
Abstract
Objectives
There is little research into the constituents of effective psychiatric inpatient care. The aim of this study was to assess the effectiveness of a newly adopted model of inpatient care; the acute assessment ward.
Design
Review of data collected over a year-long period.
Setting
Acute assessment ward in North London.
Participants
All Admissions between 8 October 2009 and 7 October 2010.
Main outcome measures
Duration of stay, need for readmission, patient satisfaction and frequency of conflict behaviours.
Results
A total of 485 admissions over the yearlong study period. The median stay to discharge from the assessment ward was 6 days, whereas in those transferred it was 19 days. Readmission within 28 days following discharge from the assessment ward was 13.9%, whereas those discharged from other wards was 9.2% (P = 0.1). Patient satisfaction was no lower, for all domains, than for other wards in the trust. Frequency of conflict behaviour was equal to previous studies, 1 but self harm was significantly less common (P = 0.01).
Conclusions
Our data show that focusing on the ‘point of entry’ to inpatient services means that some admission times can be reduced without an increase in 28-day readmission rates or conflict behaviours. The acute assessment model attempts to address the need for the NHS to deliver more for less, whilst remaining focused on service-user and staff satisfaction. Research into which areas of this complex intervention are effective is challenging, but we would urge others who run services with novel structures to publish data about their functioning.
DECLARATION
All of the authors are employed by Camden and Islington NHS Foundation Trust
No funding or sponsorship was received
Ethical approval was not required for this study. All data were anonymized before being accessed by the authors. The study only includes data collected by the NHS Foundation Trust as standard. Patients are not identifiable
Apu Chakraborty
JH, RG, FO, ST and AC devised the study. JH and RG collected and analyzed the data. JH, RG, FO, ST and AC wrote the paper
Andrea Livingstone and Gerard Leavy
Introduction
Despite the drive to ‘care in the community’ 2 , with a decrease in the number of psychiatric beds 3 and an increase in funding to community teams, 4 inpatient care remains an essential component of mental health services. Inpatient wards play a major part in supporting people during times of crisis, relapse and ill health. 5 Over time, there has been increased success in avoiding admissions to hospital through improved community-based services. 6 Over recent years, community mental health teams have evolved and functional teams (early intervention, assertive outreach, crisis resolution and home treatment teams) have developed. 7 However, when people do need to go into hospital, it is essential that the services provided offer the very best care and treatment from a highly skilled and experienced workforce.
The number of inpatient psychiatric beds nationally has been reducing from a peak in 1955 of around 150,000. 8 In 2000 34,214 beds existed, and this has now reduced to 25,563. 9 This trend is unlikely to be reversed in the near future because of the current economic climate and, where as previously there was a transfer of funding from inpatient to community settings, there are also likely to be changes to other service areas because of funding cuts.
Mental Health Trusts therefore need to be innovative in the way they provide care. This is especially true of inpatient services, but there is little quality evidence available with regards to what is effective. There has been recent work looking at alternatives to traditional inpatient care, 10 which has been driven by service user and stake holder wishes to improve the experience of an inpatient stay. However, the evidence was not compelling enough that alternatives should be seen as essential in every catchment area, and many types of alternative may not be suitable for patients who are severely unwell. 11 Further research into acute inpatients services is clearly needed, but there are multiple challenges in evaluating such a complex intervention. 12 Guidance from the Department of Health 13 concentrates on improving services rather than considering service innovation as a means of solving problems, but it has been recognized that there is a need to develop new ways of delivering acute inpatient care, as well as making it more efficient.
This study reviews the success of a trust in North London in developing an acute assessment ward as a new way of delivering inpatient care. The ward has now functioned for one year. The model is similar to that adopted by the triage ward in Lewisham 14 and others around the country. However, the authors are not aware of any detailed patient outcomes that have been published from similar inpatient care models.
It was hypothesized that the ward was facilitating earlier discharge for some patients, with no increase in readmission or serious untoward incidents. We recorded clinical outcome data; route to admission, duration of inpatient stay, ICD-10 diagnosis, need for readmission within 28 days, and bed occupancy over the course of a year. During this time, patients were invited to complete an anonymous satisfaction survey. We also recorded the frequency of conflict behaviour over a three month period.
Setting
The London Borough of Camden is an area in the north of the City, reaching from Holborn and Bloomsbury in the south, to Hampstead Heath in the North. The 2001 census gave Camden a population of 202,600. Camden is 73% white, 6% Bangladeshi and 6% African. A total of 35% of householders are owner-occupiers; and 86% of households live in purpose-built or converted flats. 15 The borough is home to some of London's most affluent areas, such as Hampstead, Dartmouth Park, and Primrose Hill, as well as areas of high unemployment, social deprivation, and high crime levels (especially drug crime) around Haverstock, Somers Town and, to a lesser extent, Kentish Town and Camden Town. This gives rise to the ‘two Camdens’ Syndrome, 16 which is signified by a wide Jarman Index across the borough, 17 and an apparent inequity in access to education and healthcare in its constituencies.
North Camden inpatient services are provided at The Grove Centre, on the site of the Royal Free Hospital. The unit has 44 beds, which are split between two treatment wards (Fleet and Isis) and the acute assessment ward (Solent).
New model
There are 16 assessment beds on Solent ward. Vigorous efforts are made by the inpatient team to discharge patients where possible within a brief period. Key features of the Solent ward model are:
Medical input
The medical input consists of one whole-time equivalent consultant, a higher trainee and two core trainees. There is a consultant lead ward round every weekday morning. Senior medical staff are involved at the time of admission, and all patients will normally have senior input within 24 hours of admission (excluding weekends). Treatment can therefore be initiated at an early stage, potentially decreasing the duration of inpatient stay. Should a longer period of inpatient treatment be necessary, the patient will be transferred to one of the treatment wards. All patients have easy access to information about medication and treatment plans, and the level of medical cover means that any concerns the patient has, can be addressed in a timely manner.
A ‘whole-system approach’ to inpatient care
Essential to the model is the recognition that there are alternatives to inpatient care and to facilitate this a ‘whole system approach’ has been adopted; working closely with other wards, the Camden Crisis and Response team (who have access to Crisis House beds) and Community Mental Health Teams.
Multi-disciplinary team working
Each patient will be discussed on a daily basis, by all members of the clinical team, with regular updates to care plans and timely management interventions. Patients have dedicated time with a named staff member and there is input from a social worker, occupational therapist and housing support officer. Discharge planning is commenced as soon as a patient is admitted to the ward.
Positive ward environment
The ward was specifically designed to provide care for inpatients with awareness of patient and staff needs. Male and female areas are separate to preserve dignity and privacy. All patients have their own rooms with en suite toilet and shower facilities. Unit based occupational therapy facilities include a gym, computer room, art room and small library
Method
Data were collected over a number of domains for a period of one year (8 October 20t09–7 October 2010) including basic demographic data, route to admission, diagnosis (checked using the operational criteria OPCRIT checklist for psychotic and affective illness 18 ), Mental Health Act status, duration of inpatient stay, readmission, and need for transfer to longer stay wards. During this study period patients were invited to complete a satisfaction survey, which was completed anonymously on the ward by computer 19 (this survey was not carried out by the authors). Over a three month period (12 February 2010–12 May 2010), measures of conflict behaviours (verbal aggression, aggression to objects, physical assault, self harm) were recorded on a shift by shift basis, with the aim of comparing the frequency of adverse events with those found in the City 128 Study 1 of 136 acute psychiatric wards in the UK. Sadly, because of time constraints, recording of conflict behaviours could not be sustained for the full study period of one year.
Results
Four hundred and eighty-five patients were admitted within the twelve month period, 315 males and 170 females, mean age 40.5 years (standard deviation 12.8). Of these, 67.2% were of white background, 62.5% were informal patients (see Table 1). Bed occupancy was 70.9% over the yearlong period of study. Furthermore, 58.6% of admissions were via Emergency Departments (which, in the area, are used as ‘places of safety’ under the Mental Health Act). Only 12.6% of admissions were ‘planned’, that is, directly referred from the patient's community team. A total of 185 patients (38.1%) were from outside Camden.
Demographic characteristics and route of entry

With regards to patient stay on the assessment ward; 158 patients were discharged directly from the ward, back into the community. The remaining 327 were transferred to other psychiatric wards including the Crisis House (15 patients were transferred from Solent to the Crisis House, another ten were transferred from other wards to the Crisis House). Those discharged directly from the ward had a median stay of 6 days (range 0–49). Those transferred to another psychiatric ward had a median total inpatient stay of 19 days (range 2–349). Fifty-two patients were identified who were readmitted within 28 days of their discharge date (from Solent ward or another psychiatric ward). Twenty-two patients (13.9%) were discharged from Solent ward to the community and readmitted (to any inpatient psychiatric unit, within 28 days), 30 patients (9.2%) who were discharged from other wards were readmitted. Using Fisher's exact test, this difference was found not to be statistically significant (P = 0.1194).
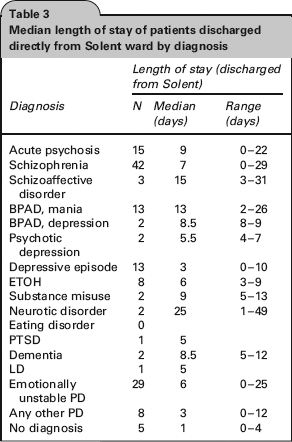
Diagnosis of all patients is shown in Table 2. Paranoid Schizophrenia was the most common diagnosis (33.2%) and the majority of patients admitted (59.4%) had a psychotic illness (schizophrenia, acute psychosis, schizoaffective disorder, psychotic depression, or mania with psychotic symptoms). Median length of stay for all patients discharge directly from the ward by diagnosis is shown in Table 3.
Clinical diagnosis

Median length of stay of patients discharged directly from Solent ward by diagnosis
During the study period, 211 patients completed the electronic satisfaction survey. 19 90.9% described the care provided on their current admission as very good or excellent. Comparison with average scores for seven other general adult wards in Camden and Islington NHS foundation trust which are not using this model, is shown in Table 4.
Patient satisfaction

Over a three month period, measures of conflict behavior were recorded: verbal aggression occurred at a frequency of 1.89 events per day; aggression to objects 0.51 per day; physical assault 0.39 per day; and self harm 0.06 per day. These measures are shown in Figure 1.

Frequency of conflict behaviour – comparison with City 128 study
Discussion
Principal findings and possible mechanisms
Admission to inpatient services will, for many patients, be first point of contact with psychiatric services and it is rare that this happens in a planned manner (only 12.6% of our sample were ‘planned admissions’). Restricted bed numbers and funding cuts mean that it is increasingly important that the process of admission and patient movement through the inpatient system is as efficient and effective as possible. As well as this, the system should respect the autonomy dignity and individual needs of the population it serves. We have collected data from a North London acute assessment ward, developed in an attempt to meet these challenges. The main differences in terms of ward set-up are thought to be daily consultant lead ward rounds and a strong multidisciplinary approach to patient care.
The ward managed 485 admissions over the year-long period of study. The median length of stay on the Solent ward for patients that were directly discharged to the community was one-third of that in the transferred group. It is possible that if a greater percentage were transferred, or were on wards with less intensive medical management, their stays would have been longer. It was shown that 10.7% of patients were readmitted within 28 days. When readmission is used as a quality outcome measure for inpatient psychiatric programs, below 15% is generally quoted as an acceptable 28-day readmission rate.20,21 There was no statistically significant difference in readmission rates between wards, which suggested that rapid discharge from Solent ward does not increase readmission rates beyond those expected. However, it must be recognized that this relies on the appropriate selection of patients for discharge or transfer, and studies in the past have shown that the ‘gain’ of a shorter initial inpatient stay per stay does not always result in shorter cumulative hospitalization.22,23
Overall, inpatient stays were reduced by access to the Crisis House. Patients were discharged from Solent ward that would have required longer on the ward or transfer to intermediate stay wards. Alternative options for psychiatric care, such as crisis houses, have been shown to improve patient satisfaction and cost-effectiveness, 11 and it may be that there are specific advantages to this kind of alternative when they are run in conjunction with an acute admissions ward such as Solent. Crisis Teams also facilitate the functioning of the model, working closely with both community and inpatient services (straddling the gap which previously existed), acting as gatekeepers to inpatient care, and facilitating early discharge. It is only through all of these elements working effectively together that the system can function.
The study showed that 38.1% of patients in the survey were from outside the borough of Camden; this makes information gathering a challenge, slowing care planning and discharge. This includes patients who would have to be found accommodation in the local area (no fixed abode), and those who require relocation. Data from the whole of Camden and Islington NHS foundation trust suggest these patients have a median stay of 11 days and around 30% end up in accommodation locally. It is not infrequent that foreign nationals requiring repatriation are admitted, and coordination of this can be both costly and time consuming.
The majority of patients in our sample were admitted on an informal basis. This is comparable with the ‘Count Me In’ census from 2009, 24 which found that 47% of inpatients were detained under the Mental Health Act. With a continuing trend of fewer inpatient beds, the proportion of detained patients is likely to increase, and the threshold for admission rise. Keown, Scott and Mercer 25 found that between 1996 and 2006 the number of involuntary admissions per annum increased by 20%. They also found that overall yearly admissions declined by 11%, but that this reduction was limited to three subpopulations: learning disability, unipolar depression, and dementia. Therefore the inpatient case mix has shifted further towards psychotic and substance misuse disorders and Solent ward's milieu; 59.4% psychotic illness, 4.5% drug and alcohol misuse disorders is likely to be typical of inpatient units throughout the county.
The results of the satisfaction survey suggest that patients are generally more satisfied with the acute admissions ward, than with other general adult wards in the Trust. Understandably there was a limited response to the survey and patients completing it are self-selecting. This data is therefore of limited quality and no statistical analysis has been possible, but we feel it is important to note that at the time of highest stress for patients (initial admission to inpatient services), they do not rate the quality of care they receive poorly. It has been suggested that satisfaction is strictly linked to effectiveness of care provided, whereas dissatisfaction is frequently the reason behind patients’ discontinuing contact with psychiatric services.26,27
The data collected on conflict behaviour suggest that incidence of verbal aggression, aggression to objects and physical assault were not significantly different to those for all acute wards involved in the City 128 study. 1 An unpaired t-test was used to compare Solent ward and the City 128 Study data. It showed a significantly lower incidence of self harm on Solent ward (P = 0.0104). There was no statistically significant difference for any of the other measures of conflict behavior in Figure 1 (verbal aggression P = 1.0000, aggression to objects P = 0.1490, physical assault P = 1.395). Before Solent ward was created, there was concern that a ward established to manage the most acutely unwell patients, directly from the community, would result in higher untoward incidents, however this has not been the case. There were no incidents of suicide throughout the study period. We found this to be a particularly striking and encouraging finding with broad ramifications.
The intervention which occurs at the point of entry to inpatient services is clearly a complex one. It is likely that it has the power, if conducted correctly, to alter a patient's long-term engagement with services for the positive. It is vital therefore that every effort is made to optimize this experience; discharging patients to their homes efficiently and safely in a timely manner is central to this. Although controversial, it is possible that a shorter stay in hospital may be beneficial for some patients; brief containment during a crisis could be what is needed to start recovery, and retain dignity and authority over their lives.
Strengths and weaknesses
Sadly we were unable to gather complete before and after data for the change in ward structure which may have provided stronger evidence for the effectiveness of the model. As such, it could be argued that we are not comparing like with like when looking at Solent ward vs. all other treatment wards. Whilst this may be true for duration of stay, this is not necessarily the case given our key outcomes are readmission rate and incidence of conflict behaviours. There is very little pre-existing research in this area to make comparisons with, and any evidenced-based assessment of inpatient psychiatry is always going to be complex.
Unanswered questions
Research into which elements of inpatient care are key to effectiveness is still needed. A useful interim however, may be wards such as Solent highlighting the central tenets of their care model and reporting their outcomes. Hopefully this will prompt discussion and debate about this crucial area of the mental health service.
Footnotes
Acknowledgments
Not applicable