
Abstract
Objectives
In the winter of 2005-2006 the management at our children's hospital elected to admit ‘overspill’ acute medical admissions to the ward used for plastic surgery and burns for logistical reasons. This study was conducted to assess the effects of that change on the incidence of infective complications in thermally injured patients.
Design
We conducted a retrospective study by reviewing the case-notes. The data gathered included days on IV fluids and antibiotics, transfer to the Paediatric Intensive Care Unit (PICU), microbiology and a ‘septic signs score’ – based on pyrexia, irritability, diarrhoea/vomiting, wound colonization, bacteraemia. We compared the study winter (when mixed with the medical admissions) to the two preceding winters (control).
Setting
Royal Hospital of Sick Children in Edinburgh.
Participants
Seventy-three patients were studied, 23 in the sample winter and 50 in the two preceding control winters.
Main outcome measures
The outcomes studied were the maximum ‘septic signs score’; patients with a score ≥3; wound colonization; PICU admission; days on antibiotics and IV fluids.
Results
A statistically significant increase in patients with septic episodes was demonstrated by an increase in the mean septic signs score (0.66 to 1.48, p = 0.044) and the number of patients with a score ≥3 (4% to 22%, p = 0.017). Other analysed variables did not reach statistical significance although the raw data suggested a trend.
Conclusion
It was concluded that there is an association between mixing acute medical admissions with thermally injured patients and an increase in the incidence of infective complications in the latter group.
DECLARATIONS
None
Not applicable
FS
All authors contributed equally
Introduction
The need for a clean and safe environment in burns units is essential and each unit has measures to promote infection control and assessment of infective complications. At the Royal Hospital for Sick Children in Edinburgh (RHSC) thermally-injured patients are monitored closely and any signs of septic illness documented daily. These include: pyrexia (>38°C); irritability; diffuse macular rash; occlusive dressings; diarrhoea or vomiting; white cell count <4.0; urine output <1 mL/kg/hr; high fluid requirement (above burn resuscitation fluid); inflamed mucous membranes; wound colonization; and hypotension – a late and very serious sign. Our guidelines state that if a child has three or more of the above; there is a strong ground for suspicion of sepsis. These guidelines are based on the Centers for Disease Control 1980 criteria to define toxic shock syndrome (TSS). 1 The possibility of Staphylococcus aureus or Streptococcus pyogenes associated TSS is of particular concern in the paediatric population.2,3
During the winter of 2005-2006, the management team at the RHSC elected to mix acute medical admissions with paediatric burns and plastic surgery patients for logistical reasons. The subjective impression of medical and nursing staff was of a significant increase in infective complications and septic episodes. This project is a case-control study comparing the incidence of infective complications in the winter of 2005-2006 (November-January) with the two previous winters.
The hypothesis tested was that mixing medical patients with the thermally-injured patients increased the incidence of infective complications: burn-related sepsis and wound colonization. It would seem self-evident that the introduction of a wide range of micro-organisms carried by medical patients around the susceptible thermally-injured patients would increase the risk of infection.
Methods
The case-notes of all the paediatric patients admitted to the Burns and Plastic Surgery unit at RHSC in Edinburgh between 1 November 2005 and 31 January 2006 (which is the period in which the medical admissions were mixed with the thermally-injured patients) were reviewed. The control groups were all the burn patients admitted to the unit in the two preceding winters (1 November 2003-31 January 2004 and 1 November 2004-31 January 2005) when there were no medical admissions on the ward.
Infective complications were studied, as defined by parameters indicative of septic illness mentioned above. They were summated as the main outcome measure and the data collected are shown in the table in Appendix 1. Data was collected for five days post-admission, and for every sign present the patients received 1 point. The points were added up and the maximum score for any one day recorded: the ‘septic signs score’. Other complications of wound infection such as delayed healing or graft failure were not studied.
Wound colonization was defined as the isolation of Staphylococcus aureus, Staphylococcus pyogenes and Pseudomonas aeruginosa from a wound swab in the absence of clinical evidence of local infection.
Medical admissions to the burns ward in the studied winter were also considered and the diagnoses recorded.
Statistical analysis was carried out, the groups were compared and confounding factors assessed. Tests used include means, medians, histograms, box plots, T-Tests and Chi-squared tests.
Results
A total of 73 patients were studied, 23 patients in the sample winter of 2005-2006, and 50 patients in the control winters of 2003-2004 and 2004-2005. Nine patients (three from the winter studied and six from the control winters) whose medical records could not be traced were excluded.
Overspill medical admissions were only a winter phenomenon in 2005-2006; hence control data were restricted to winter months of the two previous years. The data were also restricted to paediatric patients. The patients ranged from a few months old to 13 years of age.
A few confounding factors may have affected the results: patients’ age (young children are more susceptible to TSS because antibody protection against TSST-1 increases with age 4 ); bacteria detected on the wound; and the cause of the thermal injury. Those were analysed and the two groups’ statistical similarity, in terms of age (Table 1), percentage of body surface affected (Table 1), length of stay (Table 2) and aetiology, precluded the need for the use of regression in the statistical analysis. Other potential confounding factors such as previous infections, past medical history and the changeover of the junior staff in the three-year period were not studied or analysed. Nevertheless, it is noted that the senior staff responsible for care were consistent throughout the study period. The admission criteria for a burns patient (all burns greater than 5%; burns in difficult areas, e.g. perineum, potential airway injury or compromise, potentially septic child, and suspicion of non-accidental injury) was not altered over the three years.
Patient demographics

Length of stay

Septic signs score
There was a statistically significant increase (P = 0.044) in the mean septic signs score. The mean and median scores (Table 3) of the sample winter were significantly greater than the control winters. The mean score in particular was noted to be more than double in the sample winter.
Septic Signs Score

P = 0.044
Septic signs score of 3 or over
For further analysis the septic signs score data were recorded as 0-2 and 3-6; the latter of which results in a high degree of suspicion of burn-related sepsis and/or TSS. The results (Table 4) show a 5-fold increase in the percentage of patients with a septic signs score of 3 or over; from 4.0% in the control winters to 21.7% in the sample winter. The Chi-squared test demonstrated statistical significance.
Septic Signs Score ≥3
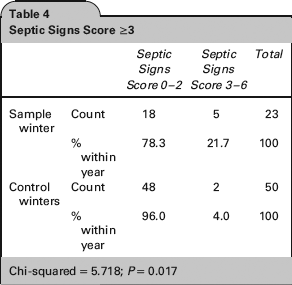
Chi-squared = 5.718; P = 0.017
Of the patients with a score of 3 or over: 100% had a pyrexia; 100% had growth on the wound swab; 57% were irritable and 71% had diarrhoea and vomiting – which one would expect in children with nosocomial viral infections.
Wound colonization
Although wound swabs are not a reliable predictor of infection, wound colonization was analysed and it increased from 38% of patients in the control winters to 47.8% in the sample winter (Table 5). The increase was statistically insignificant.
Wound colonization

Chi-squared = 0.628; P = 0.0428
Paediatric Intensive Care Unit (PICU) admission
There were more PICU transfers (Table 6) in the control winters; however, the difference was statistically insignificant. Patients were transferred to the PICU for various reasons. One patient from the study winter was admitted because of extensive (47%) burns. The other three admissions to PICU were in the control winters; one was admitted for airway management and two were admitted due to infective complications.
PICU admissions

Chi-squared = 0.083; P = 0.773
Days on antibiotics and days of IV fluids
The mean number of days on antibiotics appeared to increase from 1.86 in the control winters to 3.30 in the sample winter – a 77% increase (Table 7). The mean number of days on IV fluids also appeared to increase from 0.84 in the control winters to 2.83 in the sample winter – a 236% increase (Table 7). However, neither of these increases was statistically significant.
Days on antibiotics and IV fluids

P = 0.181 for antibiotics; P = 0.098 for IV fluids
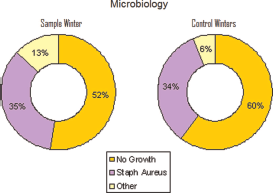
Microbiology
There was no change in the culprit organisms over the time period. The isolated organisms and trends were practically identical. S. aureus was the most common isolate with a 34% overall incidence (Figure 1). Group A S. pyogenes was isolated in three patients: one in the study winter and two in the control winters.
Microbiology
Furthermore, the trends of isolation of Group A streptococcus pyogenes in patients in the RHSC were reviewed. There was no significant increase in infection rate in the study period. Although we did not correlate the infective organisms between the medical admissions and the burns patients, the lack of significant increase in streptococcus pyogenes (as a surrogate indicator of the trend of gram-positive organisms across the hospital); strengthens the evidence that the increase in infection rate in our study group was due to the mixing of patients. Unfortunately we did not have the data regarding blood cultures drawn in either group.
Toxic shock syndrome
Only one patient in this study met the diagnostic criteria for toxic shock syndrome. This patient was in the control winter (2004-2005). In the other patients with a septic signs score of 3 or greater, no organism was identified on blood or wound culture.
Length of stay per percentage burn
One would expect the average length of stay (LOS) and the length of stay per percentage burn to increase reflecting an increase in infective complications. However, there was no statistically significant difference in the average length of stay between control winters (6.22 days) and in the study winter (5.82) (Table 2). Percentage burn was divided into quintiles and analysed against LOS (Table 2) and no statistical difference was found for burns up to 7%. In burns above 7%, the LOS was higher in the study winter; again this was statistically insignificant.
Severity of burns, management and outcome
Analysis demonstrated the severity of the burns, in terms of depth, in the two groups to be similarly distributed. The microbiology of the two groups was similar (Figure 1) and no resistant or atypical outbreaks occurred. The average percentage burn was also comparable (Table 1). There were no smoke-inhalation injuries in either group. One-third of patients, in both groups (31.6% in the study winter, and 33.3% in the control winters) were admitted to theatre for excision, debridement or split-skin grafting (Table 8). There were no significant differences in terms of scarring, with about 40% of the patients with no scarring (37% in the study winter and 43% in the control winters); however, there was double the percentage of severe/hypertrophic scarring in the control winters (33%) than in the study winter (16%). The rate of contractures was also double in the control winters (10% vs. 5%) and 10% of the control patients were readmitted after discharge (Table 8). These results were statistically insignificant.
Burn outcome

Not all data on outcome/management could be retrieved
Medical admissions diagnoses
A total of 179 patients were admitted to the ward for medical reasons in the winter of 2005-2006. Almost half (47%) of the medical admissions came in with infective pathology and diseases. A significant number of the ‘undefined pathologies’ (e.g. vomiting) may also have had an infective aetiology. Therefore, 47% probably underestimates the prevalence of infective pathology in the medical patients. Common diagnoses upon admission included upper respiratory tract infections (bacterial and viral), pneumonia, vomiting, gastroenteritis, diarrhoea, skin infections and pyrexia.
Discussion
Principal findings
Medical admissions
The study demonstrated that the rate of infective complications and burn-related sepsis did increase after mixing acute medical admissions with thermally-injured patients. There was a statistically significant rise in the proportion of patients with a septic signs score of 3 or greater. At least 47% of the medical admissions had infective pathology. It seemed self-evident to burn clinicians that case-mixing of this nature was illadvised. However, objections were overridden for logistical and economic reasons.
We recognize that the score was designed to pick up early warning signs of toxic shock syndrome. However, we are proposing that the mixing of medical patients with burns patients increases the risk of cross-infection with infections common to acute medical admissions and, therefore, confuses the picture and makes the assessment of the individual child more difficult.
We have not demonstrated which organisms were responsible for such an increase. The increase in septic score without an increased incidence of wound colonization could have been attributed to an increased virulence of endemic organisms in the sample winter. However, no major differences in the characteristics of endemic organisms in our institutions have been identified in the study period. This is, therefore, considered unlikely. We consider it more likely that a variety of infective agents including viruses were likely to be involved, reflecting the prevalence of infective agents leading to acute paediatric medical admissions.
It is clear that patients with respiratory, gastrointestinal or dermatological infections in close proximity to burns patients cannot be regarded as ideal clinical practice.
Risks of infection in thermally injured patients
Infection remains the largest single cause of morbidity and mortality in acutely-burned children. 5 Children with serious burns are prone to a host of septic complications. This tendency to infection is due to the immunosuppressive effect of burn injury, the loss of the skin and mucosal physical barriers, and the requirement for invasive support devices. 6 Another risk factor for toxin-mediated infection in paediatric burns is the localization of such burns to the face and head. 7
Toxic shock syndrome
One of the main concerns in paediatric burns patients is staphylococcal, or streptococcal, toxic shock syndrome (TSS).2,3 TSS is an underdiagnosed complication of burns and scalds in paediatric patients. It can follow minor burns and lead to serious complications.8,9
The true incidence of TSS may be higher than originally reported, especially since there is no definitive diagnostic tool. 10 The incidence of TSS does seem to be higher in the UK than other European countries although this may reflect diagnostic fashion. 11
The incidence may be reduced by the use of systemic or topical antimicrobials and the avoidance of occlusive dressings,12– 14 although a UK survey suggested no association between the management of the wound and subsequent development of TSS. 15
Our practice and dressing protocol was consistent throughout the study period. Superficial scalds above 5% are covered with Biobrane™, smaller superficial scalds are treated with Mepitil™ or Jelonet™. Facial scalds are managed exposed. Where scalds are obviously deeper, either silver sulphadiazine ointment or silver impregnated dressings (Acticoat™) are used as a prelude to early surgery. We have not used systemic antibiotic prophylaxis as a routine in paediatric thermal injuries principally due to concerns about the likelihood of increased prevalence of resistant bacteria. Patients undergoing burn excision and grafting were routinely given a single intravenous shot of antibiotic tailored to their culture results, or Co-Amoxiclav if swabs were non-contributory. Prolonged antibiotics (IV flucloxacillin and IV benzylpenicillin) were only started in response to clinical suspicion of sepsis or TSS.
Sub-Biobrane infection is dealt with according to recognized protocols; if localized then the dressing on that area of the infected blistering is removed and Anticoat or Flamazine applied; if generalized then the whole dressing is removed and replaced.
Role of isolation and infection control
The practice of both isolation and barrier precautions of acute-burn victims is widespread and evidence-based.16 - 20
Our burns unit compromises 16 beds in total, of which four are single cubicles. The cubicles have a single-door system and do not have laminar flow or positive pressure systems. The policy in our unit has been to manage thermally-injured children in single rooms with simple protective barrier precautions until healing is advanced or wounds grafted. All patients are initially admitted to a cubicle. Dressing changes are a clean aseptic procedure and the nursing and medical staff adhered to a strictly enforced and audited hand-washing protocol. No clothing below the elbows is worn. Contaminated hands are washed with antiseptic solution and warm running water. Before all patient contact, non-contaminated hands maybe doused with alcohol gel as an alternative.
In the study winter, the medical patients were in the same ward area of the burn patients. The hospital was built in the 19th century and so the cubicles are adjacent to the ward area with only the single door as barrier. The nurses were communal to both patient cohorts and each nurse would typically care for three to four patients with a mixture of medical admissions in the open ward and isolated patients in the cubicles.
In previous winters, the percentage bed utilization by burns patients was similar but the empty beds on the unit were most frequently occupied by trauma patients.
Limitations and weakness of the study
There are a number of limitations to the study, one of which includes the number of patients studied. Although the main outcomes reached statistical significance, the other parameters may have also shown a significant change with a bigger cohort. In addition, the medical admissions were not studied in detail. We know that at least 47% of them had an infective pathology, but the culprit organisms were not recorded or compared to those in the burns patients. However, it is very difficult to prove cross-contamination and we do not think that having such data would alter the conclusions. We accept that after mixing the burns patients may have picked up nosocomial viral infections although we were unable to demonstrate that with nasopharyngeal results, e.g. a limitation of a retrospective study.
Other complications of wound infection, such as delayed healing and graft failure were not studied. Also the impact of the increase in the number of the patients on the ward, and whether that had a role to play in the increase in infection was not analysed. Furthermore, other potential confounding factors, as mentioned above, were not studied or analysed.
Meaning of the study
Based on the evidence presented we believe that co-location of potentially infected paediatric medical admissions with thermally-injured children compromises the ability of clinical teams to provide an effective isolation policy. We believe that the maintenance of a clean environment is fundamental to the care of burn patients. A low prevalence of patients with infective illnesses must be a pivotal part of that policy.
We are pleased to report that the admissions policy of our institution has now been amended appropriately. We are also pleased to report that there are plans for a new hospital, with single isolation cubicles within a high dependency unit for all burn patients.
Unanswered questions and future research
Although the study shows an increase in trends suggesting infection; we were unable to prove cross-contamination as a causative link. Further analysis of nasopharyngeal results, blood culture data and culprit organisms in the medical admissions may lead to a stronger study.
Footnotes
Acknowledgements
We would like to acknowledge the great effort and assistance we have received from the following people and would like to extend our sincerest gratitude for the time spent in helping us do this project: Julie Freeman (Paediatric ITU Constultant at RHSC), Annette Henderson (Audit studies), Kim Scott (Medical Record Assistant Manager), Tony Wright (Medical Record IT Technician), Margaret MacDougall (Medical Statistician), Sheila Fisken (Librarian)