
Abstract
We report a case on a 12-year-old child with chyluria and Noonan's syndrome in whom lymphoscintigraphy demonstrated lymphatic communications within the urinary tract.
DECLARATIONS
None declared
None
Written consent to publication has been obtained from the patient or next of kin
SG
All authors contributed equally
Donald Stanley
Case report
A 12-year-old boy with phenotypic characteristics of Noonan's syndrome who previously in 1997 underwent surgery for pulmonary stenosis, presented with a two-week history of passing ‘whitish-coloured urine’. This was biochemically and cytologically confirmed as chyluria but occasional red blood cells and mature reactive lymphocytes were also detected in the urine.
From the age of 4 years he presented with intermittent short episodes of chyluria with spontaneous regression of symptoms following each episode. When his chyluria became protracted over a two-week period, however, he was referred for lymphoscintigraphy.
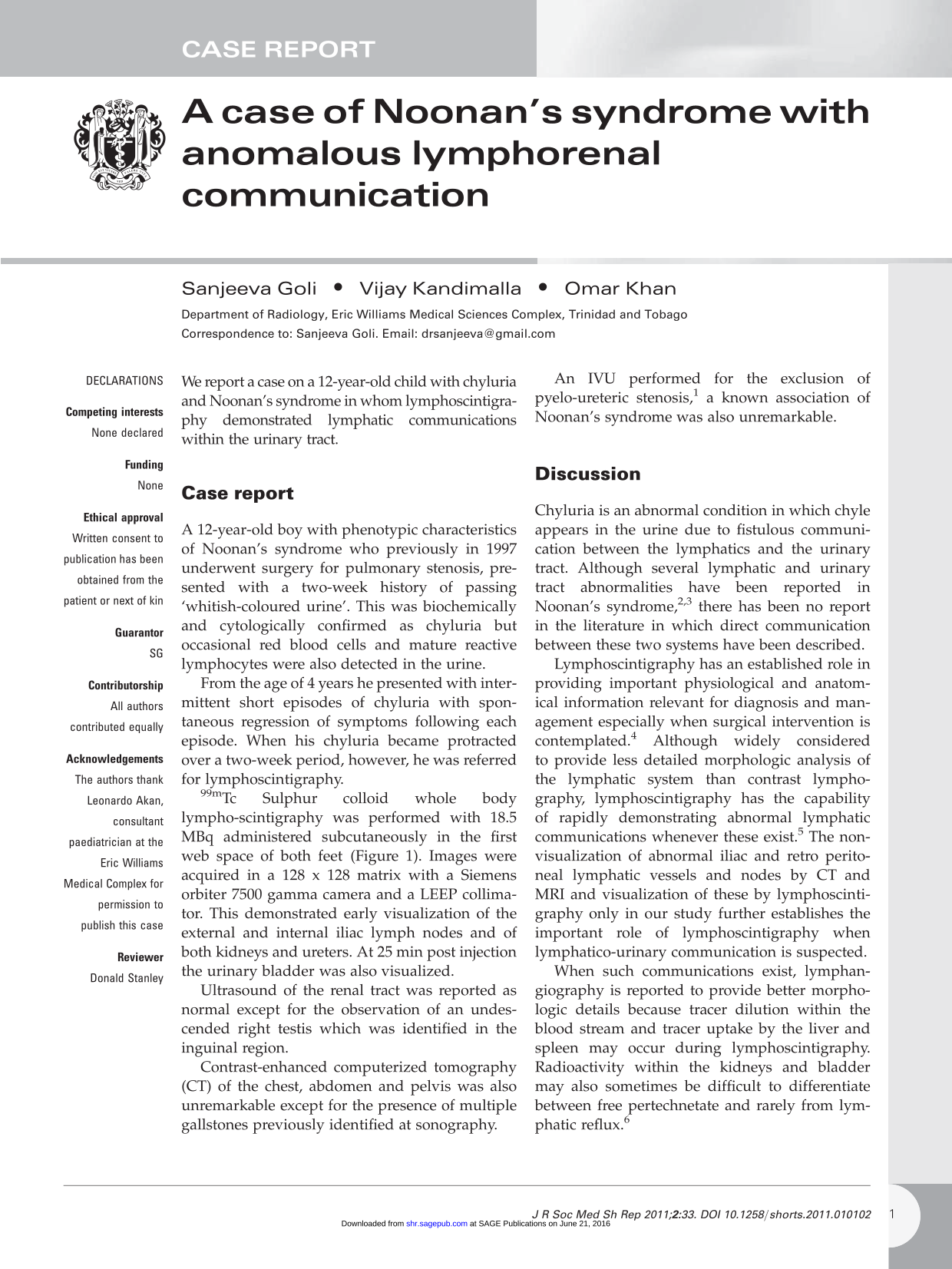
99mTc Sulphur colloid whole body lymphoscintigraphy was performed with 18.5 MBq administered subcutaneously in the first web space of both feet (Figure 1). Images were acquired in a 128 × 128 matrix with a Siemens orbiter 7500 gamma camera and a LEEP collimator. This demonstrated early visualization of the external and internal iliac lymph nodes and of both kidneys and ureters. At 25 min post injection the urinary bladder was also visualized.
Sequential images of bilateral lower limb 99m Tc Sulphur colloid lymphoscintingraphy obtained at 5-min intervals demonstrate visualization of inguinal lymph nodes at 10 min, activity within both kidneys at 15 min and bladder activity at 25 min
Ultrasound of the renal tract was reported as normal except for the observation of an undescended right testis which was identified in the inguinal region.
Contrast-enhanced computerized tomography (CT) of the chest, abdomen and pelvis was also unremarkable except for the presence of multiple gallstones previously identified at sonography.
An IVU performed for the exclusion of pyelo-ureteric stenosis, 1 a known association of Noonan's syndrome was also unremarkable.
Discussion
Chyluria is an abnormal condition in which chyle appears in the urine due to fistulous communication between the lymphatics and the urinary tract. Although several lymphatic and urinary tract abnormalities have been reported in Noonan's syndrome,2,3 there has been no report in the literature in which direct communication between these two systems have been described.
Lymphoscintigraphy has an established role in providing important physiological and anatomical information relevant for diagnosis and management especially when surgical intervention is contemplated. 4 Although widely considered to provide less detailed morphologic analysis of the lymphatic system than contrast lymphography, lymphoscintigraphy has the capability of rapidly demonstrating abnormal lymphatic communications whenever these exist. 5 The nonvisualization of abnormal iliac and retro peritoneal lymphatic vessels and nodes by CT and MRI and visualization of these by lymphoscintigraphy only in our study further establishes the important role of lymphoscintigraphy when lymphatico-urinary communication is suspected.
When such communications exist, lymphangiography is reported to provide better morphologic details because tracer dilution within the blood stream and tracer uptake by the liver and spleen may occur during lymphoscintigraphy. Radioactivity within the kidneys and bladder may also sometimes be difficult to differentiate between free pertechnetate and rarely from lymphatic reflux. 6
Although the most common cause of chyluria worldwide is due to Wuchereria bancrofti, nonparasitic chyluria may also arise due to thoracic duct stricture or direct injury. The mechanism for communication between the urinary tract and the lymphatics in Noonan's syndrome is poorly understood although several anomalies of the lymphatic system have been reported in this condition. These include lymphoedema, pulmonary lymphagectasis, intestinal and testicular lym-phangiectasis, cystic hygroma, chylothorax and lymphatic dysplasia of the lip. 3 Lymphatic dysplasia/hypoplasia has also been reported in 15-20% of patients with Noonan's syndrome. 7 This condition has been linked to mutations in PTPN11 encoding the protein tyrosine phosphatase SHP-2 in more than 50% of cases studied. It has been postulated that the pathogenesis of this syndrome may arise from SHP-2 activity but genetic heterogeneity has also been recorded. 8
Recognized radiological manifestations include: hypoplastic peripheral lymphatic vessels; hypoplastic lymph nodes; chylothorax and pulmonary lymphangiectasia. 9 When obstructive lymphatic changes are present collateral formation in the retroperitoneal, mediastinal and cervical lymphatics 3 has been observed. Urinary tract abnormalities including obstructive uropathy secondary to pyeloureteral stenosis duplication of the collecting system, renal hypoplasia and polycystic renal disease have also been described in Noonan's syndrome. An IVU and micutrating cystography performed to exclude urinary tract anomalies and vesico ureteric reflux were both normal in our study.
Although not considered to be life-threatening, at least 50% of cases of chyluria are reported to resolve spontaneously. 10 Recognized methods of treatment include sclerotherapy 10 somatostation therapy 11 and lymphatic microsurgery, but none of these management protocols were employed as the patient's chyluria spontaneously resolved over a one-month period following presentation. The principal aim when surgery is contemplated is to identify the site of lymphatic obstruction and to detect any co-existing lymphatic collaterals and to preserve the latter. 12 Although lymphangiography is the ‘gold’ standard for the visualization of the lymphatic system the technique requires expertise for cannulation and significant radiation exposure can result. 13 As accurate anatomical detail is often not provided by lymphoscintigraphy lymphangiography may be considered if surgery is contemplated. 14 We did not attempt lymphangiography in this patient, as the specified equipment required for the procedure does not exist at our institution. In recent years lymphoscintigraphy has essentially replaced lymphangiography. In most clinical situations lymphoscintigraphy has been reported to provide adequate and even additional information in the evaluation of congenital lymphatic abnormalities. It is less time-consuming, non-invasive, reproducible and is associated with less radiation exposure compared to lymphangiography. This case provides supportive evidence for its clinical utilization when chyluria is suspected, as it was able to readily demonstrate 99mTc labeled colloid within iliac nodes and thereafter within the kidneys and urinary bladder.
Footnotes
Acknowledgements
The authors thank Leonardo Akan, consultant paediatrician at the Eric Williams Medical Complex for permission to publish this case