
Abstract
Objectives
Acute appendicitis is a common surgical condition which can lead to severe complications. Recent work suggested that patients experiencing right lower abdominal pain, with normal white cell count (WCC) and C-reactive protein (CRP) are unlikely to have acute appendicitis and can be discharged. We present two independent datasets that suggest that this strategy may not be risk-free.
Design
Retrospective cohort study of consecutive patients from two district general hospitals. Sensitivity and specificity of CRP, WCC and neutrophil count (NC) in predicting appendicitis were calculated. Markers were analysed using Fisher's exact test and Kruskul-Wallace test.
Setting
Two district general hospitals in the UK.
Participants
Patients undergoing appendicectomy for suspected appendicitis.
Main outcome measures
Inflammatory markers and appendix histology.
Results
A total of 297 patients were included. Appendicitis occurred in four patients with normal CRP, WCC and NC in centre A and 13 patients in centre B. The sensitivity of all three markers combined was 94% (centre A) and 92% (centre B). The specificity was 60% (centre A) and 64% (centre B). No single marker could differentiate uncomplicated and complicated appendicitis, but a raised NC or a CRP >35.5 mg/l predicted complicated appendicitis. CRP, WCC and NC combined differentiated between patients with a normal appendix, uncomplicated appendicitis and complicated appendicitis.
Conclusions
Appendicitis in the presence of normal inflammatory markers is not uncommon. We disagree with the view of Sengupta et al. who suggest that patients with normal WCC and CRP are unlikely to have appendicitis, and recommend that clinicians be wary of normal inflammatory markers in patients with a high clinical suspicion of appendicitis.
DECLARATIONS
JRR's current post is funded through the National Institute of Health Research of the United Kingdom (NIHR). The NIHR had no role in the design, performance, analysis or publication of this study
None
Not applicable
JRR
PGV-S collected dataset B, performed the literature search and wrote the manuscript; JRR offered significant critical contribution to and supervised changes to the manuscript; EB collected dataset A; MH proof-read and offered critical contribution to the final draft manuscript; TP collected additional data for dataset B following recommendations from preliminary peer review
Beryl De Souza
Introduction
Acute appendicitis is a common surgical condition 1 that is readily treated but can lead to complications such as perforation, peri-appendicial abscess, peritonitis, and rarely death.2,3 While traditionally appendicitis was a clinical diagnosis perhaps using raised inflammatory markers to guide the decision-making process, 4 now ultrasonography and most recently computerized tomography (CT) 5 are being employed with increasing frequency to aid diagnosis and to prevent unnecessary surgical intervention. A negative appendectomy rate of up to about 20% has conventionally been accepted to minimize the incidence of perforation and peritonitis associated with a delay in treatment, 6 but some may now consider such rates unacceptable. The increasing availability of CT scans has been associated by some with a decrease in the negative appendicectomy rate with some centres in the United States now reporting rates of less than 2%. 7
However where CT is not immediately available or concerns relating to radiation exposure exist, the clinician will rely on history, clinical examination and blood tests to make a diagnosis and decide whether surgical intervention is warranted. This approach is the basis of the Alvarado score which has been shown to predict appendicitis with relatively high sensitivity and specificity.8–10 The role of inflammatory markers in diagnosing appendicitis has been extensively debated with the stated sensitivity and specificity of C-reactive protein (CRP) ranging from 40–95%, with little consensus on whether white cell count (WCC) is a more sensitive or specific marker than CRP.
A meta-analysis by Andersson11 incorporating 24 studies investigating the role of inflammatory markers in the diagnosis of appendicitis concluded that inflammatory markers themselves are weak discriminators for appendicitis unless combined with clinical findings. However a recent paper by Sengupta et al. 12 reviewed 98 patients presenting with lower abdominal pain and claims to be the first paper to demonstrate a negative predictive value and sensitivity of 100% when CRP and WCC are combined. They conclude that patients with a ‘normal’ WCC (≤11 × 109/l) and CRP (≤10 mg/l), are unlikely to have appendicitis and can be safely sent home. These data are interesting and have significant implications for the management of patients with right iliac fossa pain. If indeed it is the case that CRP and WCC combined are 100% sensitive, many unnecessary admissions, imaging procedures and surgical interventions may be prevented. This paper analyses the preoperative levels of CRP, WCC and neutrophil count (NC) in patients undergoing appendicectomy at two district general hospitals in order to investigate the safety and validity of the approach espoused by Sengupta et al.
Methods
Two series of consecutive patients with a diagnosis of appendicitis were identified retrospectively from hospital databases for the period November 2005 to October 2006 (centre A) and April 2009 to May 2010 (centre B). Patient notes, blood results and pathology reports were examined using the hospital computer systems.
Data were analysed using Microsoft Excel (Microsoft Inc., Seattle, WA, USA) and GraphPad Prism v3.03 (GraphPad Software Inc., La Jolla, CA, USA). Descriptive statistics were derived using Excel and PRISM. Histological information of resected tissue were compared to blood results on admission to ascertain the sensitivity, specificity, positive predictive value and negative predictive value for CRP, WCC and NC. Normal values at our institution were CRP <10 mg/l, WCC <11 × 109/l, and Neutrophil <7.5x109/l. The Kruskul-Wallace Test with Dunn's multiple comparisons was used to compare absolute values of CRP, WCC and NC in patients with findings of a normal appendix, uncomplicated appendicitis and complicated appendicitis (peritonitis, gangrene and/or abscess) while Fisher's exact probability test was used to compare the proportions of patients with normal or raised inflammatory markers with or without appendicitis.
Results
One hundred and eighteen patients underwent appendicectomy at centre A and 200 at centre B in the respective study periods. Twenty-one patients were excluded because of incomplete data or an alternative diagnosis to appendicitis. Demographic data and data from histopathology reports are displayed in Table 1.
Demographic and histopathological data of both datasets
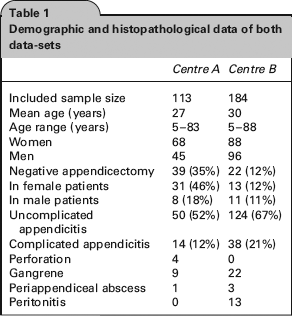
In centre A, appendicitis in the presence of normal CRP or normal WCC or normal NC occurred in 24, 22 and 15 patients, respectively. Appendicitis in the presence of normal CRP and normal WCC and normal NC occurred in four patients. In centre B, appendicitis in the presence of normal CRP or normal WCC or normal NC occurred in 50, 47 and 36 patients, respectively. Appendicitis in the presence of normal CRP and normal WCC and normal NC occurred in 13 patients.
The negative appendicectomy rate defined by histological assessment was 35% in centre A and 12% in centre B. The centre A cohort comprised a greater proportion of female patients who themselves had a negative appendicectomy rate of 46%. In patients with a histologically normal appendix (n = 61), inspection of operation notes, imaging and discharge summaries revealed that appendicitis was recorded as the intraoperative finding in 45 patients, while ovarian cyst (n = 2), mesenteric adenitis (n = 2), Crohn's disease (n = 1), band adhesion (n = 1), urinary retention (n = 1), retrograde menorrhagia (n = 1) and nonspecific abdominal pain (n = 8) were recorded as diagnoses for the remaining patients. There was no significant difference between the proportion of patients with histologically normal appendixes given the diagnosis appendicitis between centres A and B (n = 29, n = 11, P = 0.1).
The sensitivity, specificity, positive predictive values and negative predictive values for appendicitis are given in Table 2. These data, particularly those from centre B, demonstrate a moderate sensitivity but a poor specificity and negative predictive value.
Diagnostic attributes of tests in distinguishing normal from abnormal appendices, values shown are percentages

PPV = positive predictive value, NPV = negative predictive value, LR+ = likelihood ratio that individual has appendicitis, LR- = likelihood ratio that individual does not have appendicitis
Odds ratios were calculated for the three inflammatory markers individually and in combination (Table 3). This shows that in centre A, a patient with all three inflammatory markers raised is 7.13 (95%CI 2.28-22.32) times more likely to have appendicitis than a patient with at least one normal inflammatory marker and up to 44 (95%CI 9.93-194.93) times more likely than a patient with completely normal inflammatory markers.
Odds ratios and 95% confidence intervals for appendicitis based on categorical test results. ‘≥1 marker raised’ indicates at least 1 normal inflammatory marker, while ‘All normal’ indicates normal CRP and normal WCC and normal NC

With both datasets combined, Kruskul-Wallace test analysis of absolute values for WCC and NC demonstrated statistical significant difference in CRP, WCC and NC between patients in the three categories: normal appendix; uncomplicated appendicitis; and complicated appendicitis (Figure 1, Table 4). However, testing with Dunn's multiple comparisons demonstrates that no marker can significantly differentiate uncomplicated and complicated appendicitis. When used as categorical variables (i.e. marker raised or normal), Fisher's exact test demonstrates that NC, but not CRP or WCC has some ability to predict complicated appendicitis. A recursive approach indicated that CRP >35.5 mg/l or above could predict complicated appendicitis (P = 0.0366). However no WCC cut-off was found to predict complicated appendicitis.

Graph of mean (Dark circle) and standard deviation (Error bars) of absolute CRP (mg/l), WCC (x 109/l) and NC (x 109/l) for A) Patients with a histologically normal appendix, B) Patients with uncomplicated appendicitis and C) Patients with complicated appendicitis
Inflammatory markers versus appendicitis and complicated appendicitis. Kruskal-Wallis test was used with Dunn's multiple comparison to compare absolute values of inflammatory markers. Fisher's exact test was used to compare proportions of patients in each group with high CRP (>10 mg/l), WCC (>11 × 109) and NC (>7.5 × 109), respectively

Discussion
Principal findings
This paper demonstrates that contrary to the findings of Sengupta et al. patients with normal inflammatory markers can still have appendicitis. In our two independent datasets this happens with some frequency, with 5% and 8% of patients with appendicitis having normal CRP, WCC and NC on admission. We have shown, however, that CRP, WCC and NC are statistically associated with appendicitis and that CRP (>35.5 mg/l) and raised NC can predict complicated appendicitis. Our data show that a combination of all three markers gives a greater sensitivity than each marker individually suggesting that using all three markers will offer the clinician greatest guidance but normal values for CRP, WCC and NC on admission cannot be absolutely reassuring.
Strengths and weaknesses of study
It is well-known that inflammatory markers increase in appendicitis and this paper confirms this. However this paper looks only at those undergoing appendicectomy which, given the high clinical suspicion of appendicitis, results in an artificially high positive predictive value and low negative predictive value. However, when our data (sensitivity 94% and 92% and negative predictive value 85% and 52%) are compared to those of Sengupta et al who reported both a sensitivity and negative predictive value of 100% we were not able to replicate these in two independent datasets. Therefore we have shown that in two independent cohorts of patients with a high clinical suspicion of appendicitis (i.e. who underwent appendicectomy) the negative predictive value of CRP, WCC and NC is poor and that patients with a clinical history and examination consistent with appendicitis but normal inflammatory markers should not be discharged.
Comparison with other published data
Papers investigating the role of inflammatory markers in appendicitis date back as far as 194713 and our data concur with the majority of studies that have been published to date. The major challenge when comparing studies in this area is patient selection and cut-off values for the markers of inflammation. The cut-off values are rarely consistent and reported sensitivities and specificities for both CRP and WCC vary widely as reported in a meta-analysis by Hallan and Asberg. 14 Furthermore there is little consensus on whether either CRP or WCC is a better marker than the other. The sensitivities and specificities calculated in this study are similar to those previously reported (Tables 5 and 6). Our results when combining inflammatory markers support those reported by Birchley who demonstrates a sensitivity and specificity of 94% and 56% for CRP, WCC and NC. 15 Our results and those of Birchley do not support the finding of Sengupta et al., that combined CRP and WCC are 100% sensitive for appendicitis, a finding also reported in 1989 by Dueholm et al. 16 The meta-analysis by Anders-son11 found that where all markers of inflammation were normal, the negative likelihood ratio is less than 0.10, but not zero, indicating that appendicitis is still possible with normal inflammatory markers. Finally, we demonstrate a negative appendicectomy rate of 39% and 12% in our two datasets which is considerably higher than recent published data. 17 Negative appendicectomy rate has decreased considerably over the last 20 years7,17 and this may, in part, account for the difference to published data and between our two datasets. In addition, the greater proportion of female patients in dataset A, who offer a greater diagnostic challenge, may also contribute to a higher negative appendicectomy rate. 18

RIF = right iliac fossa
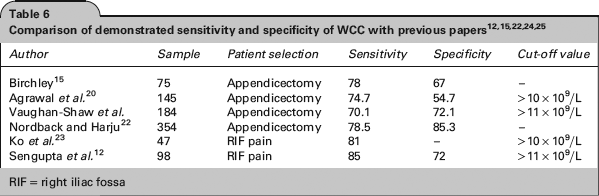
RIF = right iliac fossa
Implications for practice
Appendicitis is a common surgical condition that requires prompt treatment. When treatment is delayed development of gangrenous appendicitis, perforation, or peri-appendicular abscess may occur. 19 Sengupta et al. concluded in their abstract that ‘patients experiencing lower abdominal pain, with normal white cell count and CRP are unlikely to have appendicitis and can be safely sent home’. We feel that this strategy may not be without risk to patients who have normal inflammatory markers. Appendicitis is an inflammatory process which may be associated with normal inflammatory markers at an early stage and it may be these cases which we have identified. A weakness of our study is that we have no data on the interval from onset of symptoms to measurement of inflammatory markers or to time of surgical procedure. Individuals may now present at an earlier stage in the development of appendicitis because of easier access to healthcare or changes in the provision of health-related information (e.g. the Internet). If this is the case normal admission blood results may become a more common phenomenon and serial examination, repeat blood testing or greater use of imaging is likely be employed before undertaking surgical intervention. The availability and use of imaging should also reduce negative appendicectomy rates.
Conclusions
This paper demonstrates that patients with normal inflammatory markers can still have appendicitis which is in contrast to the conclusions of a recent publication. 12 We believe that the diagnosis of appendicitis remains a multifactorial process and should still rely on clinical suspicion even if inflammatory markers are normal. In patients where there is clinical doubt there should be a prompt and appropriate use of imaging modalities or surgery.
Future research
The ultimate goal must be that patients with appendicitis receive timely surgical intervention, while patients without appendicitis avoid unnecessary surgery. In addition exposure to ionizing radiation must be avoided wherever possible. Further work is required to define a clear pathway from presentation to investigation and operation. This would require the relationship of symptom duration and inflammatory markers to be more clearly understood and standardized indications for ultrasound and CT to be decided and disseminated.
Footnotes
Acknowledgements
C Richardson conceived the collection of dataset B