
Abstract
Objectives
Statins are a well-known primary and secondary prevention drug for cardiovascular disease and NICE guidelines have been issued to identify key indicators for their use. An audit looking into statin prescribing for medical inpatients was carried out in two geographically distinct London hospitals.
Design
A prospective inpatient audit of medical prescription charts was performed. Blood results were reviewed for the inpatients during their admission to identify any contraindications for statin usage (rhabdomyolysis). The medical notes were also reviewed for patient refusal of statin therapy.
Setting
The study was carried out at two distinct hospitals in London. Whipps Cross University Hospital (WCUH) and Chelsea & Westminster Hospital (CWH) are located in East London and West London, respectively. Acute medical, surgical, obstetrics and gynaecology, paediatric and palliative wards were excluded.
Participants
A total of 309 inpatient medical notes and prescription chart data were collected from WCUH (n = 211) and CWH (n = 98).
Main outcome measures
High percentage of hospitalized patients are not prescribed statins despite clear clinical indications for their use. Regardless of geographical and socioeconomic factors between hospitals, statin prescribing remains suboptimal.
Results
The patient demographics in both hospitals were very similar; the mean age at WCUH was 78 ± 15 1SD while at CWH the mean age was 74± 15 1SD. The results showed that approximately one-third of patients (30% at WCUH and 33% at CWH) had at least one indication for statin therapy according to NICE guidelines and yet they were not prescribed a statin. Ten percent of patients at WCUH and 13% of patients at CWH had ischaemic heart disease (IHD) and yet were not prescribed statins.
Conclusion
Statin prescription is often overlooked in secondary care with patients being discharged without the appropriate assessment (NICE guidelines), which subsequently means repeat prescriptions are not provided by the GP. This study is the first to show that this problem is not due to resources or geography, but is inherent within the NHS system. Consequently, a revised prescription chart checking system has been suggested for pharmacists and junior doctors.
DECLARATIONS
None declared
None
Obtained in accordance with the ethics/audit committee of Whipps Cross University Hospital, and Chelsea and Westminster Hospital; confidentiality regarding all patient notes was maintained throughout and there was no breach of confidentiality during data handling and processing; all data were encrypted
RS
All authors contributed equally
The authors thank Peter Mills for his guidance and support
Honer Kadr
Introduction
Coronary heart disease (CHD) is the most common cause of death in the UK, with around 94,000 deaths annually. 1 The underlying pathology of CHD is the progression of atherosclerosis,2,3 for which one of the main risk factors is hypercholestrolaemia.4,5 Statins are used to lower LDL levels, through the inhibition of the rate-determining step of cholesterol synthesis in the liver. 6 Numerous trials have proven that secondary prevention with statins considerably improves mortality and morbidity. 7 In addition, primary prevention strategies for cardiovascular disease (CVD) lead to significant risk reductions; 12% in all cause mortality, 30% in major coronary events, and 19% in major cerebrovascular events. 8
The social and economic burden of CVD is an ever more serious problem with the increasing prevalence of adverse lifestyle practices and the ageing UK population. The National Institute for Health and Clinical Excellence (NICE) has identified this problem and issued clinical guidelines for the use of statins in primary and secondary prevention. Adults with a history of CVD are automatically recommended for statin prescription and adults with a 10-year risk of developing CVD equal to or greater than 20% should start statin therapy as primary prevention.
The effective adherence to clinical guidelines is crucial in improving patient outcomes as it defines a standard practice across the nation using the latest evidence. 9 This benchmark standardization provides cost efficiency and efficacy especially in preventative medicine, where a rigorous systematic approach to drug prescription is necessary for clinical outcomes. In addition, if hospitals initiate changes to a patient's primary management, then this is often continued into primary care. 10
The report that governs the NICE guidelines has identified a large number of significant risk factors for CHD for which statins have been found to reduce the risk of these events (Table 1).

Since the guidelines have been announced, there has been no published data highlighting the prescribing patterns of statins in the UK. This audit, using current NICE guidelines, is a cross-sectional prospective study that identified the prescribing levels of statins in two geographically distinct regions within London. A city-wide study was necessary to provide an accurate sample to be analysed, so that valid conclusions could be obtained on statin prescription.
The regions considered include a relatively deprived area covered by WCUH and a more affluent area covered by CWH. Previous studies have highlighted the relationship between socioeconomic status and prescribing habits; people living in more affluent areas have higher rates of statin prescription compared to those in deprived areas. 11
It was envisaged that the advent of NICE guidelines would enforce correct statin therapy, especially in high-risk patients such as those with a history of CVD. This study aims to assess the level of statin prescribing in accordance to NICE guidelines.
Methods
All inpatient medical notes and prescription chart data were collected from two hospitals of distinct geographical location: WCUH and CWH. Blood results were reviewed during inpatient stay to exclude any contraindications for statin usage, such as rhabdomyolysis. The medical notes were also reviewed for patient refusal of statin therapy.
Inclusion and exclusion criteria
Patients admitted under the medical specialties, such as cardiology, gastroenterology, renal, respiratory, stroke, infectious disease and elderly care medicine were included in this audit. Patients from acute medical wards (Medical Assessment Unit, Accident and Emergency) were excluded due to the high rate of patient turnover while other wards (Obstetrics and Gynaecology, Paediatrics, Surgery, Palliative Care) were excluded as we felt the patient groups were not appropriate targets for statin usage.
Twelve CVD risk factors specified in the NICE guidelines were considered in this study as an indication for statin prescription. These were: hypercholesteraemia, hypertension, ischaemic heart disease, acute coronary syndrome (ACS), angina, myocardial infarction (MI), diabetes mellitus (DM), chronic cardiac failure (CCF), peripheral vascular disease, coronary artery bypass graft (CABG), cerebral vascular accident, transient ischaemic attack (TIA). 7
Data were collected by a different team located at each centre, and then both sets of data were inserted into an electronic database by another team. The database was verified by senior cardiologists to ensure that the indications for statin usage were indeed present (as advised by the NICE guidelines). After the verification process was complete, the dataset was redistributed to the data anlaysis team. The teams consisted of doctors, administration staff and medical students.
Results
A total of 309 patients were identified and collected from both centres: 211 from WCUH (215 identified of which four were excluded due to inability to validate data) and 98 from CWH (98 identified, 0 excluded).
Demographics
At WCUH the mean age of patients was 78 ± 15 1SD, with 48% men and 52% women. CWH had a mean patient age of 74± 15 1SD, with 50% men and 50% women. The total dataset gives a mean patient age of 77± 15 1SD, with 49% men and 51% women.
Statin prescription
At WCUH, among the 211 inpatients, 30% of patients had CVD risk factors but were not prescribed statins in accordance with NICE guidelines. Similarly, at CWH, among the 98 inpatients, 33% of patients had CVD risk factors but were not prescribed statins to reduce their risk of cardiovascular events.
From the group of at-risk patients for whom statin is indicated but not prescribed, 17% of WCUH patients and 19% of CWH patients suffered from ischaemic heart disease. Cerebral vascular accident is the most neglected indication, 10% of patients from CWH and 5% of patients from WCUH have a past history of cerebral vascular accident. Figure 1 illustrates in this group of neglected at-risk patients, the most common CVD risk factors are: ischaemic heart disease (18%), cerebral vascular accident (8%), hypercholesterolaemia (1%) and peripheral vascular disease (1%). Additionally, 40% of these patients are over the age of 70 and suffer from a combination of hypertension and diabetes.
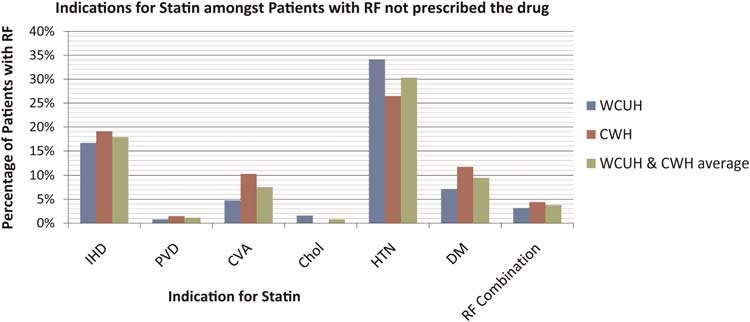
Graph showing the most frequent indications found in at-risk patients who were not prescribed statins. IHD = ischaemic heart disease; PVD = peripheral vascular disease; CVA = cardiovascular event; Chol = hypercholesteraemia; HTN = hypertension; DM = diabetes mellitus; RF (risk factor) combination = hypertension, diabetes mellitus and age older than 70 years
Conversely, there were patients for whom statins were not indicated, but were prescribed the drug; they comprised 6% of the statin-taking population at WCUH and 5% of statin-taking population at CWH (Figure 2).

Pie charts showing patients prescribed statins in relation to those with or without cardiovascular disease risk factors
Discussion
The aim of this cross-sectional study was to identify whether NICE guidelines on statin prescription were being effectively implemented across two geographically distinct hospitals in London.
The results indicate that there are a large number of patients who should be on a statin, according to NICE guidelines, but are not. It may be that this discrepancy results from clinician unfamiliarity with the actual guidelines which would also explain why some patients are on statins, despite statins not being clinically indicated. However, it is notable that the omissions in statin prescription decrease with an increase in the number of CVD risk factors the patient has, i.e. a patient with a single CVD risk factor is less likely to be prescribed the statin which he needs than a patient with two or more CVD risk factors. Having said this, 29% of WCUH patients and 37% of CWH had statins omitted despite having two or more CVD risk factors (Figure 3).
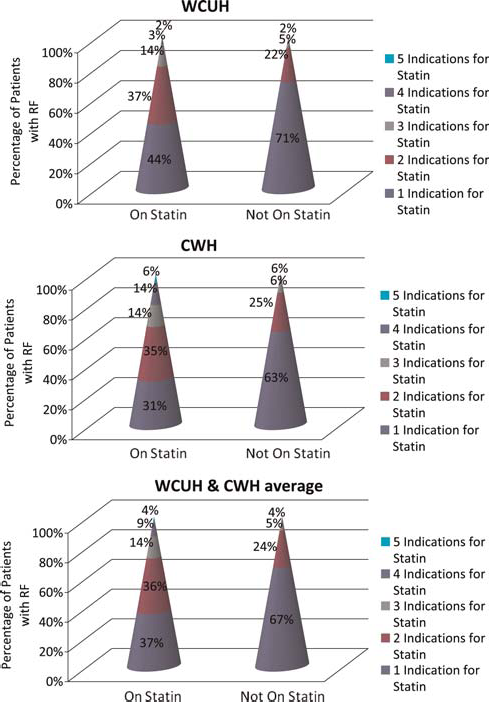
Cone plot showing the number of cardiovascular risk factor indications among patients on statin and patients not on statin
Our results prompt us to investigate other hospitals in London to gather more evidence for our hypothesis that there is no association between statin prescribing habits and the socioeconomic status of the area in which the hospitals are based. Perhaps the failure to effectively prescribe statins is not dependent on the socioeconomic status of the area, but actually reflects a London-wide crisis that requires immediate resolution.
In 2006, CVD cost the NHS £14 billion.12,13 With the huge amount of aforementioned evidence showing that statins lower CVD events and are an effective primary and secondary prevention strategy, we can conclude that some of the CVD cost burden on the NHS is the result of suboptimal statin prescribing.
Clinical guidelines must be met in order to provide effective prevention strategies and benefit the population in the long term. Daily plans and events for patient care are well documented in the patients’ notes; however, it is the drug charts which act as pivotal records from which healthcare professionals implement drug therapies. Drug charts already have an organized layout so that important drug therapies are not overlooked and also have a system of checks to ensure due attention is placed on certain aspects e.g. allergies. This is an ideal place for a statin prescription check to take place such as a simple box on the front page that asks the healthcare professional to acknowledge whether or not a statin is required, by ticking off a box. This compulsory consideration of statin prescription should emphasize an action to initiate a CVD risk factor assessment of the patient.
Conclusion
This London-based audit has revealed the inadequacy with which patients are prescribed statins and this will have huge implications not only for inpatients but the continuation of this omission when the patient is once more in the community. Hence, there is a considerable obstacle to the effective reduction of CVD both in the primary and secondary prevention setting. Furthermore, this suboptimal usage of statins in moderate to high-risk patients is reflected in both London centres, which are diverse in terms of socioeconomic and geographical placement. This supports the theory that it is actually clinician omission rather than any other variable, i.e. localized prescribing habits or patients’ economic status, which leads to the suboptimal statin prescription. Patients with a single CVD risk factor are the ones who are not prescribed a statin on most occasions. This omission is almost certainly contributing to the CVD cost burden on the NHS and changes in current practice could have widespread implications, not only economically but also on the incidence of CV events. Furthermore, improvements in secondary care drug prescribing will be propagated into primary care, once the patient is discharged back into their community.
Footnotes
Acknowledgements
The authors thank Peter Mills for his guidance and support