
Abstract
Objectives
To examine the prevalence of risk factors for diabetes and its complications in the Co-operation Council of the Arab States of the Gulf (GCC) region.
Design
Systematic review.
Setting
Co-operation Council of the Arab States of the Gulf (GCC) states (United Arab Emirates, Bahrain, Saudi Arabia, Oman, Qatar, Kuwait).
Participants
Residents of the GCC states participating in studies on the prevalence of overweight and obesity, hyperglycaemia, hypertension and dyslipidaemia.
Main outcome measures
Prevalences of overweight, obesity and hyperglycaemia, hypertension and hyperlipidaemia.
Results
Forty-five studies were included in the review. Reported prevalences of overweight and obesity in adults were 25–50% and 13–50%, respectively. Prevalence appeared higher in women and to hold a non-linear association with age. Current prevalence of impaired glucose tolerance was estimated to be 10–20%. Prevalence appears to have been increasing in recent years. Estimated prevalences of hypertension and dyslipidaemia were few and used varied definitions of abnormality, making review difficult, but these also appeared to be high and increasing,
Conclusions
There are high prevalences of risk factors for diabetes and diabetic complications in the GCC region, indicative that their current management is suboptimal. Enhanced management will be critical if escalation of diabetes-related problems is to be averted as industrialization, urbanization and changing population demographics continue.
DECLARATIONS
None declared
This study was supported by sponsorship provided to Layla Alhyas by the United Arab Emirates Ministry of Research and Higher Education, Abu Dhabi. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript
Not applicable
LA
LA created and revised the research strategy; LA and AMcK selected and assessed the quality of the studies, and analysed the data from the studies; all authors wrote and revised the paper
Paramjit Gill
Introduction
The increasing prevalence of diabetes mellitus, particularly type 2 diabetes mellitus, is well documented. 1 Type 2 diabetes is currently estimated to account for over 90% of the global diabetes burden. 2 Together with similar trends in other non-communicable diseases, it leads to risks not only for individuals, but for health systems, social systems, and state economies. This risk is in part to do with an anticipated relatively dramatic rise in countries with relatively young populations, and still developing economic infrastructure, as they undergo the predicted increases in prevalence of diabetes associated with changes in lifestyle and economic development, and population growth. Even when based on changes in population size and demography alone, 3 the highest predicted future increases are expected in the International Diabetes Federation's ‘African’ region (estimated 98.1% increase 2010–2030), followed by the ‘Middle East-North Africa’ region (estimated 93.9% increase 2010–2030 4 ). The Middle East-North Africa region already has some of the highest rates of diabetes in the world. The countries of the Co-operation Council for the Arab States of the Gulf (GCC) include those currently ranked 2, 3, 5, 7 and 8 for diabetes prevalence among the 216 countries for which data are available. 4
This high prevalence in the GCC states is associated with higher prevalences of risk factors for type 2 diabetes in this region. The International Diabetes Federation suggests the following as risk factors for type 2 diabetes: age, obesity, family history, physical inactivity, race and ethnicity, and gestational diabetes. Of the modifiable risk factors, physical inactivity appears to have been surprisingly little studied in this region, although it is likely to be correlated with overweight and obesity, which have been relatively well studied.
We aimed to review the prevalence of overweight and obesity in the GCC region. We also aim to review the prevalence of potentially ‘prediabetic’ hyperglycaemia (measured either as impaired fasting glycaemia, impaired glucose tolerance or raised random glucose). We also examined hypertension and dyslipidaemia, which are risk factors for adverse outcomes in people with diabetes.5–7 Diabetes is complicated by various micro- and macro-vascular conditions and people with metabolic syndrome — a collective of obesity, insulin resistance, dyslipidaemia, hypertension and hyperglycaemia8–12 — have a relatively higher prevalence of cardiovascular disease than those without. 13 Due to the heterogeneity of studies identified on preliminary searching, there was no anticipated meta-analysis.
Methods
Review question
A literature search was used to identify material relevant to the following review question: What are the prevalences of overweight and obesity, hyperglycaemia, hypertension and dyslipidaemia in the GCC region?
Search strategy
We developed a systematic review protocol (available from the authors on request) using the Centre for Reviews and Dissemination guidelines. 14 Medline and Embase were searched separately on 15 July 2009 and the search was repeated on 03 July 2010 (via Dialog and Ovid, respectively; 1950 to July week 1 2010, and 1947 to July 2010) using terms identified from PICOS deconstruction of the above review questions, and database- and manually- derived alternatives (Appendix 1). The search strategy was trialled, reviewed by independent professional colleagues (IW, KP) and updated before use. Further relevant studies were identified by searching the reference lists of the database-derived papers, contacting expert investigators, screening conference proceedings, citation searching and hand searching the International Journal of Diabetes and Metabolism and the Saudi Medical Journal, for the periods 1993–2009 and 2000–2010, respectively.
Selection of studies
The search yielded 1331 studies. The titles and abstracts were evaluated by one reviewer to determine eligibility for full screening. All studies wherein overweight, obesity, body mass index (BMI), hyperglycaemia, hypertension and dyslipidaemia were investigated were eligible for inclusion. No limitations on publication type, publication status, study design or language of publication were imposed. However, we did not include secondary reports such as review articles without novel data synthesis. The inclusion criteria required that the study population be of a GGC country, but otherwise all ages, sexes and ethnicities were included, resident and expatriate populations, urban and rural, of all socioeconomic and educational backgrounds. Studies of general, working, young, student, healthcare attending, and other populations were included. We did not specify diagnostic criteria for the studied conditions, but incorporated them into our data synthesis.
A total of 1331 studies were identified. The full texts of these studies were each considered by two reviewers (LA and McK). All studies of diabetic populations were excluded,15–17 and studies wherein people with diabetes had been excluded from the study population were excluded.18,19 Further exclusions were made on the basis that the studies were:
The selection process is summarized in Figure 1.
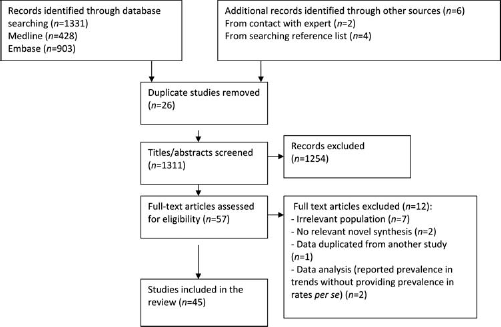
Flow chart of study selection process
Data extraction/quality assessment
The data extracted from each study included data relating to: (1) methods (study design, recruitment, measurement tools, analysis); (2) participant characteristics; (3) setting; and (4) outcomes (those observed, their definitions, results of analysis). Study quality was assessed using a checklist adapted from the Centre for Reviews and Dissemination guidelines. 14 As the identified studies were relatively few and heterogeneous, no study was excluded on the basis of quality alone; rather the assessment was used to inform synthesis. Data extraction was performed, in duplication, by two reviewers (LA and AM), and disagreement regarding any study eligibility was resolved through consensus and seeking the opinion of the third reviewer (AM).
Data synthesis
Data synthesis included summarizing the results of the data extraction process, considering the strength of evidence relating to various questions formulated a priori (see the Results section), and examination of results inconsistent with our formed proposals. In the cases of hypertension and dyslipidaemia, synthesis was limited by the number of studies identified, and in these cases description and discussion suffices.
Results
Forty-five studies (43 papers) relating to risk factors and their prevalence were identified for review. All papers identified were journal articles published between 1987 and 2010. Five studies were carried out (where reported) and/or published in the late 1980s, 23 in the 1990s, and 15 in the last 10 years. Studies of various 20 Saudi,24–46, seven Kuwaiti,47–50 three Bahraini,51–53 eight Emirati,54–60 four Omani61–64 and one Qatari 65 populations were included. All were cross-sectional studies; 23 of the general population, seven of primary care populations, four of schoolchildren, three of students, one of a young population, five of working populations. Women were exclusively studied in five cases, men in six. Sample size ranged from 215 to 25,337.
In addition to examining the prevalence of the particular risk factors in the GCC states, we were interested in the following:
Trends in prevalence across time;
Differences by country;
Trends in prevalence associated with age;
Sex differences;
Location (urban/rural) differences;
Prevalence in children.
Only in the cases of overweight and obesity, and hyperglycaemia were study numbers sufficient that reasonable conjecture regarding subgroups could be made. They are considered separately, for each risk factor, below.
Obesity/overweight
Thirty-three studies addressed the prevalence of overweight/obesity (Table 1).
Summary of overweight/obesity prevalence data

Summary of cross-sectional studies investigating the prevalence of overweight/obesity in the GCC region
Employees of Saudi National Guard and dependents
‘Mostly settled tribal men’
Attendees at primary healthcare centres with minor complaints, plus accompanying persons
AII subjects recruited via family member at UAE University
Adult attendees of the Kuwait Medical Council and Public Authority for Social Security (government employed/retired population)
Employees of Kuwait Oil Company
Age-adjusted data
Quality assessment checklist adapted from the Centre of Reviews and Dissemination guidelines (CRD) for non-randomized studies:
(1) Was the aim of the studv stated clearly?
(2) Was the methodology stated? And was it appropriate?
(3) Were appropriate methods used for data collection and analysis?
(4) Was the data analysis sufficiently rigorous?
(5) Were preventive steps taken to minimize bias?
(6) Were limitations of the study discussed?
In systematic review, was search strategy adequate and appropriate?
PC = primary healthcare-registered population; GP = general population; WP = working population; SC = schoolchildren; SP = student population; YP = young population
Overweight and effect of date and country
The reported prevalence rates of overweight (BMI 25 to <30) in adults ranged from 26.3–48% in men, and 25.2–35% in women. Although higher values are displayed in Table 1, they have been scaled down for/omitted from comparison as either the definition of overweight used included the typical definition of obesity, or the prevalence was given only by age group, allowing the possibility that similarly high figures were masked in the age-nonspecific data of other studies. A lower value has also been omitted where the study population was particularly young. 54 Within these ranges, the data were fairly even distributed between the limits, and reported sex-nonspecific prevalences were also consistent with these figures. The data showed no obvious trends or anomalies by date or country, although the data from Oman (two studies, reporting combined overweight/obesity rates) suggest prevalence there may be relatively low.
Obesity and effect of date and country
The reported general prevalence rates of obesity (defined as BMI ≥ 30) in adults ranged from 13.05–37% in men, and 16–49.15% in women (again a lower value has been omitted where the study population was particularly young 54 ). As for the overweight data, the reported sex-nonspecific data are consistent with these figures, and potentially excepting the Omani data, show no obvious trends or anomalies by date or country.
Obesity and overweight and age
Age as a potential predictor of prevalence of overweight/obesity was considered in eight studies (of adult populations), and the results were tested for significance in two cases. These latter studies demonstrated correlation between overweight/obesity and age, 36 and a significantly higher mean BMI in a 45–54-year age group versus a 55–64-year age group. 49 Similarly, all remaining studies indicated that prevalence increased with age to a threshold level (variably between 30–40 and 50–60 years (potentially younger in women) after which it began to fall, or fluctuate.27,33,47,48
Obesity and overweight and sex
Most studies reported prevalence rates by sex, but only four tested for differences. Of these four, in all cases but one, BMI/prevalence of obesity and overweight was higher in women,35,54,60 and where overweight was higher in men, 36 the combined prevalence of overweight/obesity remained higher in women. In the remaining studies, prevalence of obesity, and the combined prevalence of overweight/obesity was again always higher in women, although in some cases the ‘difference’ was slight.
Obesity and overweight and residential environs
Six studies considered prevalence in urban versus rural populations. In three, mean BMI was found to be significantly higher in rural populations.31,33,34 In a further two studies, prevalence of both overweight and obesity were significantly lower in rural regions.29,30 This trend (with one subgroup exception — female obesity) was also observed where significance of differences was unclear. 51
Obesity and overweight in national/expatriate populations
Only one study considered prevalences in national versus expatriate populations. This reported that the combined prevalence of obesity and overweight was higher in Kuwaitis versus non-Kuwaitis. 66
Obesity and overweight in children
In keeping with the association with age, prevalences in children/young people (<20 years) are lower than those in adult populations. However, there is a greater indication that prevalences in the younger populations are increasing. Single figure prevalences were reported until around 2000, and have not been observed since. The most recent reports (suggesting prevalences of combined overweight and obesity >30%) provide rates comparable to those in adults. Although less considered, there is again evidence for higher prevalences with increasing age in these relatively young populations,47,56,67 in urban areas 57 and in girls.39,57
Hyperglycaemia
Seventeenstudies28,29,40–45,49,50,53,59,61,63–65 reported on the prevalence of hyperglycaemia, 12 studies as impaired glucose tolerance,28,29,40–44,53,63–65 three studies as impaired fasting glucose45,59,61 or a high random capillary glucose (>10 mmol/L).49,50 A summary is provided in Table 2. Generally, impaired glucose tolerance was defined as venous plasma glucose ≥7.8 and <11.1 mmol/L 2 h post glucose loading. Where the World Health Organization 1980 criteria were used, however, the impaired glucose tolerance would be defined as venous plasma glucose 8.0 and 11.0 mmol/L 2 h post glucose loading, and the study of Al-Moosa et al. 62 involved capillary whole blood rather than venous plasma samples (Table 2). Impaired fasting glucose was consistently defined as a fasting venous plasma glucose >6.1 and < 7.0 mmol/L. The studies of random capillary blood glucose and impaired fasting glucose are so few that interpretation is difficult. Additionally, the random glucose measurement figures are likely to include instances of transient/‘stress’ hyperglycaemia. Nevertheless, both are potentially consistent with the impaired glucose tolerance results.
Summary of hyperglycaemia prevalence data

Summary of cross-sectional studies investigating the prevalence of (non-diabetic) hyperglycaemia in the GCC region
Government/municipal salaried workers
Adult attendees of the Kuwait Medical Council and Public Authority for Social Security (government employed/retired population)
Selection of subjects intentionally biased towards UAE citizens
Quality assessment checklist adapted from the Centre of Reviews and Dissemination guidelines (CRD) for non-randomized studies:
(1) Was the aim of the study stated clearly?
(2) Was the methodology stated? And was it appropriate?
(3) Were appropriate methods used for data collection and analysis?
(4) Was the data analysis sufficiently rigorous?
(5) Were preventive steps taken to minimize bias?
(6) Were limitations of the study discussed?
(7) In systematic review, was search strategy adequate and appropriate?
Prevalence of impaired glucose tolerance and age
Broadly speaking, the relatively comprehensive study of impaired glucose tolerance is suggestive of a recent and ongoing increase in prevalence, with the latest published figures suggesting rates of perhaps 10–20% in the adult population. Although there are some inconsistent figures (Table 2), we consider that these could be accounted for by a combination of changes in prevalence across time and the ages of the studied populations. The studies of El-Hazmi et al. 44 in particular reports an inconsistently low figure, but their sample was 39.1% children and the authors report a significantly higher prevalence with increasing age, although we could not access the full data and the statistics were not described. Similarly, the other relatively young populations are those wherein reported prevalences are relatively low. Furthermore, of all studies reviewed (including those of random blood glucose and impaired fasting glucose), five considered the effect of age on prevalence.42–44,49,50 All found the prevalence was higher with advancing age, and in all cases where tested (three cases), the relationship was found to be significant.43,49,50
Prevalence of hyperglycaemia by country
There was no obvious discrepancy in prevalence by country, but the number of studies available prohibited a reasonable comparison.
Prevalence of hyperglycaemia by sex
Thirteen studies reported differential prevalence rates by sex, although not all considered the strength of sex differences. The majority of studies (10) suggested a higher prevalence in women.29,41–43,45,46,53,59,63,65 Two demonstrated a significantly higher prevalence.41,59 Conversely, two studies50,61 showed a higher prevalence in men (one significantly so 61 ), and one demonstrated no sex difference. 45
Urban/rural residence and prevalence of hyperglycaemia
Only one study reported prevalence according to urban versus rural residence. 29 Prevalence was higher in urban areas.
Prevalence of hyperglycaemia by residential status
No studies reported on effects of ethnicity, or on the prevalence of hyperglycaemia in national versus expatriate populations.
Hypertension and dyslipidaemia
Only few of the identified studies investigated the prevalence of hypertension34,46,59,60,62,65 and dyslipidaemia.34,49,62,66 Moreover, variable or ill-defined definitions of the diagnosis were used in each case.
Hypertension
We identified eight studies that included an assessment of hypertension.30,34,46,59,60,62,65,66 The definitions of hypertension employed ranged from ≥140/≥90mmHg to > 160/95 mmHg, and variably included those on antihypertensive medication. Additionally, one study 34 depended upon a previous (undescribed) diagnosis. Reported rates of hypertension ranged from 6.6–33.6%. Potentially prevalence has been increasing since 1993–1994 (when the first identified studies were undertaken).
Dyslipidaemia
Dyslipidaemia was considered in six studies.34,46,49,50,62,65 Dyslipidaemia was defined as: cholesterol ≥5.2 mmol/L, cholesterol >5 mmol/L, high density lipoprotein < 1.0 mmol/L, low density lipoprotein > 4.1 mmol/L, triglycerides ≥2.3 mmol/L, or a previous (undescribed) diagnosis. Reported rates of dyslipidaemia ranged from 2.7–51.9%. This relatively large range is potentially partially due to increasing rates across recent years, to consideration of different aspects of the lipid profile in different studies and to differing definitions of abnormality. Additionally, in the study reporting the very lowest prevalence, 34 diagnosis was established by ‘previous diagnosis’ alone, and thus allowed no assessment of the extent of undiagnosed cases.
Discussion
We found the prevalence of overweight to be 25–50%, obesity 10–50%, relatively high in women and higher with advancing age to threshold levels between 30–40 and 50–60 years. Prevalence was also found to be high in children, and appeared to be increasing in this group. We estimated, from relatively recent reports, the prevalence of hyperglycaemia in adults (using impaired glucose tolerance as the outcome measure) to be approximately 10–20%. Prevalence of hyperglycaemia appears to have been increasing across recent years, and higher prevalence again showed an association with advancing age and female sex. There has been relatively little research of the prevalences of hypertension and dyslipidaemia in the GCC region and a lack of consistency in definitions used for study. Accordingly, estimates of prevalence vary: between 6.6–33.6% for hypertension, between 2.7–51.9% for dyslipidaemia, and it is unclear what additional factors may have impacted on these ranges.
Potentially, the prevalences of hypertension and dyslipidaemia are increasing, which would be in keeping with a more widespread trend.68–70 The increasing prevalence of hyperglycaemia is similarly in keeping with trends reported elsewhere. By contrast, we observed no obvious temporal trend in prevalence of overweight and obesity in adult populations, which is not in keeping with reports from elsewhere, and despite a relatively well established association with diabetes (both epidemiologically and pathophysiologically1,71–73) and pathophysiologically. Importantly, though, particular authors have noted a rising prevalence within the relatively well controlled environments of their own studies,47,48 and several of the reviewed studies did demonstrate correlation between BMI, and overweight and obesity, and diabetes or blood glucose concentration.28,35,50 Moreover, the observed prevalence of overweight and obesity by age, increasing with advancing age until a plateau or decline in middle and older age, is suggestive that overweight and obesity may be an important risk factor for diabetes.
We noted differences in the patterns of spread of diabetes and obesity and overweight in the GCC region. For example, the observed bias of obesity and overweight to the female population is not obviously replicated in the population distribution of diabetes (unpublished data), demonstrating that additional aetiological factors may hold important roles in the current expansion of the diabetes problem.
Implications
We consider the need for further study to identify the major contributory factors to the current diabetes problem in the GCC region, and of factors such as hypertension and dyslipidaemia that compound the risks of diabetes, an important outcome of our review. The limited number and heterogeneity of existing studies pose difficulties for targeting, designing and developing potential management strategies. The relatively high levels of hyperglycaemia, and obesity and overweight (and potentially of hypertension and dyslipidaemia) observed — and their possible rising prevalences — are indicative that current management is insufficient. The reviewed data are suggestive that age and urban residence may be risk factors for, at least, overweight/obesity and hyperglycaemia. Enhanced management is thus crucial to prevent escalation of the problems as urbanization and changing population demographics continue.
It would be useful to determine that the situation is similar across the various GCC states. This is likely but cannot be confirmed from the data reviewed here. If so, expansion of existing management strategies, and coordination of novel strategies, across the region, would probably be relatively successful and relatively cost-effective. The likely contribution made by overweight/obesity to the diabetes problem in the GCC region is suitable for management, at least in part, by primary preventative measures, which we anticipate would also be relatively cost-effective.
Limitations of study
We report above that individual studies included in our review demonstrated recent temporal trends in prevalence of overweight and obesity, even though this was not clear from our overview of studies. This is probably illustrative of the general heterogeneity of the reviewed studies. The studies reviewed were relatively few and distributed across many years. They were of varied population characteristics, in different regions of six countries, and the utilized definitions of particular risk factors were inconsistent. We were thus able to make only relatively crude observation, and could not provide measures of confidence in our outcomes. The quality of reporting of results in the examined studies was also variable. For example, many studies did not report confidence intervals or had missing data for key variables. This reinforces the need for authors of risk factors studies to use standard methods for reporting the results such as STROBE guidelines.
Although quality was variable, it was never alone a reason for exclusion. Quality was, rather, incorporated into building our estimations of ranges for normal versus abnormal among the results returned. This was difficult due to the wide variability in these results, and the potential for bias has implications for the strength of our proposals. In addition, we may have increased bias by duplication of included data, as it is anticipated that the female sample of one Al-Isa study 47 is that included in the mixed sample of another, 48 and the male sample of Jackson et al. 49 that included in the sample of Jackson et al. 50 Finally, all of our reviewed studies were published in English, although we had no language restriction. Hence, we may have limited capture of publications in other languages due to the databases we searched.
Conclusions
Prevalence of overweight and obesity in the GCC region is high and the ages of those affected suggest it may be a relatively important factor in the growing diabetes burden in this region. Further study aimed at elucidating its relative contribution to the diabetes problem is desirable, but regardless the reviewed data are suggestive that implementation and enhancement of primary preventative strategies in particular would be useful in the management of type 2 diabetes in the GCC region. The current prevalences of hypertension and dyslipidaemia are unclear, but potentially relatively high compared to many other parts of the world. More comprehensive study of their prevalence is desirable, and standardization of definitions of these conditions will be important if further study is to be maximally useful. Primary preventative strategies may also be useful in managing these conditions.
Footnotes
Acknowledgements
The authors are grateful for contributions from Igor Wei and Kate Perris who assisted with the electronic search strategy