
Abstract

A case of a 14-year-old girl with a 2-year history of peripheral and sacroiliac joint pain and gastrointestinal symptoms, secondary to enthesitis-related arthritis, is presented along with the management.
DECLARATIONS
None declared
None
Written consent to publication has been obtained from the patient or next of kin
SJG
Both authors contributed equally
Gerry Schwalfenberg
Introduction
Previously considered a chronic condition, enthesitis-related arthritis - a type of juvenile idiopathic arthritis - may in some cases represent a sensitivity-related illness and thus respond to antigenic avoidance and remediation of biochemistry. Enthesitis-related arthritis is a rare but serious cause of childhood disability and chronic pain that often leads to continuing complications in adult life. Forming a small (1-16%) subset of children with juvenile idiopathic arthritis,1,2 enthesitis-related arthritis patients typically experience enthesitis and asymmetrical hip and lower extremity arthritis.3–5 Common systemic features include acute iritis 6 and subclinical inflammatory bowel disease (IBD), 7 while symptomatic cardiac myopathies and pulmonary parenchymal disease occur less commonly.1,8 Unlike adult-onset spondyloarthropathies, sacroiliitis in enthesitis-related arthritis tends to present years after disease onset. 8
To meet International League of Associations for Rheumatology (ILAR) classification for enthesitis-related arthritis, patients must have (1) arthritis and enthesitis; or (2) arthritis or enthesitis with at least two of the following:
Acute, symptomatic anterior uveitis; Sacroiliac joint or lumbosacral pain; Male gender and age over 6 years; HLA-B27 genotype; First-degree relative with history of ankylosing spondylitis (AS), enthesitis-related arthritis, sacroiliitis with IBD, Reiter's syndrome, or acute anterior uveitis.
Exclusion criteria for enthesitis-related arthritis include systemic juvenile idiopathic arthritis, psoriasis, or two positive findings of IgM rheumatoid factor occurring three months apart. 9
Genetic factors are particularly significant in enthesitis-related arthritis as 80% of cases are found to be HLA-B27 positive. 1 Possessing a HLA-B27 genotype confers a 20-fold increase in spondylopathy risk in Caucasian populations 10 and also increases risk of enthesitis-related arthritis progression to AS. 11 Moreover, HLA-B27 is implicated in cardiac, 12 pulmonary 10 and malignant 13 complications of spondylopathies. While multiple mechanisms have been proposed for the role of HLA-B27 allotypes in triggering autoimmunity, 10 research is still inconclusive on the exact pathophysiology.
Extensive work has been done on the extent to which genetics influence juvenile idiopathic arthritis and spondylopathies14,15 but environmental parameters remain largely unexplored due to the relative rarity of the condition and the continuing re-classification of juvenile idiopathic arthritis. Preliminary evidence implicates the absence of breastfeeding, maternal smoking, 16 and infection - particularly streptococcus and Epstein-Barr virus - in the development of juvenile idiopathic arthritis, 17 but further inquiry is needed. Although children with juvenile idiopathic arthritis are known to be at risk for malnutrition, nutritional studies have focused on BMI rather than specific biochemical deficiencies. 18
Management of enthesitis-related arthritis
Non-steroidal anti-inflammatory drugs (NSAIDs) remain the first-line treatment for enthesitis-related arthritis, while metrotrexate and sulfasalazine are often introduced in the early stages for better symptom control. 19 AntiTNF-alpha bio-logics, particularly etanercept, 3 are increasingly used in paediatric autoimmune disease. While generally well-tolerated, gastrointestinal symptoms including nausea, vomiting and abdominal pain are a significant adverse effect of all of these options,3,20 often complicated by inflammation due to disease activity. 21
Beyond gastrointestinal symptoms, each of these medications has significant side-effect profiles. NSAIDs are also associated with nephrotoxicity, headaches and behavioural changes, while methotrexate may cause (largely reversible) liver toxicity.4,22,23 Other reported adverse effects of methotrexate include loss of appetite, alopecia, malaise, leucopenia,19,24 and one case each of intestinal sprue 25 and skin toxicity. 26 Sulfasalazine may cause hepatitis, nephritis, 27 and haematologic abnormalities, 28 although these are all uncommon. 29
Meanwhile, antiTNF-alpha agents have been recently correlated to higher incidences of cancer in adults 30 as well as paediatric malignancy. 31 Although autoimmunity confers an innate predisposition to malignancy, genotoxic effects from antiTNF-alpha therapy in juvenile idiopathic arthritis have been shown to extend beyond pre-existing DNA damage. 32 Rarer events include possible increased occurrence of Crohn's disease with etanercept (although no conclusive link has been established). 33 Finally, steroids are avoided when possible, due to the well-known potential effects on bone density, mental health, weight and growth.34,35
Treatment outcomes vary. Although patients with juvenile idiopathic arthritis often achieve high educational and employment levels, 36 overall quality of life is most dependent on disease subtype, activity and progression. 37 One-third of juvenile idiopathic arthritis patients experience disease continuing into adulthood with full remission rates ranging from 87% in oligoarthritis to 17-33.4% in enthesitis-related arthritis.2,38 Unfortunately, progression to AS occurs in 39-75% of enthesitis-related arthritis cases3,39 even with the advent of new therapies. Though evidence on safety and efficacy is mixed,40–42 what is certain is that the longterm consequences of new immunosuppressive and biologic therapies in juvenile idiopathic arthritis will not be clear for another generation and caution must be exercised.
Case report
A 14-year-old girl with a history of enthesitis-related arthritis presented to an environmental medicine clinic, seeking adjunctive therapy for complications of her illness. An extensive history, physical exam, environmental assessment 43 and series of laboratory tests 44 were performed.
Sixteen months prior, the previously healthy patient had presented to a family physician with a one-week history of sudden-onset right knee pain. A joint aspirate was inconclusive for viral infection and naproxen was prescribed for pain control. Early investigations showed a positive result for antinuclear antibody and an elevated CRP (result 86.6 mg/L with normal 0-8 mg/L). Results were negative for Streptococcus, Lyme and Bartonella exposure. Family history included ulcerative colitis in her father, and paternal grandfather, although neither had sacroiliitis.
Over the next month, symptoms progressed to include stiffness and soreness in her lower back, bilateral knees and hips, right wrist and right first interphalangeal joint, at which point rheumatology was consulted and diagnosed enthesitis-related arthritis, although HLA-B27 testing was not done. Visualizing persistent joint effusions on ultrasound, the rheumatologist began methotrexate and what would become a five-month course of prednisone in addition to Naproxen. Sulfasalazine treatment began 14 months after disease onset, as the patient experienced increasing difficulty swallowing pills.
Although the patient noted some improvement with medications, soreness and stiffness remained in her back and affected joints. Intra-articular steroid injections were associated with improved function in her right wrist and thumb, and physiotherapy and occupational therapy were beneficial, but pain continued to limit her participation in sports and school activities. Schoolwork was also difficult as she was right-handed. Significant medication-related nausea and abdominal discomfort were only minimally lessened with antiemetic medication - ondansetron. However, the patient stated that compliance with ondansetron was poor as the sight of any pill became associated with nausea. Moreover, the course of prednisone had resulted in a 20 lb weight gain, about which the adolescent patient was quite self-conscious. While moderately satisfied with conventional treatment, the family regularly sought out alternative therapies such as craniosacral therapy and reflexology; these interventions were felt to be minimally helpful.
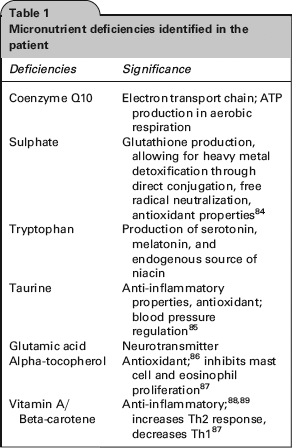
Medical records from the environmental health clinic revealed that physical exam was unremarkable aside from a high BMI, and exposure history was typical for a North American teenager. However, biochemical analysis showed severe nutritional abnormalities including low serum levels of tryptophan, taurine and glutamic acid, and low blood levels of zinc and copper. Serum levels of sulfate, co-enzyme Q10, alpha-tocopherol, vitamin A, B-carotene, and 25-hydroxy-vitamin D were also markedly low.
Toxicant analysis revealed elevated arsenic and mercury levels in whole blood, as well as the presence of two fungal mycotoxins - ochratoxins and tricothecenes in urine testing - suggesting a history of mold exposure. In light of the prednisone exposure, bone density analysis was conducted and found low - normal levels in the patient's hip and spine (total hip z-score -1.2; total spine z-score -0.9).
Given the evidence of toxicant bioaccumulation, it was hypothesized that the mechanism for development of enthesitis-related arthritis in this case might be related to epigenetic determinants and sensitivity-related illness 45 - a disease mechanism initially described in the literature by Claudia Miller in a 1996 paper in Toxicology 46 and thought to be mediated primarily through the action of pro-inflammatory cytokines. 45 Accordingly, proposed treatment focused on: (1) removing agents recognized as common antigenic triggers; (2) restoring nutritional adequacy; and (3) intervening to remove the bioaccumulated toxicants such as mycotoxins and other toxic elements. 45 This approach has proven worthwhile with other immune-related conditions. 47
Gluten and casein are commonly linked to sensitivity-related illnesses,
48
and were thus eliminated from the patient's diet along with refined sugar, artificial sweeteners, flavouring agents and corn. Next, initial supplementation focused on vitamin D, zinc, copper, DHA, strontium, vitamin K2, magnesium and probiotics, due to the following indications:
Vitamin D deficiencies are linked to auto immune rheumatic disease in adults,
49
and adequate levels are known to be anti inflammatory;50–52 Copper and zinc play significant roles as co-factors in normal immune functioning53–55 and deficiencies are linked to gut inflam mation.
56
Furthermore, copper and zinc deficiencies are associated with rheumatoid arthritis;57,58 Though evidence for probiotics is not yet con clusive,
59
they may decrease gut inflam mation,60–62 improve arthralgias,
63
and improve gut barrier function.
64
As the combination of steroid treatment and juvenile idiopathic arthritis are known to predispose patients to a higher lifetime risk of osteoporosis,65,66 a series of agents were targeted at bone health. Studies support the use of strontium, magnesium and vitamin D, and to a lesser extent, vitamin K2 and DHA in increasing osteoblast activity and restoring bone density67–73 Zinc and copper are increasingly recognized as important co-factors in preventing osteoporosis as well.74,75
Within one month, the patient saw significant improvements in function that allowed her to decrease, and then completely discontinue the methotrexate, sulfasalazine, naproxen and ondansetron after six months. At six months, antinuclear antibody testing was repeated and found to be negative, and CRP levels had returned to normal (result 1.0 mg/L), supporting the clinical picture of inactive disease. Two months after discontinuation, the patient reported that her functioning and quality of life were ‘just like before’ the onset of enthesitis-related arthritis, and she was fully participating in gym class without any concerns. She had lost the excess weight, was taking guitar lessons without further wrist or finger symptoms, and found the diet and lifestyle changes ‘more than worth it’ for the health she was experiencing. At 13 months post intervention, the patient remains completely well with no recurrence of symptoms. Follow-up will continue with the environmental health specialist to address the xenobiotics found on toxic elements and myco-toxin analysis - the suspected factors likely involved in the initiation of sensitivity-related illness in this patient.
Discussion
By the Wallace criteria, true remission of disease cannot be declared until the patient has been completely asymptomatic without medication for 12 months with no active arthritis; no fever, rash, sero-sitis, splenomegaly, or generalized lymphadenopathy attributable to juvenile idiopathic arthritis; no active uveitis; normal erythrocyte sedimentation rate (ESR) or CRP and a physician's global assessment of disease activity. 38 As the patient has been asymptomatic for over 12 months, she can be considered to be in full remission as she meets all criteria.
Nevertheless, to the authors’ knowledge, this is the first reported case of amelioration of enthesitis-related arthritis symptoms after treatment with dietary changes and nutritional supplementation. While studies have focused on specific areas of nutritional deficiency related to juvenile idiopathic arthritis,17,18,50,76 no treatment strategy has targeted environmental factors as key to enthesitis-related arthritis and its remission. Still, a growing body of evidence suggests sensitivity-related illness as a mechanism behind many cases of autoimmune disorders. 45 It is unknown to what degree the specific signs and symptoms in this case are the direct result of sensitivity-related inflammation or the secondary result of disordered biology resulting from nutritional deficiency. As maldigestion and malabsor-pion are common problems associated with food intolerance resulting from sensitivity-related inflammation, nutritional deficiency ensues -which may account for the malnutrition state in many cases of enthesitis-related arthritis.
In the sensitivity-related illness model, a patient's genetic predisposition towards illness is compounded by the accumulation of toxicants, including toxic elements77,78 and mycotoxins.79,80 Each toxicant may impact immune system functioning, cumulating in sensitivity towards agents that are typically well-tolerated (such as casein and gluten). In response, autoantibodies form45,78 to tissues including that of the joints and the gut, 81 leading to the presenting symptoms. Mycotoxins 80 and medications 59 alike may be determinants in gut inflammation. Inflammation leads to impairment in absorption of nutrients necessary for healthy immune function and excretion of toxic substances (Table 1), further worsening symptoms.45,46,82,83
Micronutrient deficiencies identified in the patient
Although enthesitis-related arthritis is not usually treated as a sensitivity-related illness, cases of SLE 90 and of polyarticular juvenile idiopathic arthritis 45 have been reported that are either result from, or are resolved through environmental manipulation. While more rigorous study is needed to elucidate the pathways behind the development of enthesitis-related arthritis and to derive consensus conclusions that can be generalized, individual patients may benefit from an environmental medicine approach to their disease. Although one case is insufficient to draw firm conclusions as spontaneous remission is possible, the complete resolution of signs and symptoms occurring within short order after directed interventions were commenced suggests that such an approach warrants further investigation in other patients.
Conclusion
In this case report, a patient with a two-year history of enthesitis-related arthritis experienced a total resolution of symptoms after avoiding certain inciting antigens and correcting her nutritional deficiencies. Although the conventional approach to enthesitis-related arthritis manages to control patient symptoms and maintain function, years of chronic disease and reliance on medications is not ideal if remission is possible with less toxic measures. Enforcing dietary changes and taking required supplements to address specific nutritional deficiencies requires a high level of commitment on the part of patients and their families, but may offer a better quality of life than the current standard of care. Thus, prior to commencing potentially toxic pharmaceutical interventions, the authors suggest that it is reasonable to consider a detailed assessment and remediation of nutritional biochemistry; an eight-week trial of avoidance of common inciting antigens; and exploration and management of any underlying bio-accumulated toxicant load resulting from adverse environmental exposures.
Footnotes
Acknowledgements
None