
Abstract
The intratracheal (IT) injection technique has been widely used in the mouse studies of pulmonary diseases. Here, we describe a non-invasive technique using oral instillation challenge with the surfactant phospholipid that may advantageously replace the traditional IT technique. We performed comparative studies between oral instillation and IT injection of both vectors (adeno-associated virus, AAV vector) and bacteria (Pseudomonas aeruginosa). Our results demonstrated that the oral instillation is a reliable alternative to IT injection. The administration of a fluorophore-labelled AAV vector demonstrated a similar pattern of distribution and quantity of vector delivered by oral instillation compared with IT injection. In addition, administration of AAV5-alpha-1 antitrypsin (AAT) to the lungs by oral instillation resulted in similar levels of AAT in both the lung homogenates and sera compared with the IT injection group. In our study of P. aeruginosa delivery, oral instillation resulted in similar mouse weight loss, cytokine levels in the epithelial lining fluid [interleukin (IL)-1β, IL-6, tumour necrosis factor-α, neutrophil chemokine and macrophage inflammatory protein-1α], lung histology/pathology and bacterial loads. Therefore, we conclude that oral instillation of materials mixed with surfactant phospholipid is an adequate and reproducible technique to replace the invasive IT injection procedure for the delivery of either vector or bacteria to the lungs. This procedure has the benefits of eliminating the discomfort, local inflammation and mortality associated with the more invasive IT surgical procedures.
A host of lung diseases, such as cystic fibrosis, pulmonary fibrosis, allergic asthma, acute respiratory distress and other inflammatory or infectious lung diseases, require animal studies in which mice are infected or given a therapeutic agent via airway administration. A widely used procedure is the intratracheal (IT) injection of an infectious, toxic or therapeutic agent for this purpose. In this procedure, the trachea of a mouse is exposed by surgical intrusion under anaesthesia. After either a therapeutic vector or bacterial dose is injected in the trachea, the trachea is sutured under anaesthesia. IT injection ensures an equal amount of vector or bacteria administered to each animal, but this invasive technique also causes side-effects, such as discomfort, local inflammation and occasionally mortality.
An oral instillation method has been described by Wills-Karp et al. (1999) with minor modifications by Walters et al. (2001) For this instillation procedure, the anaesthetized mouse is placed in the supine position on a 60° incline board. The tongue is gently extended using coated forceps and 30–50 μL of sample is dropped into the back of the oral cavity. Guilbault et al. (2005) used a similar technique to administer Pseudomonas aeruginosa-laden beads into the trachea with microscope guidance. Oral instillation technique eliminates discomfort, local inflammation and mortality due to surgery. However, little is known concerning its efficacy and reproducibility, and no published articles have used this method to deliver adeno-associated virus (AAV) vectors. Although rodents are likely to aspirate materials in the oral cavity when placed under anaesthesia, the possibility that some or all of the material would be swallowed into the stomach still exists. In this study, we modified a previously described oral instillation method (Walters et al. 2001) with the addition of surfactant phospholipid to assist distribution of vector or bacteria more evenly in the lungs. For the first time, we also compared the modified oral instillation technique directly with IT injection to determine if this simple and non-invasive method can replace the invasive IT procedure to deliver bacteria or therapeutic agents to the airways of mice more efficiently and consistently.
In the first part of the study, we administered AAV5-alpha-1 antitrypsin (AAT) vector using both the techniques. By employing a fluorophore dye-labelled AAV vector, we compared the AAV vector distribution in lungs by both the techniques. We also determined the AAV vector gene expression by measuring human AAT protein in lung homogenates, and the sera of mice after vector administration.
In the second part of the study, we evaluated mouse weight loss, cytokine profiles in the lung homogenates and epithelial lining fluid (ELF), lung pathological changes and bacterial burden following the delivery of P. aeruginosa-laden agarose beads. Again, we wanted to compare the efficacy of the two methods and determine if the surfactant phospholipid would inhibit the Pseudomonas growth, making this particular delivery method unsuitable for P. aeruginosa administration. Our goal was to find a non-invasive method with the same degree of reproducibility and efficiency as the IT injection, while eliminating the side-effects associated with surgeries.
Materials and methods
Pseudomonas aeruginosa and adeno-associated virus vector
A mucoid P. aeruginosa strain isolated from an unidentified cystic fibrosis patient's sputum was used for this study. Bacteria were maintained in glycerol stocks and stored at −80°C. A recombinant AAV serotype 5 vector encoding human alpha-1 antitrypsin (hAAT) driven by cytomegalovirus/chicken β-actin hybrid promoter (AAV5.Cβ.hAAT) was produced and purified by the University of Florida vector core using methods already published (Virella-Lowell et al. 2005).
Animals
Eight-week-old female C57BL/6 (C57BL/6NCrl) mice and CD-1 (Crl:CD-1) mice were purchased from the Charles River Laboratories (Wilmington, MA, USA). The mice were fed Harlan Teklad Sterilizable Rodent Diet 8656 (Harland Teklad, IN, USA) and bedded on autoclaved 1/8 in. corncob bedding and corn husk nesting material (Harland Teklad). The mice were housed in Micro-Isolator Top Flow Ventilated cages (Tecniplast, Exton, PA, USA) in ventilated racks and studied under Institutional Animal Care and Use Committee approved protocols in the animal facilities of the Medical University of South Carolina. The C57BL/6 mice were used for the AAV vector study and the CD-1 mice were used for the P. aeruginosa-laden agarose beads study.
Labelling of adeno-associated virus vector with fluorophore dye
Alexa 610 succinimidyl ester fluorophore was purchased from Invitrogen (Carlsbad, CA, USA). AAV5.Cβ.hAAT was incubated with a reactive dye solution (10 mg/mL Alexa 610 succinimidyl ester fluorophore dissolved in dimethyl sulfoxide) with continuous stirring at room temperature (RT) for one hour. Then, the AAV-fluorophore conjugated (AAV5.Cβ.hAAT*Alexa 610) was separated from the unreacted labelling reagent through a Sephadex G column and stored at 4°C.
Preparation of P. aeruginosa-laden agarose beads and sterile agarose beads
In order to establish a model of chronic infection, bacteria-impregnated agar beads as described by van Heeckeren and Schluchter (2002) were used to infect the lungs. Briefly, P. aeruginosa was streaked on a tryptic soy agar (TSA) plate from frozen stock in 10% glycerol. A fresh P. aeruginosa colony was inoculated in tryptic soy broth (TSB) and shaken overnight at 37°C. The next day, an aliquot (100 μL) of the inoculated broth was inoculated in a new 50 mL TSB and shaken overnight at 37°C. Then, the bacteria was concentrated by centrifugation and added to warm (50°C) autoclaved 2% low melting agarose. The bacteria–agarose mixture was added to warm (50°C) heavy mineral oil and stirred rapidly, first at room temperature for 6 min and then cooled by adding ice for over 10 min. For the preparation of sterile agarose beads, 2% low melting agarose was autoclaved and added to warm (50°C) heavy mineral oil as above. The resulting beads were washed sequentially with 0.5% sodium deoxycholate (SDC), 0.25% SDC and four washes with Dulbecco's phosphate-buffered saline (PBS) (Mediatech Inc, Herndon, VA, USA). Next, the beads were collected and homogenized using a Kinematica polytron PT10/35 homogenizer (Kinematica, Littau, Lucerne, Switzerland). The size of the beads was verified microscopically, and only those preparations containing beads predominantly of 100–200 μm in diameter were used for administration. To determine the bacterial concentration in the colony-forming units per millilitre (cfu/mL), the final inocula was diluted in 10-fold serial dilutions, spread on TSA plates and incubated at 37°C overnight.
Preparation of surfactant phospholipid liposomes
1,2-dipalmitoyl-sn-glycero-3-phosphocholine (DPPC) and 1-palmitoyl-2-oleoyl-sn-glycero-3-phosphocholine (POPC) phospholipids were purchased (Avanti Polar Lipids, Alabaster, AL, USA) with stock concentrations of 20 mg/mL (DPPC in chloroform) and 10 mg/mL (POPC in chloroform). For every millilitre of final liposome suspension, 17.5 mg of DPPC (0.875 mL stock) and 7.5 mg of POPC (0.75 mL POPC stock) were added in a clean, sterile 13 × 100 mm glass tube. The tube was capped and mixed well via vortex. The solvent was removed via nitrogen stream, with the tube submerged in a 40°C waterbath, and mixed during the drying process. After the samples were dry, the tubes were transferred to a lyophilization flask and vacuum-dried overnight without additional heating. PBS (1.0 mL) was added to each tube; then the tubes were heated at 45°C for 15 min, vortexed for 30 s and sonicated for 10 s. This process was repeated three times to ensure that the liposome preparation had consistent viscosity and did not contain large liposome aggregates. The liposomes were transferred to sterile screw-cap plastic cryovials using sterile pipette tips and stored at 4°C. The stock phospholipid liposome concentration was 7:3 (mol/mol) DPPC/POPC in 25 mg/mL total phospholipid. On the day of AAV or P. aeruginosa administration, the phospholipid liposomes were diluted to 4 mg/mL with AAV5.Cβ-hAAT or diluted P. aeruginosa-laden beads.
Oral instillation of AAV vector or P. aeruginosa-embedded or sterile agarose beads
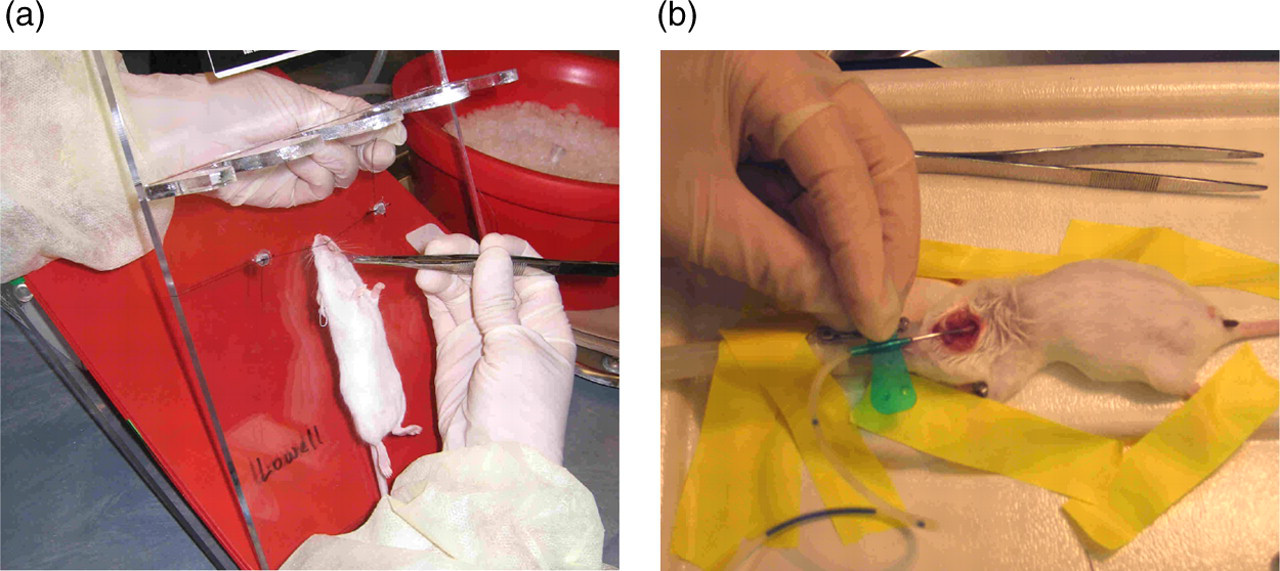
Mice were anaesthetized by inhalation of a mixture of oxygen and isoflurane in a closed ventilation chamber for 5 min. Mice were then placed in a supine position on a 60° incline board. The tongue was gently extended using coated forceps (Figure 1a) and 40 μL of sample was instilled at the back of the oral activity above the tracheal opening. The mice aspirated the lipid by gulping and typically recovered from anaesthesia within 2–5 min after oral instillation.
For the AAV dissemination study, a 4 mg/mL bolus of surfactant phospholipid liposomes with 1 × 1012 particles of AAV5.Cβ.hAAT*Alexa 610 was administered. For the AAV protein expression experiments, a 4 mg/mL bolus containing surfactant phospholipid liposomes with 2 × 1012 particles of AAV5.Cβ.hAAT was administered.
For the P. aeruginosa delivery experiments, a 4 mg/mL bolus of surfactant phospholipid liposomes with sterile agarose beads or 5 × 106 cfu of P. aeruginosa-laden beads was administered.
Intratracheal administration of adeno-associated virus vector or P. aeruginosa-embedded or sterile agarose beads
Mice were anaesthetized by inhalation of a mixture of oxygen and isoflurane in a closed ventilation chamber. Later, the mouse was placed on a surgical platform, and anaesthesized by inhalation of a mixture of oxygen and isoflurane via a face-mask and nebulizer tubing. Following a transverse cervical incision, the trachea was exposed and intubated with a sterile, flexible 21-gauge SURFLO winged infusion set (Terumo Corporation, Tokyo, Japan) attached to a 1.0 mL syringe (Figure 1b). Depending upon the agent, an inoculum of 40 μL AAV5.Cβ.hAAT*Alexa 610, unlabelled AAV5.Cβ.hAAT, P. aeruginosa-laden beads (5 × 106 cfu), or sterile agarose beads were injected into the lungs. All incisions were closed by suture. Mice usually recovered within 10 min after surgery.
Collection of samples
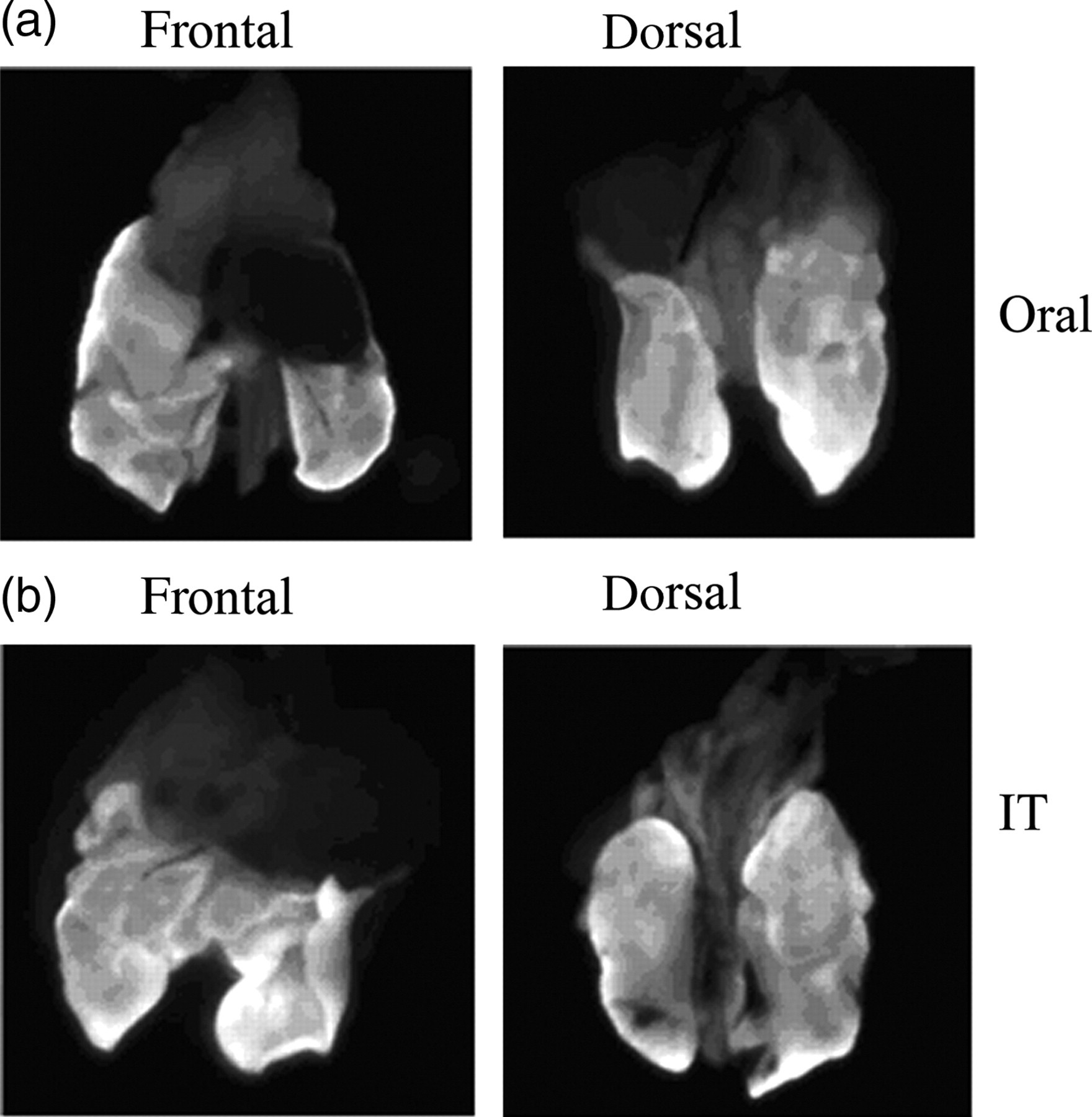
For the analysis of AAV5.Cβ.hAAT vector distribution, the mice were sacrificed 2 h after vector administration under isoflurane sedation. Lungs, heart and thymus from each mouse were removed and photographed under UV light.
For the analysis of AAV5.Cβ.hAAT vector protein expression, the mice were sacrificed six weeks after vector administration under isoflurane sedation. Blood was collected by puncturing the vena cava. Lungs were homogenized. Both lung homogenates and serum were analysed for AAT protein expression.
For the P. aeruginosa experiment, the mice were sacrificed three days postinfection under isofluorane sedation. Blood was collected from all the mice as above. The lungs from half the mice were collected and homogenized for quantitative bacteriology and cytokine analysis. Bronchoalveolar lavage fluid (BALF) was collected from the lungs of the other half of the mice, whose lungs were sent to histological analysis later. Briefly, the trachea was isolated by blunt dissection and an incision made in the upper portion of the trachea, which was cannulated with a 21-gauge shielded intravenous catheter (BD Bioscience, USA) attached to a 5 mL syringe. Then, the alveoli were gently washed three times with 1 mL PBS, recovering a BALF volume of approximately 1.5 mL. Lungs were then collected, weighed, fixed in 4% paraformaldehyde and sent for pathological analysis.
Preparation of lung homogenates and quantitative bacteriology
To prepare lungs for quantitative bacteriology, lungs were first washed in a 0.5 mL cell wash buffer (Bio-Rad, USA) and homogenized in 2 mL of PBS for 60 s at high speed using a Polytron PT10/35 homogenizer (Kinematica). Lung homogenates were diluted in 10-fold serial dilutions, spread on TSA plates and incubated at 37°C overnight. The lung homogenates were centrifuged at 1500 ×
Measurement of human alpha-1 antitrypsin
Human AAT expression in sera and lung homogenates was measured by enzyme-linked immunosorbent assay (ELISA). Briefly, the plate was coated with goat anti-hAAT (Sigma, USA) in Voller's buffer (2.76 g Na2CO3, 1.916 g NaHCO3, 0.2 g NaN3 in 1 L, pH 9.6). After washing the plate in PBS-Tween (PBS-T) three times, the serial dilution of standard AAT and samples (mice sera or lung homogenate) were added to the wells and incubated at 37°C for 60 min. Plates were then washed and blocked by bovine serum albumin (3% BSA in PBS-T) solution for 60 min at 37°C. Plates were then incubated with 1:1000 dilution of rabbit anti-hAAT (Sigma) for 60 min at 37°C. After washing the wells, they were incubated with 1:2500 dilution of goat anti-rabbit IgG-conjugated horseradish peroxidase (Sigma) for 60 min at 37°C. Following a brief wash step, 100 μL of TMB substrate (Research Diagnostics Inc, Flanders, NJ, USA) was added to each well. After 5 min of incubation, 100 μL of 0.5 N HCl was added to stop the reaction. Absorbance at 450 nm was measured using a VERSAmax tunable microplate reader (Molecular Devices, USA).
Assessment of weight loss
Body weight of all mice was determined before inoculation of P. aeruginosa-laden beads and before sacrifice.
Measurement of cytokines
Sera, BALF and lung homogenate levels of murine interleukin (IL)-1β, IL-6, tumour necrosis factor (TNF)-α, neutrophil chemokine (KC) and macrophage inflammatory protein (MIP)-1α were evaluated using the Bio-Plex protein array system (Bio-Rad, Hercules, CA, USA). Urea nitrogen (BUN) levels in sera and BALF were measured by the Stanbio Enzymatic Urea Nitrogen kit (Stanbio Laboratory, Boerne, TX, USA). ELF cytokine levels were calculated by correcting the BALF levels by a dilution factor based on the ratio of serum BUN/BALF BUN. All samples were run in duplicate.
Lung histopathology
After sacrifice, the mouse lungs were inflated, fixed in 4% paraformaldehyde for 48 h, and then embedded in paraffin. Five micrometre lung paraffin sections were stained with haematoxylin and eosin (H&E) using standard techniques and were examined for histopathological changes. The criteria of lung histopathology score were based on a previously published critera (van Heeckeren & Schluchter 2002) and are defined as follows: 0 = within normal limits, 1 = more red blood cells than normal, 2 = few lymphocyte infiltrated nodules present (0–4), 3 = several lymphocyte infiltrated nodules (5–10) and <1/4 lung consolidated, 4 = 1/4–1/2 lung consolidated, 5 = 1/2–3/4 lung consolidated and 6 = >3/4 lung consolidated.
Statistical analysis
Data are reported as the mean ± SD. Data comparing the oral aspiration delivery groups and IT delivery groups were analysed by paired or unpaired, two-tailed Student's t-test. All statistical tests were performed using GraphPad InStat (GraphPad Software, San Diego, CA, USA).
Results
Comparison of oral instillation and intratracheal injection of adeno-associated virus vector
To compare the efficiency of the delivery methods for AAV, mice were received fluorophore-labelled AAV (AAV5.Cβ-AAT*Alexa 610) by oral instillation or IT injection. The lungs' images showed that there was an even distribution of AAV5.Cβ-AAT*Alexa 610 in the lungs of the oral and IT groups (Figure 2). AAV5.Cβ-AAT*Alexa 610 was not detected in the hearts or thymuses of either groups, although an equal and small amount of the AAV5.Cβ-AAT*Alexa 610 was noted in the stomach of both groups (data not shown).
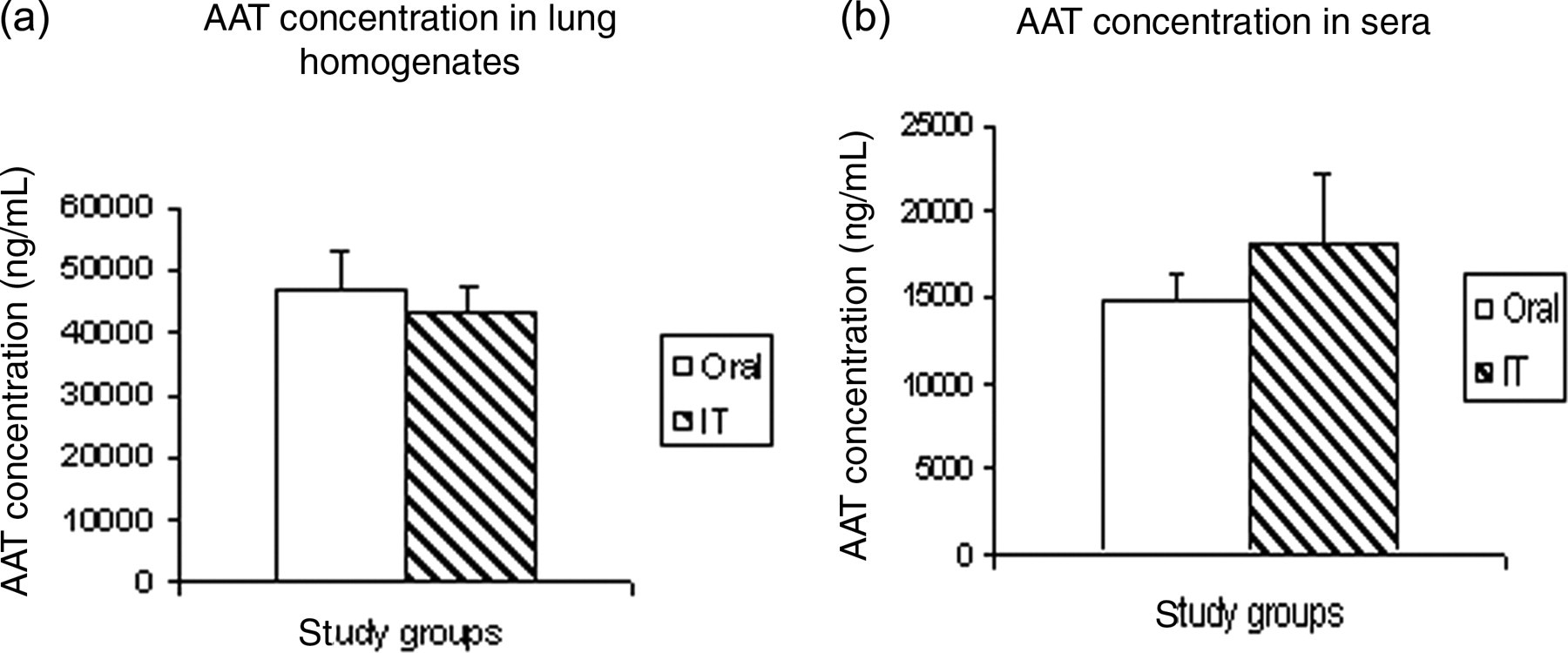
A separate group of mice received AAV5.Cβ.AAT by oral instillation (n = 7) or IT injection (n = 6). Six weeks after the AAV vector administration, hAAT expression in sera and lung homogenates was measured. Figure 3 demonstrated that there was no significant difference of AAT expression either in lung homogenates (Figure 3a, P = 0.2231) or sera (Figure 3b, P = 0.09) between both groups, thus demonstrating the modified oral instillation procedure is a reliable method for vector delivery.
Comparison of oral instillation and intratracheal injection of P. aeruginosa-laden beads
To compare the efficiency and reliability of oral aspiration versus IT delivery of P. aeruginosa, we administered 5 × 106 cfu of P. aeruginosa-laden beads to mice. Control mice were administered sterile agarose beads by both methods. Three days after the P. aeruginosa administration, mouse weight loss, cytokines (IL-1β, IL-6, TNF-α, KC and MIP-1α) expression in the ELF and lung homogenates, lung histopathology changes and bacterial burden were evaluated. In the IT group (20 mice), two mice were excluded from this study due to mortality after surgery; additionally two mice were excluded from this study due to P. aeruginosa beads leaking during IT injection.
Weight loss and weight loss percentage
The average original weight of the mice (n = 20) in the oral group was 29.31 g and the mice lost an average of 5.08 g (17.4%) of their original body weight following the delivery of 5 × 106 cfu P. aeruginosa-laden beads. The average original weight of the mice in the IT group (n = 16) was 27.51 g and the mice lost an average of 5.16 g (18.4%) of their body weight after administration of the P. aeruginosa-laden beads. There was no significant difference between the oral and IT groups in baseline weight or weight loss following infection (P = 0.3433).
Epithelial lining fluid cytokine profile
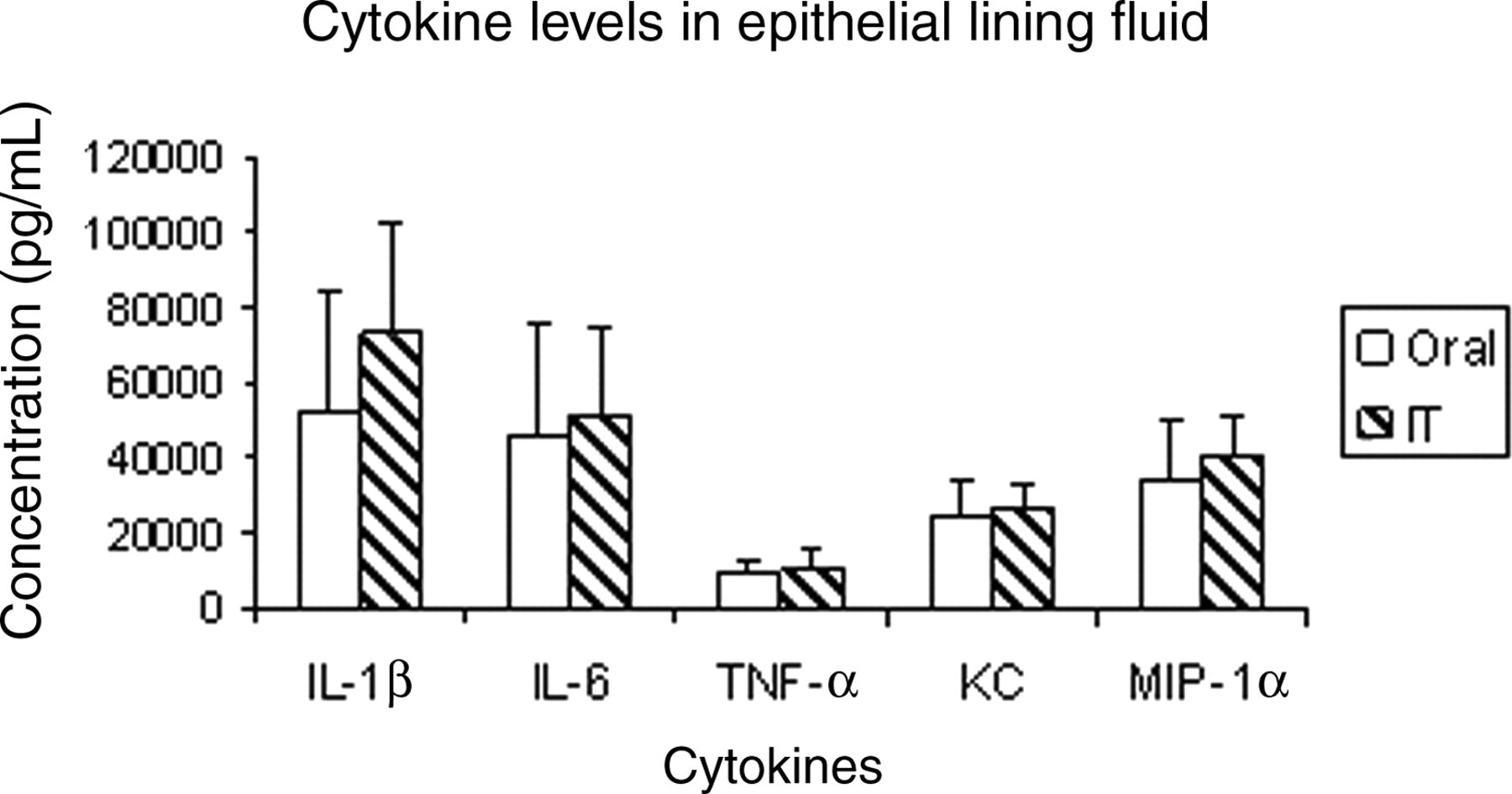
BALF was collected from the mice with P. aeruginosa-laden beads administered by oral instillation (n = 8) or IT injection (n = 8). Murine cytokine (IL-1β, IL-6, TNF-α, KC and MIP-1α) levels were assayed. BALF values were corrected for dilution using the BUN levels in the sera and the BALF to obtain more meaningful ELF values. No significant difference was detected between ELF cytokine levels (IL-1β, IL-6, TNF-α, KC and MIP-1α) in the oral and the IT delivery groups (Figure 4).
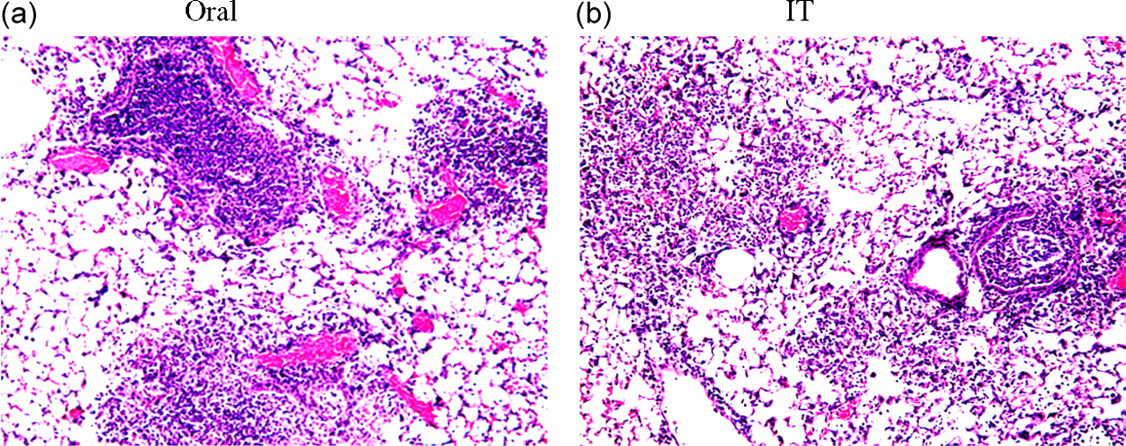
Lung histopathology
Both delivery methods had five to ten lymphocyte-infiltrated nodules and less than one-quarter of the entire lung sample consolidated (Figure 5). Further examination of the oral instillation delivery group of P. aeruginosa-laden beads (n = 8) revealed an average histopathology score of 3.90 and the average IT delivery group (n = 8) score was 3.88; this was determined to be not significant (data not shown).
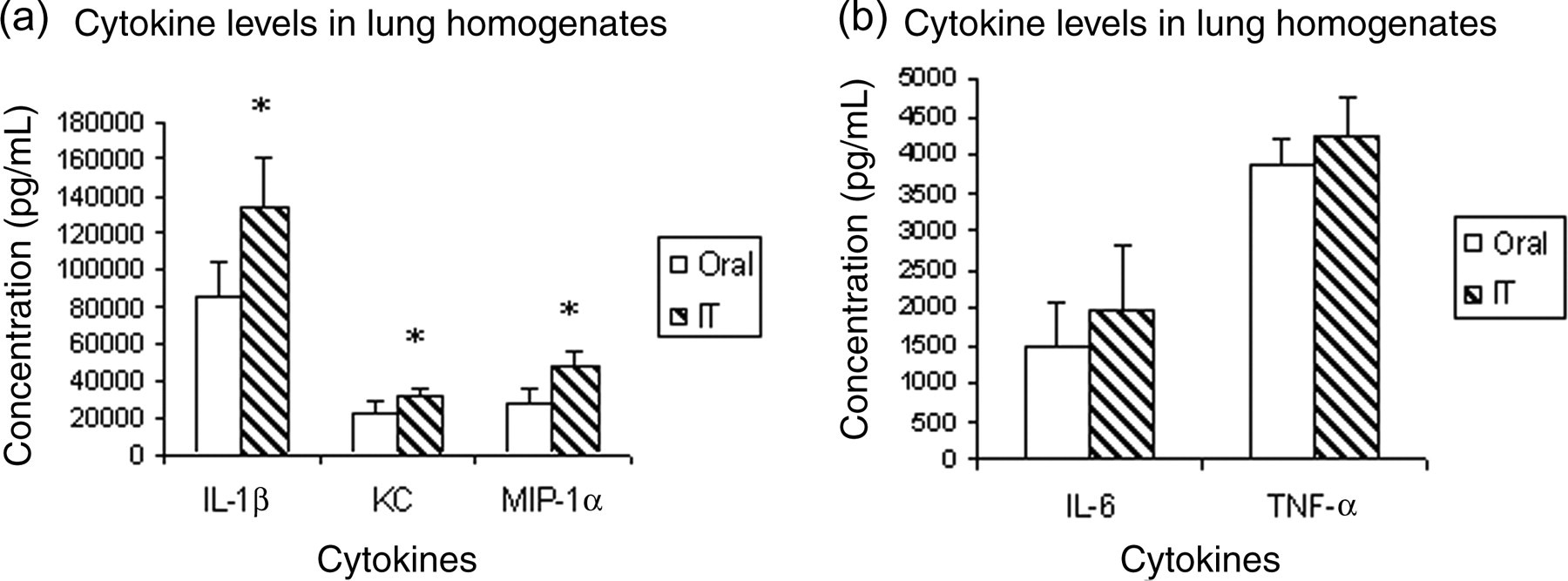
Lung homogenate cytokine profile
Levels of murine cytokine (IL-1β, IL-6, TNF-α, KC and MIP-1α) expression in the lung homogenates was determined following oral instillation or IT injection of P. aeruginosa. In the lung homogenates, the IT group (n = 8) had higher IL-1β, KC and MIP-1α expression than the oral group (n = 12) [P = 0.0029 (IL-1β), P = 0.0029 (KC) and P < 0.001 (MIP-1α)]. No significant difference existed in the IL-6 or TNF-α expression between the oral and IT delivery groups (Figure 6). It is important to note that the ratios of the standard deviations in the oral instillation delivery group compared with the IT delivery group were 0.716 (IL-1β), 1.76 (KC), 1.23 (MIP-1α), 0.69 (IL-6) and 0.72 (TNF-α), which proved that oral instillation had the same consistency as IT injection. In addition, both groups had significantly higher levels of the measured cytokines than our control sterile beads group (data not shown). Therefore, although IT delivery of P. aeruginosa-laden beads resulted in more lung inflammation, the oral instillation method is just as reproducible and can efficiently produce enough inflammation to distinguish it from non-infected models.
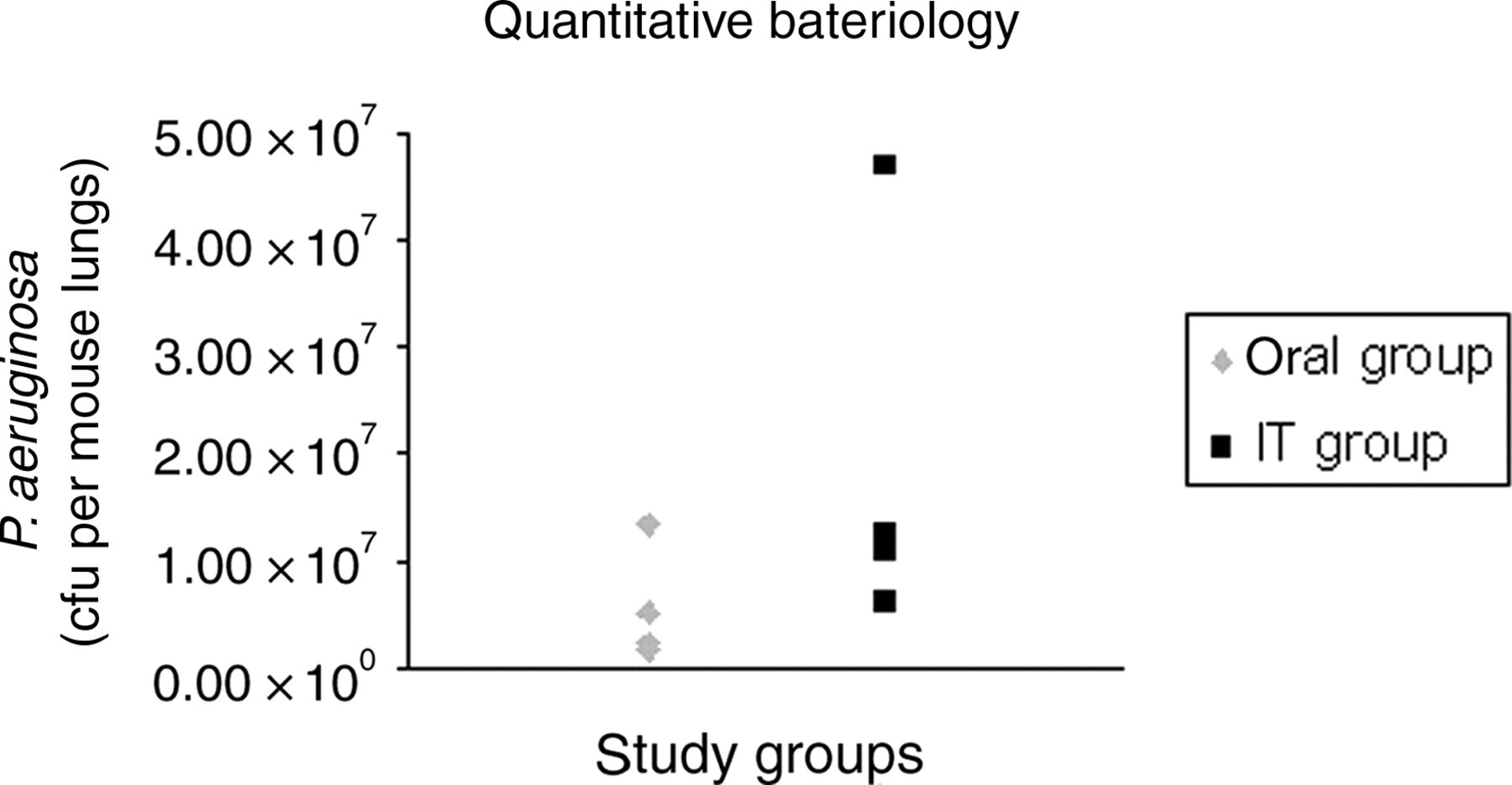
Lung quantitative bacteriology
Lungs were collected from mice that received 5 × 106 cfu P. aeruginosa-laden beads by oral instillation (n = 4) or IT injection (n = 4). The lungs were homogenized and spread in 10-fold dilutions. No significant difference was found between the P. aeruginosa bacterial count in the IT and oral aspiration delivery groups (P = 0.2360) as shown in Figure 7.
Discussion
Several techniques have been developed to establish an acute or chronic lung infection of P. aeruginosa in rodents, such as intranasal instillation (George et al. 1991, Tang et al. 1995, Cheung et al. 2000, Schroeder et al. 2001, Lu et al. 2006), aerosol aspiration (Yu et al. 1998, McCray et al. 1999) or IT injection (Chroneos et al. 2000) of P. aeruginosa. Among these methods, the IT procedure is the most widely used for delivery of either a therapeutic vector or bacteria in the lungs of mice. Although IT injection ensures accurate delivery of therapeutic vectors or bacteria to the lungs, it also has side-effects associated with surgical intrusion, such as pain, local inflammation and occasionally mortality. For example, 10% (2 out of 20) mice were excluded from this study due to mortality after IT injection. In addition, 10% (2 out of 20) mice were excluded from this study due to P. aeruginosa beads leaking out of the trachea during IT injection. The local inflammation caused by IT surgical procedure creates complexity when we want to determine if the cytokine response is related to P. aeruginosa infection or to the surgery. Sometimes, several weeks after receiving a therapeutic vector administered to the lungs by IT procedure, the mice are infected with bacteria by IT injection again to confirm the therapeutic effect of the former administered vectors. The scar tissues caused by the first tracheotomy creates difficulties for the second time to expose the trachea and perform P. aeruginosa-laden beads injection. Moreover, the scientific community is challenged to find less invasive/non-surgical procedures in animal research to prevent unnecessary pain or suffering.
The traditional IT injection method has been replaced with oral and nasal inhalation/instillation methods in an increasing number of mice (Schroeder et al. 2001, McMorran et al. 2001, Guilbault et al. 2005) for administering therapeutic, toxic or infectious agents. However, the accuracy and reproducibility of these less invasive methods had not been addressed in previous articles. With direct visualization and injection into the trachea, we could be reasonably certain that all the animals were receiving equal amounts of the desired agents by IT procedure. Although there is some variability in IT injection caused by leakage of the agent from the injection site or residual agents in the catheter or needle, the variability is minimal and relatively low numbers of animals are used. In comparison, the amount of desired agents actually delivered to the lungs when using the inhalation/instillation models is not clear. Theoretically, the variability resulting from these procedures could be quite high and might mandate the use of a larger sample size. Studies requiring larger sample sizes are especially problematic in difficult-to-obtain mouse models, such as CFTR knockout mice, which are difficult to breed for studies and are a major focus of our research. Furthermore, the benefits of a less painful and invasive procedure are somewhat negated by the need to use a larger sample size and expose more mice to an infection, toxin or therapeutic agents with unknown side-effects.
In our experiments, we modified a previous oral instillation procedure (Walters et al. 2001) by adding the surfactant phospholipid to assist even distribution in the entire lungs. Meanwhile, we compared our oral instillation directly with IT injection to confirm the efficacy and reproducibility of the oral aspiration in the delivery of both a therapeutic AAV vector and P. aeruginosa-laden agarose beads. Our oral instillation procedure took less than 10 min. With isoflurane anaesthesia, we administered either an AAV vector or P. aeruginosa-laden beads directly into the back of the oral cavity. It is a simpler and quicker procedure compared with the IT injection and eliminates the local inflammatory response and decreases surgery-related mortality and discomfort. In an effort to further promote aspiration of the agents into the lungs, we mixed the agents with the phospholipid fraction of surfactant.
Surfactant is a lipid vesicle used for the treatment of neonatal respiratory distress syndrome (Whitsett et al. 1991). It is non-immunogenic and ideal for lung administration. The chemical composition of surfactant includes phospholipids and surfactant-associated proteins. Surfactant plays an important role in the host defence of the lung. It helps bind various bacteria and the surfactant-associated proteins have antimicrobial properties in vitro (Levine et al. 1997, 1998, 2000, Levine & Whitsett 2001). To eliminate potential antimicrobial interactions of the surfactant with AAV or P. aeruginosa-laden beads, we removed the protein fraction and only administered the phospholipid component to aid in lung distribution. To ensure that there was no adverse effect of the surfactant with infection, we performed an in vitro experiment where we mixed the P. aeruginosa-laden beads with the surfactant phospholipid fraction. Serial dilutions of P. aeruginosa-laden beads or a mixture of P. aeruginosa-laden beads and the surfactant were streaked on TSA plates and incubated overnight at 37°C. Bacterial colony counts confirmed that the surfactant phospholipid fraction did not have antibacterial activity (data not shown).
The oral instillation procedure has not been used for the delivery of AAV vectors before. In our study, we demonstrated the efficacy and reproducibility of our modified oral instillation method compared with IT injection. AAV vectors were evenly distributed in the entire lungs regardless of the delivery method used (Figure 2). In addition, hAAT expression in lung homogenates and sera were similar between the delivery methods (Figure 3).
In our experiments with P. aeruginosa delivery, we demonstrated that mice receiving oral instillation of P. aeruginosa-laden beads exhibited similar weight loss, ELF cytokine expression, lung histology changes and bacterial burden as those mice that received P. aeruginosa-laden beads by IT injection. Although cytokine expression in the lung homogenates was significantly elevated in the IT group, the variability among individual mice seen in both groups was consistent; and the degree of inflammation seen in both groups infected with P. aeruginosa far surpassed what we observed in our sterile beads negative controls (data not shown). The reason for the difference in the lung homogenate cytokine expression is unclear. First, the difference could be due to inflammation arising from the surgical procedure. The IT injection can lead to a small, transient inflammatory response, but we have never observed this much of an inflammatory response secondary to IT injection in our negative controls. Most likely, it might arise from the retention of beads in the oral cavity due to the rough surface of the agarose beads. In our P. aeruginosa study, both groups of mice experienced great weight loss. Mice showed lethargic, hunched posture during the first day of administration; and recovered the third day following the administration of P. aeruginosa beads. In the future study, we will perform a dose study that provides the required degree of lung inflammation while minimizing the adverse effects associated with bacterial infection.
In summary, our mouse studies confirmed that a modified oral instillation technique with the surfactant phospholipid component is a reliable technique for the delivery of either AAV vectors or bacteria into the lungs of the mice. It can be applied to numerous mouse studies involving airway delivery of infectious, toxic or other therapeutic agents; it has the advantage of being a simple, quick, non-invasive method that reduces side-effects, such as local inflammation, discomfort and mortality associated with IT injection.