
Abstract
It is now a recognized fact that the practice of conducting a consent (or hospital) post-mortem examination is in decline. There have been many reasons put forth to explain this demise, but the quality of the consenting process is frequently cited as having a high impact. This article focuses on consent practices for post-mortem examinations in England and Wales, and considers if our consent techniques are adversely affecting post-mortem examination uptake. We examine the regulatory compliance of trusts with their statutory obligations by analyzing the Human Tissue Authority's compliance and inspection reports. We further analyze 21 publicly available NHS Trust policies on post-mortem examination consent procedures, and consider whether these are fit for the purpose of meeting the dual needs of clinicians and the bereaved. Despite more Human Tissue Authority inspections, there is a disproportionate rise in enforcement actions, with up to 48% of sampled Trusts exhibiting shortcomings in their legal duties. Additionally, only 52.4% of sampled trusts follow the Human Tissue Authority best-practice model, with 23.8% having no documented procedures. Despite the well founded evidence base for best-practice models, consent practices for post-mortem examinations remains poor and is likely to have a gross adverse effect on the rate of post-mortem examinations. We recommend that NHS Trusts rigorously review their protocols and introduce a team-approach between clinicians and trained bereavement staff in core-consent teams, as the Human Tissue Authority suggests, whilst at the same time placing a strong emphasis on education for junior and senior colleagues alike.
Introduction
‘His parents buried him ten years ago as a shell. It is like grave robbing before being put in the grave. His body had been mutilated.’ 1 This was one of the many piercing quotes to come out of the parent's testimonies to the Bristol Royal Infirmary Inquiry (2001) 2 and Royal Liverpool Children's Inquiry (2000), 3 set up to investigate the retention of organs of deceased children without the knowledge or consent of their grieving parents. Although this practice was legal under the Human Tissue Act 1961, its discovery generated arguably the greatest scandal of the medical profession for decades. Pathologists were particularly vilified and public perception of post-mortem examination was severely damaged, with post-mortem examination rates falling dramatically in the years following the scandal. 4
Whilst it is clear that these inquiries had a demonstrable, immediate effect on hospital post-mortem examination rates, it did not set the trend for the general decline in rates. Since 1979 the number of hospital post-mortem examinations has been declining steadily, from around 42.7% in 1979 to 15.3% in 2001 (the most recent figures available).
5
Is this something to be concerned about? The hospital post-mortem examination is still recognized as a useful procedure.
6
For the medical profession, it has demonstrable benefits:
In medical education for undergraduates and trainees;
6
Auditing the rate of misdiagnoses and the accuracy of death certificates;
7
In clinical trials to evaluate the efficacy of treatment and confirm cause of death;
8
Contributing to our understanding of disease pathophysiology.
8
Moreover, if handled in a sensitive and appropriate manner, there can be tangible benefits for relatives of the deceased, many reporting a sense of ‘closure’ in knowing for certain the cause of death, and a sense of the deceased helping others even in death.
9
The reasons for the long-standing decline, in face of the apparent benefits, are much debated. Whilst previously it had been thought that the opinion of relatives was behind the decline, a recent study 9 suggests it may be the result of fear of the post-mortem examination in the medical community. Reasons for this include medico-legal concerns and assumptions that relatives would not want the deceased's body further disturbed. 9 Yet in one study, perhaps surprisingly, religious objections to post-mortem examination occurred only twice in 23 deaths. 9 Could it be the case that clinicians themselves are responsible for the decline they lament?
This article will seek to examine the issues that still surround seeking consent for hospital post-mortem examinations in England and Wales. By identifying the nature of consent, how far NHS Trusts comply with their legal and ethical duties to obtain consent in an appropriate manner, and identifying areas for improvement, we may be able to answer the deadly question: are we killing the hospital autopsy with poor consent practices?
Methods
To prepare this review we obtained compliance data from the Human Tissue Authority's website (
The nature of consent: Ethical and legal basis and relationship to the Human Tissue Act 2004
Consent is not an unfamiliar term to clinicians; the common law duty to obtain consent for any medical procedure on a living person has existed for decades. 10 However, until 2004 this did not extend to the dead; under the Human Tissue Act 1961 all that was required for any permitted activity on deceased tissue was a ‘lack of objection.’ 11 In the living, if consent is not obtained or obtained incorrectly (for example through coercion) then one would find themselves open to the criminal charge of assault or the torts of battery or negligence. 12 As it is legally impossible to assault or batter a dead body, the 1961 Act contained no penalties. Thus, anyone wishing to pursue a claim was required to find novel legal grounds, such as the tort of wrongful interference with the right and duty to possess a body for burial 12 (as in the case of Re Organ Retention). 13
The Human Tissue Act 2004
14
removed this ‘no objection’ requirement. Instead, it demands that consent is at the core of all activities permitted by the Act on tissue from the deceased, including conducting a post-mortem examination. Valid consent retained its common law meaning (until updated by the Mental Capacity Act 2005)
15
but a clear hierarchy of consent now exists:
The deceased's consent in life carries the greatest weight; The consent of a representative nominated in life has the second greatest; Finally, at the bottom of the scale, consent of a person in the highest ranking qualifying relationship.
In turn, these qualifying relationships have an additional hierarchy, beginning with a spouse or partner and ending with a friend of long-standing).
As the ambiguity regarding tort remained, and given the strength of public feeling, criminal penalties for breaching the Human Tissue Act's consent requirements were introduced for the first time, with the maximum penalty being three years imprisonment and a fine.
14
Irrespective of the Human Tissue Act, the need for consent is invoked in order to protect the non-proprietary interests of relatives of the deceased. Hardcastle 12 argues that there are two such protected interests in English Law: Autonomy and Article 8 of the Human Rights Act 1998 (Respect for Freedom of Private and Family Life). Hardcastle goes on to explain that whilst it is unclear to what extent autonomy in death is protected under English Law, in Re Organ Retention 13 Gage held that the non-consensual retention of a deceased child's brain would constitute an infringement of Article 8. 12
At this point it is important to highlight the clear distinction between the hospital post-mortem examination and the Coronial post-mortem examination; in the latter, issues of consent are largely irrelevant as post-mortem examinations are performed under authority of the Crown through the Coroners Act 1988 16 (as amended) and so are not considered here. The distinction can be seen when examining the rate of Coronial post-mortem examinations; in 2010 44% of deaths reported to the Coroner (and 20.6% of all recorded deaths in England and Wales) underwent a Coronial Post Mortem. 17,18 In comparison to the 2005 Coronial Post Mortem rate for all recorded deaths of 22%, this figure has remained stable at a much higher rate than hospital post-mortem examinations. 19
The Human Tissue Authority and codes of practice
Having established exactly what the absolute minimum requirements for valid consent are, in law, we now turn to the physical implementation of these requirements. In the UK this currently falls to the Human Tissue Authority, a statutory body funded by the Department of Health whose functions and powers are set out in Part 3 of the Human Tissue Act. 14
To achieve its aim of enabling establishments to comply with the Human Tissue Act, the Human Tissue Authority publishes various Codes of Practice documents 18 to offer logistical guidance. The Codes of Practice are approved by Parliament but are not legally binding; they retain legal persuasion, in that a failure to adhere to the codes of practice would be suggestive of a failure to meet the requirements of the Human Tissue Act and potentially lead to enforcement action (or in the failure of a legal duty, prosecution). 20 Of the nine codes, the two that are most relevant to the post-mortem examination consenting process are Code 1: Consent 20 and Code 3 Post Mortems. 21 The codes are extensive, and highlight what establishments should do in order to meet the requirements of the Human Tissue Act; they are, however, deliberately open ended and the significance of this is discussed later. However, for the most part these are comprehensive, useful guidelines that place a clear emphasis on both the needs of clinicians and the bereaved.
Compliance of NHS Trusts with statutory requirements
As part of its enforcement remit the Human Tissue Authority performs inspections on establishments who are licensed to perform post-mortem examinations under the Human Tissue Act, and reports its findings annually through ‘Summary of Compliance’ reports. These reports are public documents and are freely available through the Human Tissue Authority website. 22 For the purposes of inspection, the Human Tissue Authority uses three main indicators for consent requirements, C1, C2 and C3 (which are summarized in Figure 1). These provide a succinct method of generating quantitative measures of compliance with the Human Tissue Authority's minimum standards. The results of the past three year's reports (2008–10) are summarized in Table 1; over the period of 2008–10 the Human Tissue Authority has inspected all establishments licensed for the purposes of conducting a post-mortem examination. 23 The data suggests there is an increasing level of scrutiny with increased site visits by the Human Tissue Authority, however this is accompanied by a disproportionate increase in the number of conditions and enforcement actions imposed by the Human Tissue Authority.
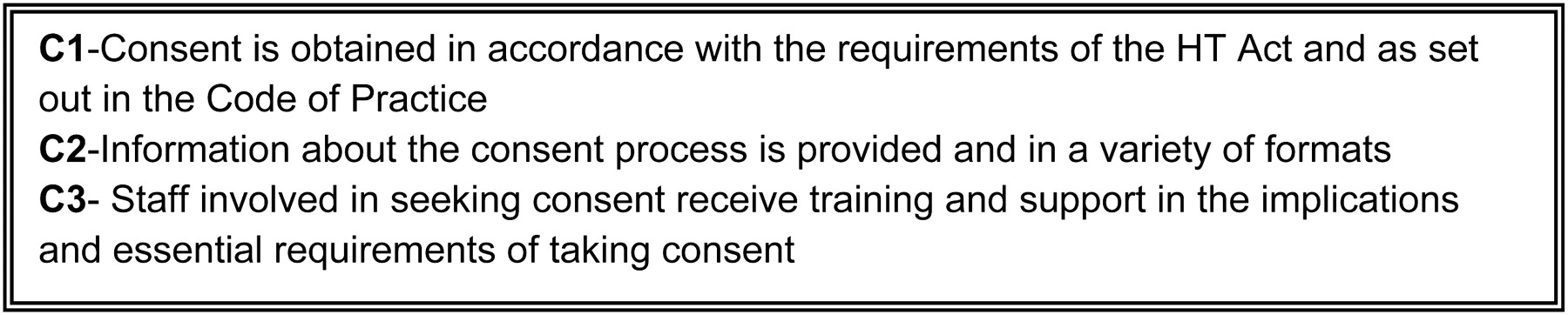
Human Tissue Authority Consent standards for measuring compliance with the Codes of Practice and Human Tissue Act24
The Summary Reports comment that the majority of establishments follow the regulations generally well in all areas of regulation for post-mortem examinations. 23 However, there were numerous concerns with practice in the area of consent, particularly standards C1 and C3. When we analyzed the most recent individual reports of 23 Trusts inspected over the period November 2010 to February 201122 (Table 2), we found that:
48% were failing to follow the Human Tissue Act or Codes of Practice requirements for obtaining consent (and in three cases this was judged to be a major shortcoming) (C1);
17% did not provide, or make available, adequate information to relatives in the consenting process (C2);
26% were failing in the provision of training to staff who undertook the consent process (C3).
On examining the remarks in the inspection and summary reports, frequent shortcomings included:
Consent being recorded on forms that were out of date or did not follow the Codes of Practice; many trusts seemed unaware of the Human Tissue Authority model consent form;
24
The lack of an appropriate Standard Operating Procedure for staff, and in a surprisingly large number of cases the lack of any Standard Operating Procedure at all, detailing the practical measures relating to consent, as required by Human Tissue Authority policy;
23
Consent being incorrectly obtained from a next of kin rather than the highest ranking qualifying relationship, with training being described as ‘inconsistent’ in a recent Human Tissue Authority policy.
25
Whilst there have been examples of good practice, the general picture is one of regulatory non-compliance, underdeveloped training and disparate practice that does not serve the needs of the bereaved or the medical profession at large.
Diversity of function in the NHS
Even though there are no frank violations of the Human Tissue Act, general practice in this area appears poor. Even if Trusts comply fully with their statutory duties, this seldom makes for best practice in any scenario. In the Summary of Compliance 2008–9 report, 24 the Human Tissue Authority argues that they are ‘careful not to be too prescriptive so that [the licence holders] may be empowered to develop tailored solutions to achieve regulatory compliance’. The Human Tissue Authority correctly recognizes that taking a completely prescriptive approach would likely be detrimental to the varying needs of establishments, and instead outlines ‘what’ needs to be achieved for compliance rather than ‘how.’ This approach can, however, have risks; it can lead to wide ranging poor-practice for Trusts that spend little time and few resources on an area that is in decline. 24
To examine how this open-ended approach from the Human Tissue Authority influences Trusts, we examined the Standard Operating Procedures for Obtaining Post Mortem Consent of Trusts in England and Wales. The Human Tissue Authority requires every trust to have a Standard Operating Procedure for obtaining consent for post-mortem examination. 25 Following an internet search, we obtained 21 publicly available Standard Operating Procedures for Post Mortem Consent from Trusts throughout England and Wales. The Standard Operating Procedures were analyzed if found to be within their scheduled review date (suggesting that they are currently in force), however, it is acknowledged that there may have been variations to these Standard Operating Procedures since their publication and they may not reflect the current version held by Trusts. This method of data extraction did allow random sampling as all retrieved policies with references to post-mortem examinations were examined. However, this is by no means intended to be a comprehensive review, rather it is a snapshot of the current approaches found in the NHS.
The main approaches employed by Trusts were as follows (Table 3):
Methods employed by 21 NHS Trusts in England and Wales to seek consent for PME
A team approach, with a clinician lead supported by an individual trained in the requirements of the Human Tissue Act and bereavement counselling (usually a bereavement officer or similar); eleven trusts used this approach, constituting just over half of the Standard Operating Procedures. In two of these eleven trusts, bereavement officers led the discussion supported by clinicians;
Clinicians acting alone to take consent in four cases; two of which required a second team member to act as advocate for the family;
One Trust used a bereavement officer acting independently from clinical staff;
The remaining five had an unclear approach, as the policy was insufficiently detailed or did not specify an approach. If a separate policy detailing the procedure existed, this was not explained in the Standard Operating Procedure.
The quality of the Standard Operating Procedures varied greatly, but many were poor. Two policies were bespoke; these generally represented the most comprehensive policies, going into detail far beyond that required by the Codes of Practice. The majority of policies explained the regulations laid down by the Codes of Practice, but failed to outline key practical procedures, such as how consent should be taken, or how a change in the consent decision would be relayed to the pathologist. Some trusts contained small sections dedicated to post-mortem examinations in their generic consent policy; these often did not cover as much detail as the bespoke policies and little emphasis was placed upon the requirements under the Human Tissue Act.
Discussion and recommendations
We see an enormous diversity of function when a snapshot of practice in the NHS is taken. Thus, the key questions remain: what actually makes good consent for post mortem examinations and are we doing it?
The phenomenon of the declining post-mortem examination rate is shared in most countries that require explicit informed consent; 6 in the UK the most recent figures (2001) show a 27.4% decline from 1967. 6 Stock et al. 4 demonstrated that the key to changing this lies with the quality of consent process. The findings here suggest that approaches to post-mortem examination consent are poor and disparate and certainly nowhere near optimal, despite the general spirit of compliance with the Human Tissue Authority Codes of Practice. There is very little emphasis on the importance of quality consent for post-mortem examinations and a potential ignorance of the benefits this could have. In the Trusts analyzed here, some had no clear policy on consent, others were following out of date practice. Of those that were compliant, there appeared to be two main approaches: clinicians alone, and clinicians supported by bereavement officers, or similar (Table 3).
To achieve best practice, we recommend the ‘treating clinician supported by trained staff’ model (with an important caveat surrounding education); this is the example identified by the Human Tissue Authority as ideal, 26 yet only half of sampled Trusts follow this. Clinicians, whilst arguably experienced in consenting the living, are unlikely to be well versed in the plethora of additional requirements for post-mortem examination consent. Indeed, the 2008–9 Compliance report 24 notes that proficiency in seeking consent in other areas is not a substitute for specific post-mortem examination consent training. Moreover, the experts in the post-mortem examinations themselves, pathologists, have little desire to be involved with the consent process. 27 The way these barriers are overcome is by supplying training on consent matters to a small, permanent team of staff. Thus, Trusts can ensure that the legal requirements for consent are being met and additionally this team can promote consent techniques amongst the clinicians they come in to contact with. 28 At the same time, the rapport between the bereaved and the treating clinician is not lost to the consent procedure; indeed this has been shown to be a key factor in success. 29 This procedure also makes logistical sense: in a study by Cairns et al., 28 the use of a Core Consent Coordinator (with responsibility for managing the consent process) when obtaining consent for post mortem brain retention increased the success rate from 0% to 71.5%. Thus, this approach seems to be solidly grounded in evidence.
The problem in this approach is the effect it may have on clinicians, especially junior clinicians. Tsitsikas et al. 9 demonstrated that families are generally receptive to post-mortem examinations, and a far greater factor in their decline is the reluctance of staff to request them; when post-mortem examinations were routinely requested, the consent rate increased to 89%. Whilst in 2003 Burton 5 demonstrated that the majority of consent was taken by pre-registration or senior house officer grades, now almost all the policies mandate that it must be a senior clinician, usually of registrar grade or above. This has its benefits, Stock et al. 4 have shown that the seniority of the clinicians is an important factor for gaining consent; this is increased when that person has a rapport with relatives. 29 This evidence taken together shows that whilst senior clinicians are the best choice to counsel relatives for consent, removing responsibility for consenting from junior clinical staff runs the risk of further reducing their belief in the value of autopsy. 29 Programmes of education and post-mortem examination viewing for junior staff are frequently cited as key positive factors in improving consent rates. 4,29 Thus, whichever method is chosen to consent for post-mortem examination, the education of junior staff is paramount, as they often have the role of ‘first on scene’ and act as an impromptu counsellor for the bereaved. If they do not believe in the autopsy's value, the opportunity to counsel relatives appropriately may be lost before it has even existed.
Importantly, whilst we can look at the evidence suggesting effective methods for obtaining post-mortem examination consent, until a detailed survey of patients' and relatives' experiences of the consent process for post-mortem examinations has been carried out, we will not know for certain which is the best method. We will also not know to what extent Standard Operating Procedures, however well-written, are followed by staff on the ‘shop floor’; this further emphasizes the need for formal audits to corroborate these findings.
Conclusions
The autopsy, or post-mortem examination, can be traced back to the very origins of medicine and remains a crucial element in solving many of the puzzles that confuse us so regularly in our daily practice. Post-mortem examinations can also be constructive for the bereaved, who can seek closure in a certain cause of death. Sadly the practice is now in decline; whilst the reasons for this are much debated, we most likely are killing off any chance of a renaissance for the autopsy with our reluctance to request them and our poor attitude to consent. By adopting an evidence-based team approach, clinicians can avoid the stigma they alone attribute to post-mortem examinations, achieve regulatory compliance and increase the post-mortem examination consent rate. In doing so, we may then breathe some life back into a faithful ally.
DECLARATIONS
Competing interests
None declared
Funding
No funding or sponsorship was obtained in the preparation of this manuscript
Ethical approval
Not applicable
Guarantor
NN
Contributorship
The two authors are justifiably credited with authorship, in accordance with the guidelines. JH-concept of the study, identification of source materials, analysis of information, drafting of manuscript and tables and figures, final approval of manuscript; NN- concept of the study, identification of source materials, critical revision of manuscript, final approval of manuscript
Acknowledgments
None