
Abstract
Erythema ab igne, a skin reaction which follows heat exposure, is characteristically associated with pancreatic malignancy but unusually in this case was a presenting sign of colorectal cancer.
DECLARATIONS
None declared
None
Written informed consent to publication has been obtained from the patient or next of kin
RB
All authors contributed equally
Kingsley Ekwueme, Sanjay Chaudhri
Case report
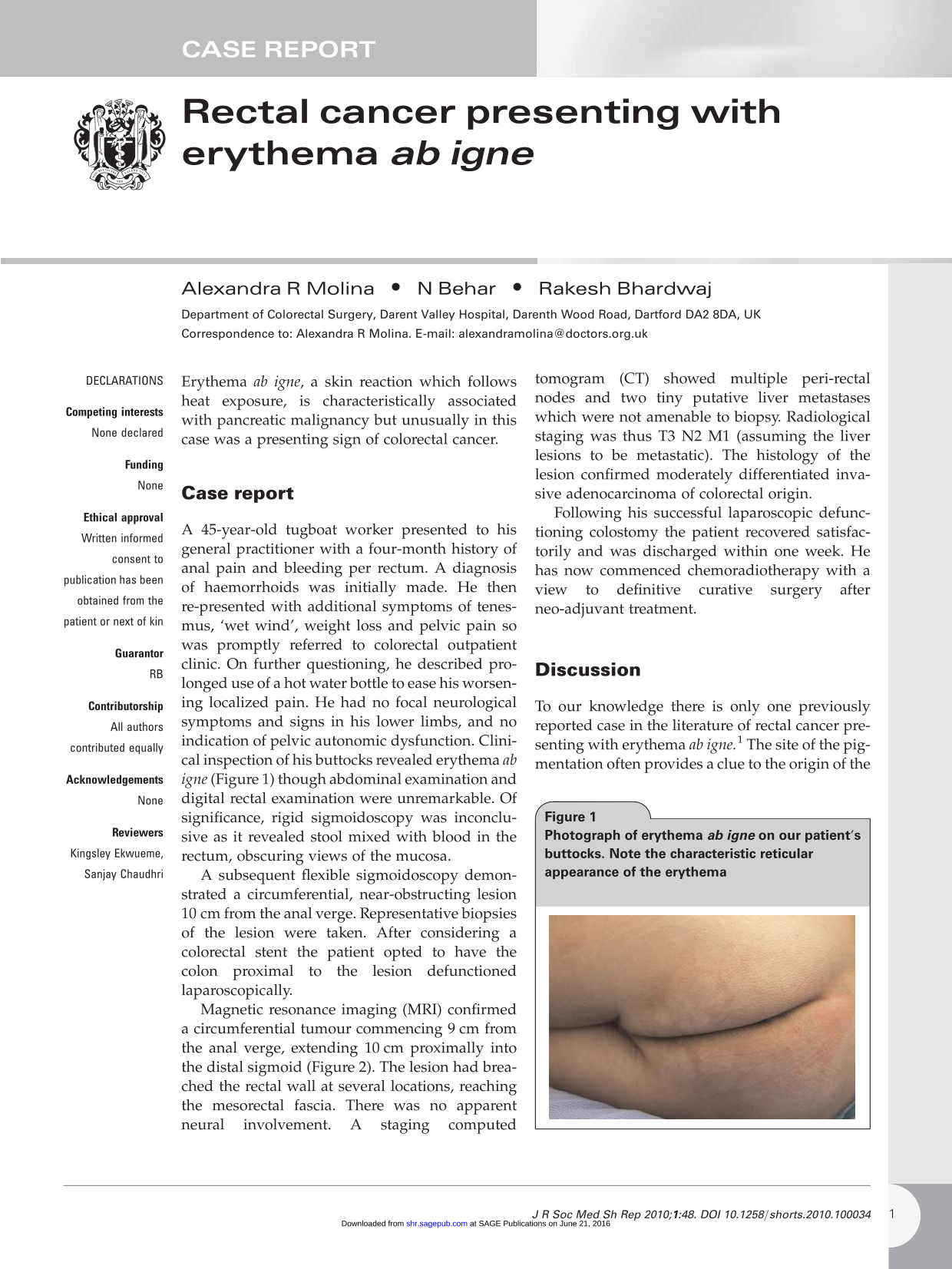
A 45-year-old tugboat worker presented to his general practitioner with a four-month history of anal pain and bleeding per rectum. A diagnosis of haemorrhoids was initially made. He then represented with additional symptoms of tenesmus, ‘wet wind’, weight loss and pelvic pain so was promptly referred to colorectal outpatient clinic. On further questioning, he described prolonged use of a hot water bottle to ease his worsening localized pain. He had no focal neurological symptoms and signs in his lower limbs, and no indication of pelvic autonomic dysfunction. Clinical inspection of his buttocks revealed erythema ab igne (Figure 1) though abdominal examination and digital rectal examination were unremarkable. Of significance, rigid sigmoidoscopy was inconclusive as it revealed stool mixed with blood in the rectum, obscuring views of the mucosa.

Photograph of erythema ab igne on our patient's buttocks. Note the characteristic reticular appearance of the erythema
A subsequent flexible sigmoidoscopy demonstrated a circumferential, near-obstructing lesion 10 cm from the anal verge. Representative biopsies of the lesion were taken. After considering a colorectal stent the patient opted to have the colon proximal to the lesion defunctioned laparoscopically.
Magnetic resonance imaging (MRI) confirmed a circumferential tumour commencing 9 cm from the anal verge, extending 10 cm proximally into the distal sigmoid (Figure 2). The lesion had breached the rectal wall at several locations, reaching the mesorectal fascia. There was no apparent neural involvement. A staging computed tomogram (CT) showed multiple peri-rectal nodes and two tiny putative liver metastases which were not amenable to biopsy. Radiological staging was thus T3 N2 M1 (assuming the liver lesions to be metastatic). The histology of the lesion confirmed moderately differentiated invasive adenocarcinoma of colorectal origin.

Sagittal MRI image showing the rectal tumour commencing approximately 9 cm from the anal verge and extending 10 cm proximally into the distal sigmoid colon.
Following his successful laparoscopic defunctioning colostomy the patient recovered satisfactorily and was discharged within one week. He has now commenced chemoradiotherapy with a view to definitive curative surgery after neo-adjuvant treatment.
Discussion
To our knowledge there is only one previously reported case in the literature of rectal cancer presenting with erythema ab igne. 1 The site of the pigmentation often provides a clue to the origin of the pain – for example, patients with pancreatic cancer may present with erythema ab igne on the anterior abdominal wall,1,2 and a patient with myeloma was reported to have exhibited erythema ab igne on her back. 1 The primary tumour or metastases may both give rise to the pain leading to repeated topical heat application.
In other circumstances erythema ab igne may be indicative of a local heat source. Elderly patients classically present with erythema ab igne on their shins as they expose their legs to absorb the heat from fires. More recent reports have described erythema ab igne on the anterior aspects of the thighs from direct contact with the heat from laptop computers. 3
However, when seen in an unusual anatomical location, it is important to remember that erythema ab igne is an alarming sign which should prompt rapid clinical investigation.1,2 In this case our patient described accompanying symptoms which alone may not have been sufficient to prompt urgent investigation, but, when evaluated together with the erythema ab igne and pelvic pain, compounded to produce a very concerning clinical picture.
Footnotes
Acknowledgements
None