (7.97% [95% CIs, 3.11-20.42; 5 studies])39,44,53-55 and southern region (7.10% [95% CIs, 2.14-23.56; 3 studies])36,37,44 These differences between the areas are not statistically significant (P-value = 0.39). Also, the heterogeneity in the period of time was explored and demonstrated that the summarized estimate of GN prevalence had declined from 18.82% (95% CIs, 9.65-36.69; 9 studies)30,31,37,44-46,48,53,58 in the period between 1990-1999 to 10.36% [95% CIs, 6.42-16.70; 11 studies] 23 34 in the period between 2000-2010. This difference between these two periods is not statistically significant (P-value = 0.15).
The summarized estimate of hypertensive nephropathy prevalence is 7.75% (95% CIs, 6.31-9.52; 17 studies)18,21,23-27,30,32-39 and there is no heterogeneity between the studies (I-square = zero%). Subgroup analysis by location shows that the highest estimate of hypertensive nephropathy prevalence was found in Saudi Arabia in the central region (20.08% [95% CIs, 6.12-65.89; 5 studies])24,25,36-38 followed by eastern region (10.56% [95% CIs, 1.80-61.77; 3 studies])26,27,30 western region (8.13% [95% CIs, 2.95-22.42; 5 studies])32-35,39 and southern region (4.39% [95% CIs, 1.58-12.1; 2 studies]) 21,35 These differences in the summarized estimates of hypertensive nephropathy prevalence between areas are not statistically significant (P value = 0.7). Also, there is no significant difference in the summarized estimate of hypertensive nephropathy prevalence in subgroup analysis by period of time, while the summarized estimate of hypertensive nephropathy prevalence is 7.06% (95% CIs, 3.29-15.16; 7 studies)18,21,35-39 in the period 1990-1999 and 7.81% (95% CIs, 6.31-9.52; 9 studies)23-27,30,32-34 in the period 2000-2010 with (P-value= 0.8).
Secondary glomerulonephritis/Vasculitis group includes haemolytic ureamic syndrome (HUS) and systematic Lupus erthematosus nephritis (SLE). The prevalence of HUS as a primary cause of ESRD reported at just 1.7% (95% CIs, -0.16-2.74) by one study conducted in Saudi Arabia in eastern region. 30 The summarized estimate of SLE prevalence is 3.61% (95% CIs, 1.88-6.93; 10 studies)18,24,25,28-31,36,39,40 and the heterogeneity between the studies is high (I-square = 89.2%).
Interstitial Nephritis/Pyelonephritis group including: interstitial nephritis, pyelonephritis, obstructive uropathy and analgesic abuse. The summarized estimate of interstitial nephritis prevalence is 3.87% (95% CIs, 2.38-6.31; 5 studies)23,25,30,35,40 with I-square = zero%; obstructive uropathy prevalence is 4.47% (95% CIs, 3.03-6.60; 12 studies)19,25,26,28,29,31,32,35-38,40 with I-square = zero%; pylonephritis prevalence is 7.45% (95% CIs, 4.81-11.56; 14 studies)18,19,21,24,28,29,31-33,35-39 with I-square = zero%. Analgesic abuse prevalence was reported in two studies; one study reported the prevalence at 1.8% (95% CIs, [-1.7-5.2] 31 and another study reported the prevalence at 2% (95% CIs, 0.1-4) 32
Cystic/Hereditary/Congenital diseases group includes polycystic kidney disease, medullar cystic disease and congenital/hereditary diseases. The summarized estimate of polycystic kidney disease prevalence is 4.81% (95% [CIs, 3.05-7.60; 8 studies])18,28-33,37 with I-square = zero%, and medullar cystic disease prevalence is 1.43% (95% CIs, 0.75-2.72; 3 studies)18,32,39 with I-square = zero%. While the summarized estimate of hereditary and congenital disease prevalence is 4.43% (95% CIs, 1.74-11.28; 8 studies)18,25,30,31,35,36,40 with I-square = 83.5%.
The miscellaneous conditions group included ESRD of uncertain aetiology, and other conditions, that are rarely reported as causes of ESRD, such as schistosomiasis, tuberculosis, sickle cell nephropathy and contrast nephropathy. In these conditions for which the aetiology is unknown, the summarized estimate is 19.59% (95% CIs, 11.23-34.17; 17 studies)18,21,23-26,28-30,32,33,35-40 with I-square = zero, while the summarized estimate for conditions that are rarely reported is 3.45 (95% CIs, 2.04-5.82; 4 studies)28,36-38 with I-square = zero%.
Co-morbidities associated with ESRD
The chronic disease group included diabetes, hypertension, cardiovascular and vascular disease. meta-analysis showed that the summarized estimate of diabetes prevalence is 47.85% (95% CIs, 17.47-131.05; 6 studies)20,23,24,41-43 with I-square = zero%, and hypertension prevalence is 77.88% (95% CIs, 39.76-152.52; 5 studies)20,23,24,43,44 with I-square = zero%. The summarized estimate of cardiovascular disease prevalence is 14.51% (95% CIs, 5.48-38.45; 6 studies)25,28,33-36 with I-square = 38.7%. One study reported the prevalence of vascular disease as a co-morbidity condition as 11.7% (95%CIs, 9.1-14.4) 33
Among the infectious disease group, the most reported and prevalent infectious disease in ESRD patients was hepatitis C virus (HCV), which is more prevalent among haemodialysis patients than among peritoneal dialysis patients. The summarized estimate of HCV prevalence is 48.31% (95% CIs, 29.16-80.04; 10 studies)29,32,34,37-43 with I-square = zero%, while hepatitis B virus infection 14.82% (95% CIs, 5.22-42.06; 3 studies)34,40,41 with I-square = zero%, and tuberculosis 6.80% (95% CIs, 4.34-10.67; 5 studies)34,44-47 with I-square = 13.3%. The prevalence of nasal carriage of staphylococcus aureus, which associated with vascular access related septicaemia, was reported as a co-morbidity condition in HD patients in only two studies conducted in Saudi Arabia in Al-Hafouf City; both reported the prevalence of nasal carriage of staphylococcus aureus as 38% (95% CIs, 7.03-205.41; 2 studies)48,49 with I-square = zero%. The incidence of peritonitis was reported in only one study as 0.62% among continuous ambulatory peritoneal dialysis patients, 50 while the prevalence is 4.7% (95% CIs, 2.6-6.8).
Other co-morbidities and complication groups included anaemia, bone disease, gastrointestinal abnormalities, liver disease, depression, malnutrition and restless leg syndrome. meta-analysis showed that the summarized estimate of liver disease prevalence is 12.74% (95% CIs, 6.71-24.2; 3 studies)28,33,34 with I-square = zero%. The prevalence of anaemia was reported in two studies in this review. One study conducted in Saudi Arabia in Riyadh City, reported the prevalence of anaemia as 47.5% (96% CIs, 35-60.1), 51 while another study reported the prevalence of anaemia for all the GCC countries to be 33.7% (95% CIs, 29.8-37.7) 33 Bone disease was reported in only two studies, both conducted in Saudi Arabia, and reported the prevalence to be 28.9% (95% CIs, 24-33.9) in Taief31,34 and 70.2% (95% CIs, 58.3-82.1) in Riyadh. 31 The prevalence of depression was reported in two studies. One study conducted in Saudi Arabia in Abha City, reported the prevalence of depression at 59.3% (95% CIs, 46.2-72.4); 52 while another study, which was conducted in Bahrain reported the prevalence of depression among men with ESRD as 48%, which is higher than the level reported among women 42%. 25 The prevalence of malnutrition, restless leg and gastrointestinal abnormalities were reported as 32% (95% CIs, 25.5-38.5), 50% (95% CIs, 40.8-59.2), and 90.7% (95% CIs, 83-98.5), respectively, in three different studies. 53 55
Causes of mortality in ESRD patients
meta-analysis showed that the summarized estimate of cardiovascular disease is 36.74 (95% CIs, 8.42-160.36; 6 studies)23,24,28-30,34 with I-square = zero%, while cerebrovascular disease is 3.68% (95% CIs, 1.25-10.83; 4 studies)24,28,30,34 with I-square = 14.8%. The summarized estimate of sepsis is 18.97% (95% CIs, 3.14-114.68; 3 studies)24,30,34 of the deaths in ESRD patients with I-square = zero%. Malfunction of dialysis access was reported only at one study as a cause of death in ESRD patients at 32% (95% CIs, 17-48) 29 Pulmonary disease (pulmonary infection and pulmonary embolizm), hepatic failure, gastrointestinal bleeding, and malignancy were all given as causes of death in ESRD patients, and death attributed to these causes ranged from 2.1 to 11%29,30,34
Discussion
This review gives an overview of the demographic distribution of ESRD patients in the countries of the GCC. It shows that the overall proportion of males with ESRD is slightly higher than females in most included studies, and the most prevalent age group is between 33 and 60 years old. This is because the proportion of males is higher than females in the general population in Saudi Arabia, where most of the included studies were conducted, while the middle age-group constitute the majority of the population, and the elderly people (those aged >65) constitute only 3%. 4 This clarifies why the proportion of elderly patients with ESRD was small in the included studies in this review.
The majority of ESRD patients in the GCC countries are on haemodialysis. Renal transplantation prevalence was reported in only five studies and ranged between 3.7% and 47.9%23,24,27,28,34 However, the most reliable data about renal transplantation in that area is provided by SCOT. This organization coordinates the medical care facilities offered to patients with ESRD and other organ failure; also, it is considered the national authority in laying down the general regulations which relate to all aspects of organ transplantation and brain death in the kingdom. The SCOT 2009 report shows that the number of kidneys transplanted from living donors is more than double the number of kidneys transplanted from deceased donors; the number of kidneys transplanted from living donors has been increasing markedly since 1979. Approximately 40% of ESRD patients had undergone renal transplantation by 2009. 68
The incidence, prevalence and mortality rate of ESRD in the GCC were not reported sufficiently in this review. All included studies reported the cumulative incidence rate, which does not show changes in the trend; except one study that reported the mean annual growth rate in Gizan was 7.44% in the period from 1987 until 2000. 27 However, two studies in this review that were conducted in Saudi Arabia in A1-Madinah city, show that the incidence rate had increased two-fold from 1988 to 2001.59,61 This implies that the incidence rate has been increasing gradually over time. Furthermore, mortality rate of ESRD in this review varied widely between studies across the region. That may relate to differing treatment practices which contribute to the variation in outcomes. In addition, it was difficult to track the trend of prevalence and mortality rate in this review because of gaps in the available data. However, SCOT data shows that the incidence rate of haemodialysis patients is increasing annually by 8%, 68 which may imply that the prevalence of ESRD is increasing without taking into account the kidney transplant and mortality rate.
The increasing size of the ESRD population who require RRT in the countries of the GCC might be due to multiple factors such as the rapid socioeconomic development in these countries in recent decades, which has resulted in changing lifestyle and nutrition habits. 8 This in turn plays a role in changing the trend of the prevalence of non-communicable disease such as diabetes, which is globally the leading cause of ESRD. 3 Many reports have provided evidence of increasing prevalence of the most common causes of ESRD in the GCC; such as obesity, hypertension, and diabetes.7,69,70 The prevalence of diabetes and hypertension is significantly higher in urban populations than rural populations and in men rather than women. This supports the finding in this review that the prevalence of diabetic nephropathy as a cause of ESRD is higher in urban areas than rural areas, but this finding was not statistically significant.
meta-analysis showed that the leading cause of ESRD in the GCC was diabetic nephropathy 17% followed by GN (13%) and hypertensive nephropathy (8%), while the prevalence of diabetic nephropathy had been increasing significantly over time. Furthermore, among all reported co-morbid conditions in this review, hypertension was the most prevalent chronic condition by 78%. In addition, infectious diseases were also prevalent co-morbid conditions, of which HCV was the most prevalent among ESRD by 48%, especially among haemodialysis patients; which might be due to frequent attendance of patients at dialysis centres spreading the disease through nosocomial infection 43 and the effect of nurse understaffing. 62 Other factors may increase the risk of HCV, such as the length of dialysis, or the number of blood transfusions; also diabetic patients and males are more likely to develop HCV35,44,48,71
Causes of mortality and hospitalization among ESRD patients usually result from infectious diseases or complications of dialysis, or chronic illness. Among all reported causes of death in ESRD populations in this review, approximately 37% of deaths were related to cardiovascular disease and 19% were related to sepsis. Two studies reported the causes of hospitalization. One study reported the majority cause of hospitalization was cardiovascular disease followed by vascular access related problems, while ischemic heart disease contributed to 19% of the total hospitalization. 28 Another study reported the main cause of hospitalization was vascular access related problems (34%). 63 However, one study suggested that the optimization of arteriovenous fistula (AVF) placement might be a preventative approach to reduce infections associated with vascular access problems, such as staphylococcus aureus infection, which can lead to septicaemia. 49 This suggestion is supported by the National Kidney Foundation's kidney disease outcomes quality initiative (K/DOQI) clinical practice guideline for vascular access, where AVF is the most preferable type for permanent vascular access for HD patients, which related to improved quality of life and increased life expectancy in HD patients. 72
In comparing this review with a similar publication that was undertaken for the countries of the Middle East, 73 which the countries of the GCC are a part, both highlighted that the incidence of ESRD is increasing substantially and that diabetes is a dominant cause of ESRD. These findings are similar to those reported in the USA and Europe, where diabetes was found to be the dominant cause of ESRD.74,75 This review indicates that hypertension is the commonest co-morbidity in ESRD population as in the SCOT report. 68 Furthermore, in comparing the findings of this review with the SCOT report, we found that the demographic distribution of age and sex in ESRD are similar. In addition, both show the prevalence of HCV as a co-morbidity to be high: approximately 48% in this review and 26% in the SCOT report, which are higher than those reported in Europe (12%) and the USA (7%). 76
The strengths of this review are firstly, it includes all of the epidemiological studies conducted in the GCC until 2010. Secondly, this review presents adequate and comprehensive information based on epidemiological studies for multiple outcomes related to ESRD. It provides evidence of the burden of ESRD and defines the high-risk groups; also, it records all co-morbidities and causes of death in ESRD patients in the GCC. This information is extremely valuable for public health planners and administrators to allocate healthcare resources in the countries of the GCC. Furthermore, it gives an overview regarding the sources and quality of the existing health data in the GCC.
Limitations of this review include gaps in the data which did not allow description of trends in the prevalence and mortality rate of ESRD. The majority of included studies in this review were concerned with the haemodialysis population, while there is no available data on either preemptive transplantation or elderly people receiving supportive care. In addition, it is prone to a selective bias in terms of excluding all of the patients who received dialysis for less than three months to exclude those patients with acute renal failure. This might result in excluding patients with ESRD who did not survive more than three months. Although this review provided an overview regarding the burden of ESRD in the countries of the GCC, it was not able to provide accurate and current estimates for each related outcome, and the majority of studies were given a low score in quality assessment because they were not well reported. For this reason, the lack of a national renal registry data in the countries of the GCC is a critical issue. Sufficient information is supposed to be recorded for each patient; such as demographic and clinical characteristics, RRT, vascular access, primary causes of ESRD, co-morbidity conditions, laboratory tests, medications, hospitalization, death event and its cause. Each outcome must be recorded by healthcare specialists according to standardized policy, especially in diagnostic procedures. 16 This registry will provide a reliable source of data for further related epidemiological research.
Nevertheless, this review has several important implications for policymakers and public health planners. It provides evidence of the rise in the trend and burden of ESRD in the countries of the GCC; this helps to enable the prediction of healthcare trends. Furthermore, it defined high-risk groups in the GCC population, who were patients with diabetes; this emphasizes the importance of developing potential preventative strategies such as screening programs to detect and manage diabetes and chronic kidney disease (CKD) in early stages and slow down their progression; those programs may be more cost-effective in the future.3,77 In fact, the quality of care and management should be a target for healthcare providers to improve the quality of life and life expectancy, since hypertension and HCV have become prevalent among ESRD patients and may lead to increased costs of healthcare, because patients with comorbidities require more hospitalization and medications. In addition, investigating causes of death in patients with ESRD may help to draw the attention of healthcare professionals to specific health issues which can lead to improved healthcare services in that area. This may increase the quality of life and life expectancy of ESRD patients.
Conclusion
This is the first systematic review of the epidemiology of ESRD that has been undertaken in the countries of the GCC. There were several methodological challenges that could not be overcome; however, it was possible to construct a framework of the epidemiology of ESRD in the countries of the GCC. This review presents an overview of the increasing burden of ESRD in the GCC countries, which is similar to the rest of the world. It also provides a list of the major causes of ESRD in these countries and the most frequent morbidities associated with ESRD. Accordingly, this review suggested that the dominant cause of ESRD in the GCC was diabetic nephropathy; and the most frequent co-morbidities were hypertension and HCV. It highlights the emphasis on the need of national renal registry data as a crucial issue and preventative strategies, such as screening programs for the primary causes of ESRD and CKD. Finally, we recommend further epidemiological studies to describe the pattern of the disease in the area and to improve the overall quality of renal care management.
Footnotes
Acknowledgements
The Department of Primary Care & Public Health at Imperial College London is grateful for support from the NIHR Collaboration for Leadership in Applied Health Research & Care (CLAHRC) Scheme, the NIHR Biomedical Research Centre scheme, and the Imperial Centre for Patient Safety and Service Quality