
Abstract
Objectives
Older patients with carpal tunnel syndrome who are resistant to conservative treatment often have a less than satisfactory outcome after surgery. We therefore investigated whether the age of the patient affects the subjective complaints or the objective severity of the nerve entrapment prior to surgery in patients younger than 40 years compared with those above 70 years of age.
Design
Prospective study.
Setting
NHS specialist neurophysiology department.
Participants
One hundred and six splint-resistant patients scored their subjective complaints and scores were then compared with the neurophysiology results.
Main outcome measures
Nerve conduction speeds and subjective visual analogue score of pain, sensation and motor function.
Results
Conduction speeds were significantly more affected in patients over 70 years of age than in those under 40 years. Older patients scored their subjective complaints lower than younger patients.
Conclusions
Older patients’ subjective complaints misrepresent the severity of the nerve entrapment. Clinicians should have a lower threshold for objective investigation of patients older than 70 years of age to minimize development of irreversible nerve damage.
Introduction
Carpal tunnel syndrome is common in the general population with approximately 1% incidence but can often be treated with simple night wrist splints. 1 For those patients who do not respond satisfactorily to conservative measures a surgical decompression is often able to alleviate the patient's complaints. 2 However, some investigators have reported that older patients can have a less satisfactory outcome after surgery 3 though this impression is not universally shared.4,5 As we routinely confirm the diagnosis with nerve conduction studies (NCS) prior to surgical treatment we had developed an impression that older patients had more severe compression but had less subjective complaints. Our experience with younger patients is that many of these often have severe clinical complaints preoperatively though these are rarely confirmed from the NCS. The purpose of this prospective study was, therefore, to investigate the relationship between the severity of the subjective complaints and the severity of the NCS findings in patients below the age of 40 years and those patients over 70 years with neurophy-siologically confirmed carpal tunnel syndrome who had not responded to conservative treatment. We are not aware that such a study has previously been published.
DECLARATIONS
None declared
None
Guy's and St Thomas’ NHS Foundation Trust Research Ethics Committee
BP
BP designed the study; KA and MK performed the nerve conduction studies, collected and analysed the data; BP, KA and MK wrote the paper
Christopher Kearsey
Patients and methods
We analysed prospectively collected clinical and neurophysiological data from consecutive patients with clinical signs of carpal tunnel syndrome, 6 who were referred for NCS as part of their pre-surgical assessment. Patients were offered enrolment in the study if they had not been satisfactory managed by night splints 7 and the NCS provided objective confirmation of carpal tunnel syndrome. We aimed for a total study group of a minimum 100 patients with at least 30 participants in the groups below 40 years of age and above 70 years of age. On the day of the NCS and immediately before the test, patients were asked to self-assess the severity of their symptoms using a slightly modified version of the Boston questionnaire 8 in which they scored their sensory symptoms (numbness, tingling and loss of sensation, and wrist pain) on a VAS scale 0–10. Patients with neurological symptoms and signs suggestive of widespread peripheral neuropathy (such as sensory symptoms in the lower limbs and depressed or absent tendon reflexes) were excluded from the study. Patients with diabetes were only included if they had localized median nerve entrapments with normal ulnar motor and sensory conduction and normal for age sural sensory potential.
NCS methodology
Our standard carpal tunnel syndrome protocol includes distal motor latencies (DML) to the abductor pollicis brevis and abductor digiti minimi, motor conduction velocities and F waves, and orthodromic or antidromic distal sensory latencies (DSL) (wrist – F2/F5) for the median and ulnar nerves bilaterally. When these tests are inconclusive in patients with clinical symptoms of carpal tunnel syndrome, the second lumbrical-interosseous technique (2-LINT) test and orthodromic mid palm to wrist times for the median and ulnar nerves are obtained to detect possible incipient median nerve compression. Hand temperature is routinely kept above 30°C. NCS results were graded on a scale of 0-6 according to the following severity scale: incipient to mild carpal tunnel syndrome (grades 1-2): slow median DSL, normal DML (<4.1 ms); moderate carpal tunnel syndrome (grade 3): preserved median sensory potentials (SNAP), prolonged DML but <6.5 ms; severe carpal tunnel syndrome (grade 4): absent SNAP, DML <6.5 ms; very severe carpal tunnel syndrome (grades 5 and 6): absent SNAP, DML >6.5 ms or absent.
Statistics
Non-parametric characteristics were compared using two-tailed Mann-Whitney U Test. Nominal clinical characteristics were analysed by Chi-square test with Yates’ correction. Statistical significance was set at p <0.05.
Ethical approval was obtained from the local ethics committee.
Results
There were 106 consecutive patients with symptoms consistent with carpal tunnel syndrome and confirmatory NCS findings. For the purpose of clarity we have not included the results in the middle-age group (>40- < 70). Table 1 shows the results of the NCS in all patients and separately in the younger (≤40 years) and the older (≥70 years) patients, and how these two groups compare with regard to severity of the NCS findings and of the subjective sensory symptoms. All patients of the younger and older groups complained of sensory symptoms (numbness and pins and needles) and completed the relevant severity scale (VAS 0-10). However, only 18 of the 34 patients of the older age group and 22 of the 30 younger patients reported wrist pain and completed their pain VAS scale. To avoid small groups we distinguished these patients: (a) in terms of objective NCS severity (grades 1-6) into incipient or mild carpal tunnel syndrome (grades 1 and 2; 15 patients) and moderate to severe carpal tunnel syndrome (grades 3-6; 44 patients); and (b) in terms of subjective sensory complaints, into intense (VAS >5/10; 33 patients) and milder symptomatology (VAS ≤5/10; 26 patients).
Nerve conduction findings and subjective sensory complaints in the younger and the older patients with carpal tunnel syndrome
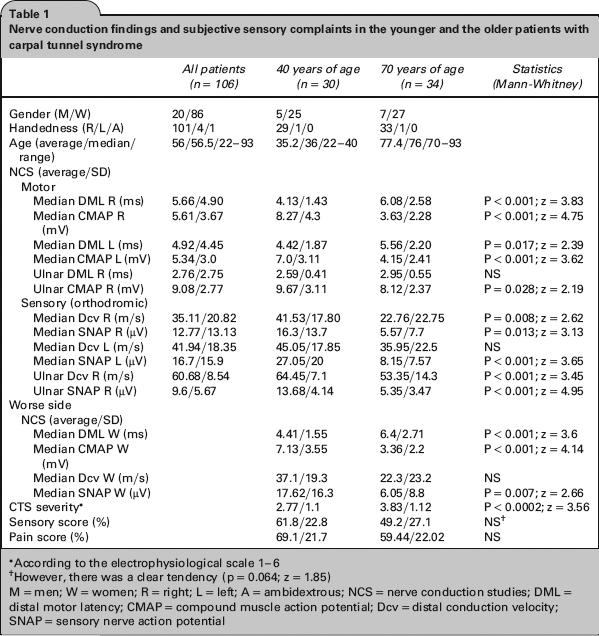
According to the electrophysiological scale 1-6
However, there was a clear tendency (p = 0.064; z = 1.85)
M = men; W = women; R = right; L = left; A = ambidextrous; NCS = nerve conduction studies; DML = distal motor latency; CMAP = compound muscle action potential; Dcv = distal conduction velocity; SNAP = sensory nerve action potential
Tables 2 and 3 show the relationships between NCS severity and the severity of sensory symptoms and wrist pain, respectively, in the younger and older patient groups. Patients with clinically severe carpal tunnel syndrome (sensory symptoms or wrist pain VAS more than 5) were less likely to have incipient or mild carpal tunnel syndrome on neurophysiological grounds if they were ≥70 years of age (Chi square: P = 0.004 and P = 0.017, respectively), and those with milder clinical expression were more likely to have neurophysio-logically severe carpal tunnel syndrome, again if they were in the older age group (Chi square: P = 0.013 and P = 0.055, respectively). In the age group ≤40 years, there was no correlation between severity of subjective symptoms and NCS severity of carpal tunnel syndrome; even VAS scores above 5 could be associated with mildly abnormal NCS (grades 1 and 2).
Intensity of wrist pain vs. NCS severity in younger and older patients

Patients with scores higher than 5/10 (>50%) on the VAS sensory scale
p = 0.017
Patients with scores 5/10 or lower (≤50%) on the VAS sensory scale
p = 0.055
For the NCS severity grades 1-6, see the Methods section in the main text
Intensity of sensory (numbness and paraesthesia) symptoms vs. NCS severity in younger and older patients

Patients with scores higher than 5/10 (>50%) on the VAS sensory scale
p = 0.004
Patients with scores 5/10 or lower (≤50%) on the VAS sensory scale
p = 0.013
Four patients in the ≤40 group and 10 in the ≥70 group had unilateral subjective complaints. In the younger group, three had normal NCS in the asymptomatic hand and only one had NCS-confirmed bilateral carpal tunnel syndrome (grade 3 on the ‘normal’ side). In contrast, only three patients in the ≥70 group had normal NCS in their asymptomatic hand and, therefore, truly unilateral carpal tunnel syndrome; the remainder seven had NCS-confirmed bilateral carpal tunnel syndrome (grade 1 in three patients, grade 3 in three patients and grade 4 in one patient).
Discussion
The results in this study support our hypothesis that older patients with carpal tunnel syndrome resistant to conservative treatment have more severe nerve compression than younger patients, as extrapolated from the NCS results. It could be argued that such an extrapolation did not take into account the lowering of conduction speed as a natural result of age by itself as reported by Tanosaki et al. 9 However, routine NCS in carpal tunnel syndrome do not make allowance for an effect of age, and indeed practice parameters and guidelines 6 do not include correction of the elec-trodiagnostic results for age; we certainly concur as the lowering in conduction speed between the 20–29-year age group compared with the 70–79 years group in the study of Tanosaki et al. was only in the range of 5%. We found a difference in mean distal median conduction speed of around 45% between our younger and older age groups (41.53 m/s and 22.76 m/s, respectively, Table 1), which is almost three times bigger than the mean difference in ulnar sensory distal speed (64.45 m/s and 53.35 m/s, respectively; difference 17%, Table 1) and nine times bigger than those of Tanosaki et al. 9 This would, therefore, suggest that other causes should be sought to explain these profound changes, which cannot be explained by natural ageing. It could be argued that the severity in the older age group was made worse by the delay in investigation as all these patients had had a trial of treatment with wrist splints, which had not been successful. However, this seems unlikely as a recent study by Nobuta et al. 10 showed that in the group of patients where the splints did not improve the clinical presentation after five months of unsuccessful treatment this additional period did not lead to a further reduction of the conduction speed. These authors found that those patients with the most severely affected conduction speed were least likely to be satisfied with splint treatment, and due to a possible negative selection this could have left the older participants in our study to have relatively more severe compression. However, the nerve compression severity as found by NCS results within our older group is comparable to that found by Townshend et al. 11 in their similarly aged group, although these investigators did not have any younger patients included for comparison. We are, therefore, left to search for the reason why older patients with carpal tunnel syndrome have more severe compression than younger patients. One such reason could be that older patients have an age-related sensory impairment that makes them less aware of the clinical symptoms. Indeed studies on pain perception suggest that there is reduced pain sensitivity with age, 12 which is possibly due to a reduction of the nerve membrane excitability as an age-related factor, and may delay the older patient from seeking treatment at an earlier and less severe stage of the compression; such delay would result in a more severe compression being electrophysiologically diagnosed when older patients seek medical attention. Our results (Table 2) on pain perception certainly support a theory that pain appeared later in the older age group as only those with compression grades 3– 6 complained of pain but in the youngest group there was an equal split between mild and severe compression among those who complained of pain. As the nerve compression is usually a gradually developing pathology it is reasonable to conclude that a principal reason for more severe nerve compressions being found in older patients with carpal tunnel syndrome is that they have had the condition for longer because they have been unaware of the condition as they did not experience the same subjective complaints as younger patients would do. We believe that lack of comparison of the subjective perception of duration or outcome after carpal tunnel syndrome surgery with the age of the patients can explain why some reports have failed to find correlation between severity of compression and symptoms. 13 This is underlined by our results in Table 3 where the comparison of NCS with subjective symptoms of numbness and paraesthesia show that only two of the 34 patients older than 70 had low severity grades of compression but that as many as 14 of the 30 patients younger than 40 had low severity compression despite eight of the younger patients reporting their low severity entrapment as giving them intense sensory symptoms. In contrast, half of the older patients self-reported only milder symptoms despite severe compression. This finding may explain the observation by Hobby et al. 5 that though the majority of patients over 70 who had carpal tunnel release experienced an improvement, they were less satisfied than younger patients, and the older patients often had problems with persistent numbness. Therefore, the older patients’ self-assessment cannot be relied on as much as that of younger patients in establishing how long they have had carpal tunnel syndrome or how severe the entrapment is likely to be. This could explain why some researchers have not found any correlation between self-assessment of duration, severity and outcome when NCS were not performed14 or in a recent study when NCS were performed, why high incidence of absent nerve conduction were found in older patients with bilateral carpal tunnel syndrome. 15 One of the main weaknesses of our study is the relatively small number of participants; therefore, further prospective studies on larger numbers of patients may would confirm and expand our findings. Nevertheless, to the best of our knowledge our paper is the first to test a plausible clinical hypothesis by analysing and comparing subjective (symptom severity) and objective (NCS) evidence on patients with carpal tunnel syndrome resistant to conservative treatment in relation to different age groups.
In conclusion, patients older than 70 years of age with carpal tunnel syndrome resistant to wrist splints have significantly more severe nerve compression and less subjective complaints than similar patients who are younger than 40 years of age. We are of the opinion that the lower satisfaction level among some older patients after surgical release is likely to reflect a longer period of subcli-nical median nerve entrapment than in younger patients, and therefore more severe compression as a consequence of time. We, therefore, recommend that clinicians have a lower threshold for investigating with NCS older patients with suspected carpal tunnel syndrome in order to prevent advanced compression that may not be surgically reversible by the time they present for surgery.
Footnotes
Acknowledgements
None