
Abstract

Intravenous white spirit injection is a rarely documented event that can cause potentially fatal respiratory collapse and abscess formation.
DECLARATIONS
None declared
None
Written informed consent to publication has been obtained from the patient
CM
Both authors contributed equally
Christoph Pechlaner
Case report
A 40-year-old man was admitted from the emergency department with pleuritic chest pain. Severe anterior pain developed 10 min after the deliberate injection of 10 mL of white spirit intravenously into his left median cubital vein, in a suicide attempt. The patient had a past history of psychiatric illness and intravenous drug abuse. Symptoms began with an almost instant cough and he subsequently developed acute anterior chest pain, worse on deep inspiration. The patient waited 15 hours prior to taking any pain killers and only achieved minimal transient relief with ibuprofen.
Loss of analgesic effect precipitated hospital attendance. Initial blood pressure was 121/78 mmHg, heart rate was 130 beats per minute, pulse oximetry was 90% on air. Physical examination was generally unremarkable with some reduction in breath sounds bilaterally. There was no tenderness to palpation. Laboratory findings on venous blood sampling revealed WCC 11.8 × 109/L, neutrophils 9.3 × 109/L with arterial blood gas demonstrating a p02 of 51.7 mmHg (FiO2 0.21) improving to 57.7 mmHg with administration of supplementary oxygen. Diffuse bilateral patchy opacification was reported in both lung fields on chest X-ray (Figure 1). While still in the emergency department a CT pulmonary angiogram (Figure 2) demonstrated multifocal peripheral bilateral air space consolidation and no pulmonary embolism.
Chest X-ray showing diffuse bilateral patchy opacification in both lung fields
CT pulmonary angiogram showing multifocal peripheral bilateral air space consolidation and no pulmonary embolism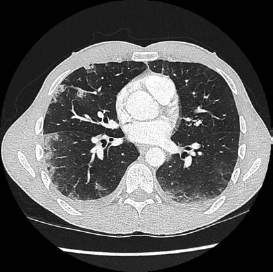
The patient remained clinically stable although he was diaphoretic, tachycardie with some residual pleuretic chest pain which responded well to intramuscular morphine. Oxygenation improved and 32 hours post initial insult repeated arterial blood gases showed p02 89.5 mmHg (FiO2 of 0.28). Chest X-rays taken over subsequent days showed increased right middle lobe shadowing superimposed on the previously noted bilateral patchy opacification. He was treated with analgesics, antibiotics and subsequently discharged on a course of oral prednisolone 30 mg once daily until follow-up. Follow-up was planned for one month.
During his admission he developed an increasing tender erythamatous swelling in the soft tissue surround the long head of the left tricep, the site of injection. This developed into an abscess and was successfully treated with surgical incision and drainage.
At one month follow-up the patient had completed a period of psychiatric treatment and returned to work. There were no reported residual respiratory problems and the injection site abscess had fully healed. There was no residual phlebitis in the left arm. Blood tests did not demonstrate any abnormality or organ damage. He was discharged from further follow-up with the steroids to be tapered then stopped. No further medical treatment was planned.
Discussion
White spirit, also known as Stoddard solution, is a transparent, paraffin-derived, low viscosity, volatile, hydrocarbon-based liquid. Used mainly as a solvent in the painting and decorating industry, it has also been used in wood preservatives and as a cleaning and degreasing solvent. Derived from the fractional distillation of petroleum it is composed of hydrocarbons, flammable and easily vaporized. Toxic exposure is usually seen following ingestion and subsequent aspiration. There are some documented cases of local tissue destruction resulting in amputation when accidentally injected into soft tissue. 1 Reported cases of intravenous injection of hydrocarbons are rare and we believe this to be the first documented case in the United Kingdom and only the second documented case of intravenous white spirit injection.2–4
This patient presented via the Accident and Emergency department and was admitted under general medicine. No emergency medicine or critical care physician on duty had ever previously seen such a case. Further information on management was sought from the primary clinical toxicology database of the National Poisons Information Service, Toxbase, but other than advocating supportive treatment advice was limited. A poisons centre was not contacted directly and the decision was taken to treat supportively.
The most serious complication following aspiration of hydrocarbons is usually pneumonia; this case, however, confirms a direct toxic effect on lung tissue when intravenously exposed to hydrocarbons. The first major capillary bed to be exposed following intravenous injection is that of the pulmonary vasculature. Previous cases have been based on the intravenous injection of other hydrocarbon-based liquids, kerosene and gasoline. It has been suggested that that the mechanism of pulmonary injury is due to endothelial injury by the hydrocarbon molecule becoming deposited in the pulmonary capillary bed. 3 The lungs are the most frequently reported organ being damaged and the associated chemical pneumonitis has been attributed to the direct toxic effect and not that of superimposed infection.3,5 The first suspected pathology in this case was that of pulmonary embolism although this was highly unlikely given that there was a known substance administered by a confirmed route and was subsequently quickly excluded following imaging.
Other organs including the heart and brain can be affected with patients presenting with either arrhythmia or convulsions.3,5,6 Patients almost always have chest pain and frequently have haemoptysis and dyspnoea which may erroneously lead to an associated or differential diagnosis of pulmonary embolism although there are no reported cases of intravenous hydrocarbon resulting in pulmonary embolism. Death has been reported with volumes as small as 5 mL due to severe lung injury despite patients receiving cardiovascular and respiratory support in an intensive care setting. 5
Patients most likely to suffer hydrocarbon poisoning from intravenous administration are men with psychiatric histories that also have a history of intravenous drug abuse. It is frequently associated with attempted suicide as was the situation in this case.3,6
Presently there are no current national or international guidelines to support either antibiotic or steroid treatment in relation to the side-effects associated with intravenous hydrocarbon injection. Due to the rarely reported nature of the illness little information is widely available. Of the reported cases such as this, management has generally been supportive and no specific medication at the time of presentation has been identified as improving prognosis. At the time of writing there is no known antidote. Should superimposed infection develop this should be treated with antibiotics. As occurred in this case, abscesses can develop at the injection site and phlebitis may also be seen.
Conclusions
This case demonstrates that intravenous injection of the hydrocarbon white spirit can induce acute lung injury and abscess formation at the injection site. Our case improved with supportive care.
Footnotes
Acknowledgements
None