
Abstract

DECLARATIONS
None declared
None
Written consent to publication has been obtained from the patients or next of kin
AC
Both authors contributed equally
Shaima Elnour
Emergency management of two cases of acute gastric dilatation are discussed, causing respiratory compromise and requiring active decompression with nasogastric tube.
Case 1
A 64-year-old man was referred to the on-call surgical team from the High Dependency Unit with acute abdominal distension. He had undergone elective abdominal aortic aneurysm (AAA) repair two days previously. The patient had not vomited, was diaphoretic, and had difficulty speaking due to discomfort and respiratory distress. He was tachypnoeic with a respiratory rate of 24/min, tachycardic at 110 bpm, and hypotensive at 90/60 mmHg. Pulse oximetry demonstrated adequate saturations of 96% on FiO2. An ECG confirmed sinus rhythm without ischaemic changes. On respiratory examination there were globally reduced breath sounds consistent with hypoventilation. The abdomen was tense, markedly distended but only minimally tender, and a pronounced succussion splash was elicited by gently rolling the patient. Review of the fluid balance chart revealed liquid feeding by nasogastric tube and 1 L intravenous fluid administration 8-hourly, and oliguria with urine output <30 mL in 4 hours.
The initial concern was that of abdominal compartment syndrome. Since the nasogastric tube was in situ, aspiration of gastric contents was attempted given the clinical findings, with removal of over 5 L of liquid feed. Abdominal girth decreased markedly, and ventilatory function correspondingly improved. The patient subsequently made a rapid recovery and was discharged one week later.
Case 2
A 72-year-old man with type 2 diabetes mellitus and severe Parkinson's disease was referred to the acute medical on-call team with a 4-day history of nausea and vomiting, and mild abdominal discomfort. Examination revealed profound bradykinesia, tachypnoea with a respiratory rate of 22/min, a pulse rate of 95 bpm, but normotension at 115/85 mmHg and oxygen saturation of 97% on air. An electrocardiogram demonstrated sinus rhythm without ischaemia. There was reduced chest expansion bilaterally with quiet breath sounds; the abdomen was swollen and tense, tympanic, but relatively painless. No succussion splash was elicited. A plain abdominal film revealed a grossly enlarged gastric shadow (Figure 1). CXR revealed under-inflated lung fields with no pneumoperitoneum (Figure 2). Blood showed elevated white cell count of 27.2 × 109/L and C-reactive protein of 369 mg/L, and acute renal failure with a urea of 23.7 mmol/L and creatinine of 270 μmol/L.

Plain abdominal radiograph of case 2 showing a large superior gastric shadow reaching inferiorly to the lumbar spine and faecal loading in transverse/descending colon

AP erect chest plain radiograph of case 2 showing severely decreased lung fields, especially of the left hemi-diaphragm and the superior half of the enlarged gastric shadow seen in the abdominal radiograph of the same patient
Nasogastric tube insertion was attempted, and a saline aspirate with a pH of 3 obtained. No further fluid was withdrawn, however, on attempted aspiration and there was no spontaneous air decompression. The patient unfortunately subsequently deteriorated over the following 12 hours and died of suspected aspiration.
Discussion
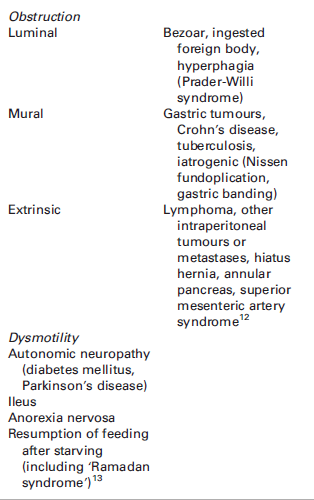
Acute gastric dilatation is a rare cause of acute dyspnoea and respiratory compromise, which may as in our cases require emergency decompression. It constitutes a surgical emergency, as delayed treatment can result in gastric necrosis, perforation, abdominal compartment syndrome and severe sepsis. The causes are varied, but either cause physical obstruction or profound dysmotility (Box 1), and often multiple factors act in synchrony in individual patients. Studies into normal gastric capacity using intra-gastric balloon expansion demonstrate that healthy individuals tolerate volumes of up to 800 mL; this along with gastric emptying half-life are increased in patients with bulimia. 1
Classification of causes of acute gastric dilatation
The most common clinical presentation of acute gastric dilatation is with relatively painless abdominal distension.2–11 The abdomen will be tympanic on percussion and a succussion splash may be elicited, but only if the gastric contents are liquid. Plain abdominal radiography will review the grossly enlarged gastric shadow, and nasogastric insertion can be both diagnostic and therapeutic. An elevated white cell count and deranged renal function, as in the second case, are ominous findings as they may be indicative of pressure necrosis and ischaemia of the gastric lining and ensuing complications. 5 Perforation and sepsis have been widely reported, 7 as has abdominal compartment syndrome through rapid elevation of the intra-abdominal pressure by >20 mmHg. 4 Type I or II respiratory failure can arise through aspiration or diaphragmatic splinting, respectively.9,10 The latter may also result in cardiac compromise due to impaired venous return and elevated systemic after-load.
Passage of a nasogastric tube as an emergency is the first-line treatment, irrespective of the underlying cause of gastric dilatation. The clinician should not leave the bedside until decompression is achieved. As in case 1, active aspiration may be required as drainage will not always be achieved spontaneously.
Should attempts at inserting a nasogastric tube be unsuccessful, placement under direct endoscopic or fluoroscopic guidance may be required. If these too are unsuccessful, or there is suspicion of a perforation or abdominal compartment syndrome, emergency laparotomy should be organized. 6
Conclusion
We present two cases of acute gastric dilatation causing respiratory compromise, presenting to both the surgical and medical on-call teams. Both required emergency active decompression with nasogastric tubing. A high clinical index of suspicion reliant on thorough and appropriate clinical examination and emergency radiology is essential for timely intervention in such patients, who are usually extremely unwell and often co-morbid.
Footnotes
Acknowledgements
None