
Abstract
This manuscript highlights polyorchidism as a differential diagnosis in scrotal masses and explains how to approach this rare condition.
DECLARATIONS
None declared
None
Written informed consent to publication has been obtained from the patient or next of kin
FC
PK presented the case history, researched the topic and drafted the manuscript; FC was the supervising consultant who reviewed and edited the manuscript; both authors read and approved the final manuscript
Bruce Montgomery
Introduction
Polyorchidism is an unusual abnormality of the genital tract in which supernumerary testes are present. To date there have been 178 reports (198 cases) of polyorchidism in the English literature. 1 To our knowledge, only two cases of bilobed testis have been previously described in the paediatric literature.2,3 It may be presumed that a bilobed testis is an incomplete expression of triorchidism. 2 Since there are insufficient data in the urological literature regarding the ideal management of bilobed testicles, we believe it is important to report this case to provide more information about this condition.
Case report
A 30-year-old African-Caribbean man presented to the outpatient clinic with 10-year history of a palpable lump in the left hemi-scrotum associated with some discomfort. There were no other urological symptoms or any significant past medical history. Abdominal examination was normal with no palpable mass or groin herniae. Scrotal examination revealed a normal right testis and scrotal content, but on the left side there were two similar size lumps. It was difficult to make a distinction between the normal testis and the mass because of their similar consistency and size. They were attached to each other superio-inferiorly. There was one epididymis and vas. An urgent scrotal ultrasound identified a left-side duplicated testis with normal echotexture and blood flow (Figure 1). Testicular tumour markers (HCG and α-fetoprotein) were found to be in normal range. For confirming the diagnosis and further anatomical evaluations a scrotal magnetic resonance imaging (MRI) scan was performed which showed a left-side bilobed testis with a single epididymis and vas attached to the upper lobe (Figure 2).

Transverse sonogram demonstrates a bilobed configuration of the left testicle. The left hemi-scrotal structures have the same normal echogenicity
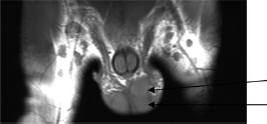
Coronal view of the scrotal MRI scan clearly demonstrates a bilobed testicle on the left draining into a single epididymis and vas
A diagnosis of a bilobed left testis was made and the patient was reassured. A follow-up review was organized.
Discussion
Blasius recorded the first case of triorchidism at a routine autopsy in 1670. 1 Some believe that the condition should be confirmed by histological examination. The first histologically documented case of polyorchidism was reported by Lane in 1895. 4
Polyorchidism has been identified in boys and men aged 3-75 years but most patients are in their early adulthood.1,5 The majority of supernumerary testes are located in the scrotal region (66%) followed by inguinal (23%) and abdominal (9%) positions. 1 The most common presentation of polyorchidism is triorchidism with the supernumerary testis confined to the left side.1,5
The exact etiology of polyorchidism is unknown, however, a few theories have been suggested including anomalous appropriation of cells in the genital ridge before 8 weeks of gestation, duplication or transverse vs. longitudinal divisional of the urogenital ridge, incomplete degeneration of mesonephrones and development of peritoneal bands. No single theory can explain all types of polyorchidism. 1 It could be postulated that in bilobed testicles, the division of the genital ridge is incomplete, resulting in a bilobed appearance. 2
There are a number of classifications for polyorchidism. Leung 6 described the first anatomical classification which was based on the possible embryological variations:
Type I: Supernumerary testis lacks an epididymis or vas and has got no attachment to the usual testis (division of genital ridge only);
Type II: The supernumerary testis drains into epididymis of usual testis and they share a common vas (division of genital ridge occurs in the region where the primordial gonads are attached to the metanephric ducts, although the mesonephrons and metanephric ducts are not divided);
Type III: The supernumerary testis has its own epididymis and both epididymis of ipsilateral testes drain into a common vas (complete transverse division of genital ridge as well as mesonephrons);
Type IV: Complete duplication of testis, epididymis and vas (vertical division of genital ridge and mesonephrons).
According to Leung, Type II is the most common type and together with Type III they comprise 90% of cases of polyorchidism. 6
Similarly, Singer et al. suggested an anatomical as well as functional classification 7 :
Type I: Supernumerary testes attached to the draining epididymis and vas deferens with reproductive potential (Leung Types II, III and IV);
Type II: Supernumerary testis lacks any attachment or any reproductive potential.
Most cases of polyorchidism are found incidentally during evaluation for other symptoms such as inguinal hernia and undescended testis. 1 Testicular torsion is also another common symptom and the most common complication of polyorchidism. 5
The incidence of testicular malignancy in polyorchidism in most reviews is between 5.7-7%. This incidence rate is much higher than normal population (0.004%) and even higher than the incidence of cancer in undescended testis (0.045%). However, in all reported cancer cases, malignancy was found only in a non-scrotal (abdominal or inguinal) supernumerary testis. 1
In a supernumerary testis spermatogenesis could be normal, reduced or absent. It seems the status of spermatogenesis is independent of the location of the supernumerary testis and also the presence of epididymis. 1
Management of polyorchidism has been subjected to much debate. With recent improvements in imaging techniques such as ultrasound and MRI scansmost cases of polyorchidism can be diagnosed and followed up accurately without any need for surgical exploration or histological examination. 2 With regard to non-scrotal supernumerary testes, orchidectomy is advisable considering the high incidence of malignancy. If the patient is symptomatic or there is a suspicion for malignancy scrotal exploration, biopsy and orchidectomy are recommended if the result of intraoperative frozen section is positive for malignancy. On the other hand, if the decision is to preserve the supernumerary testis it would be appropriate to perform orchidopexy in order to prevent testicular torsion in the future. 1
Conclusion
Bilobed testis, despite its rarity, should be within the differential diagnosis when a testicular mass is suspected. As bilobed testicles may be a variant of polyorchidism, related potential complications associated with this condition must be considered.
Footnotes
Acknowledgements
None