
Abstract

Cerebellar metastases from bladder cancer are rare, but with timely diagnosis may be treated successfully by surgical and adjuvant therapies.
DECLARATIONS
None declared
None
Written informed consent to publication has been obtained from the patient or next of kin
HM
ND'S collected the data, searched the literature, drafted and revised the paper; MJK wrote and revised the paper; SR suggested the case report be published after his involvement in patient management; HM approved the final version of the paper
Ivan Hoh
Introduction
Cerebellar metastases from superficial bladder cancer are extremely rare. Bladder cancer is the second most common cancer of the urinary tract. It is the fourth most common cancer in men and eight most common in women in Europe where its incidence is estimated at 104,000 in 2006. Seventy percent 1 of bladder cancer is confined to the mucosa (Ta, CIS-T1), but 30% is invasive. The most common solid organs with metastatic spread are lung (24–36%) and liver (21–35%). Brain metastases are rare, with previous estimates at 0.3–8%. 2
We present the case of a successfully treated solitary cerebellar metastasis that presented 11 months following resection of organ-confined transition cell carcinoma.
Case report
A 69-year-old woman was seen by a GP with painless visible haematuria and enterococcus urinary tract infection. Her only other co-morbidity was of epilepsy well-controlled with medication. Treatment with antibiotics cleared up the haematuria, and she was referred to the outpatient urology haematuria clinic in January 2008.
She had a flexible cystoscopy in February 2008, which showed a large mass on the right lateral wall. A computed tomography (CT) scan showed at least a 2 cm mass on the right lateral wall. She underwent a transurethral resection of her bladder tumour in March 2008. Staging CT and ultrasound scan showed no evidence of lymph node or metastatic spread (Figure 1).
Soft tissue mass arising from right lateral wall of bladder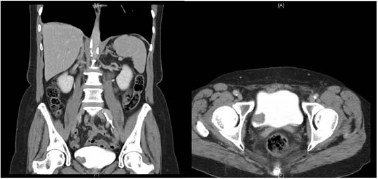
Histology from the transurethral resection of her bladder tumour revealed a G3pT1 tumour with probable lymphatic invasion, but no muscle involvement or evidence of carcinoma in situ. The patient then underwent six cycles of BCG instillation. Follow-up biopsies taken in April and August 2008 showed no malignancy.
In January 2009, she developed new onset slurring of speech, left-sided facial drooping, left eye visual disturbance and ataxia. She was diagnosed with a Tegretol overdose by her GP. Following progression of her symptoms over three weeks, she was urgently referred to a neurologist. Her signs now also included nausea, confusion and headaches, and she was admitted to hospital for an urgent CT scan of her head. This revealed a 4.8 cm mass in the right cerebellum (Figure 2).
4.8 cm cystic mass right cerebellum
She was immediately transferred to the local neurosurgical unit, and underwent de-bulking of posterior fossa metastases. Histology of the biopsy showed ‘cerebellar tissue infiltrated by an epithelial tumour composed of papillae of moderately atypical cells with weakly eosinophilic cytoplasm. Surrounding tissue shows reactive gliosis, chronic inflammation and granulation tissue’, with a final diagnosis of ‘metastatic transitional cell carcinoma consistent with bladder primary’. Subsequent immunocytochemistry showed ‘the immunoreaction for 34BE12 is positive in neoplastic cells confirming the diagnosis of metastastic transitional cell carcinoma’.
She subsequently had full brain radiotherapy, 30Gy in 10 fractions. Her one-month postoperative MRI showed only postoperative changes, and whole-body CT showed no other metastasis. Flexible cystoscopy done in October of that year did not reveal any recurrence. She remains well, 21 months post neurosurgery with no evidence of local recurrence or metastatic disease.
Discussion
Transitional cell carcinoma is the most common (>90%) primary bladder cancer. Risk factors for bladder cancer are smoking, male gender, increasing age, exposure to industrial and environmental carcinogens, chronic inflammation of bladder (bladder stones, long-term catheters and ova of scistosoma haematobium), drugs (phenacitin and cyclophosmamide) and pelvic radiation. No hereditary genetic cause for bladder cancer has been identified but some somatic genetic abnormalities have been reported. These are loss of chromosomes 9p, 9q, 11p 13q and 17q. Furthermore, activation of oncogenes (p21ras, c-myc, c-jun, erbB-2), inactivation of tumour suppressor genes (p53, retinoblastoma, p16 cyclin-dependent kinase inhibitor) and increased expression of angiogenic factors (vascular endothelial growth factor) are identified in transitional cell carcinoma.
Brain metastases from transition cell carcinoma of the bladder remains rare. A suggested mechanism for metastasis to the cerebellum is through retrograde dissemination via Batson's plexus to the vertebral venous system, to reach the intracranial venous sinuses. The time period for detection of metastases has been found in other studies to be between 7 to 40 months post-surgical treatment of primary transition cell carcinoma. Cerebellar metastases are more rare even than cerebral metastases. The first case of an isolated cerebellar metastasis was reported back in 1930. 3 There have been six cases reported in the literature4–7 of cerebellar metastases, nearly always with a high grade, high stage primary bladder cancer. This is only the second case 7 we have found reported of T1 bladder transition cell carcinoma, treated with surgical resection, that later developed a solitary cerebellar metastasis with no systemic relapse.
Conclusion
Brain metastasis from a non-muscle invasive bladder tumour is rare, but it should be considered as a differential diagnosis in a patient presenting with new focal neurological signs and known history of bladder cancer.
Footnotes
Acknowledgements
Rahul Koti