
Abstract
In this review, we make the case for evidence-based medicine (EBM) to include models of disease underscored by evidence in order to integrate evidence, as it is currently defined, with the patient's unique biology. This would allow clinicians to use a pathophysiologic rationale, but underscoring the pathophysiological model with evidence would create an objective evidence base for extrapolating randomized controlled trial evidence. EBM encourages practitioners not to be passive receivers of information, but to question the information. By the same token, practitioners should not be passive executors of the process by which information is generated, appraised and applied, but should question the process. We use the historical examples of the evolution of EBM to show that its subordination of a pathophysiological perspective was unintentional, and of essential hypertension to illustrate the importance of disease models and the fact that evidence supporting them comes from many sources. We follow this with an illustration of the benefits a pathophysiological perspective can bring and a suggested model of how inclusion of pathophysiological models in the EBM approach would work. From a practical perspective, information cannot be integrated with the patient's unique biology without knowledge of that biology; this is why EBM is currently so silent on how to carry out its fourth stage. It is also clear that, regardless of whether a philosophical or practical definition of evidence is used, pathophysiology is evidence and should be regarded as such.
Introduction
‘Grant me the strength, time and opportunity always to correct what I have acquired, always to extend its domain; for knowledge is immense and the spirit of man can extend indefinitely to enrich itself daily with new requirements.’ The Oath of Maimonides 1
Knowledge provides a basis for a belief or action. In philosophy, it is usually defined as a group of true, justifiable and actionable beliefs. Evidence in this context is anything which provides justification for a belief. Evidence, from a practical perspective, is defined by its purpose; it is information that reduces uncertainty in the context of decision-making. However, this functional definition is constrained by the epistemological framework from which it is derived. Evidence-based medicine (EBM) uses a hierarchy which narrows the definition of evidence to information arising from systematic reviews and randomized controlled trials (RCTs). EBM encourages practitioners not to be passive receivers of information, but to question the information. By the same token, practitioners should not be passive executors of the process by which information is generated, appraised and applied, but should question the process. The price for not doing so is that one's thoughts and actions become shaped by, as MacIntyre put it, ‘unrecognised theoretical ghosts’. 2 EBM assumes a number of philosophical positions, and it is important for practitioners of EBM to be aware of them and to question them.
If one defines knowledge as a set of true, justifiable and actionable beliefs, evidence can be loosely defined as anything which provides the justification. No single type of evidence can claim to be absolutely foolproof, to always establish ‘truth’. Clinical knowledge draws its justification from a range of sources, which include clinical experience and scientific research, and the weighing of each is a nuanced process which defies any attempt to be simplistically captured. EBM has, however, espoused a method of critical appraisal which is simplistic in its use of an evidence hierarchy which ranks quality based on the presence and quality of randomization and control. This has created an artificial separation between ‘evidence’, which is effectively defined as information from RCTs, systematic reviews and observational studies, and pathophysiology, which is explanatory information about mechanisms of disease. The origins of this separation lie in the philosophical assumptions of EBM methodology which view randomization, control and repeatability as sufficient conditions to establish causality, and the use of a frequentist interpretation of the probability calculus (Table 1). It has persisted partly because the paradigms of EBM have become firmly established during the rapid rise of the EBM movement, and partly because a perceived benefit of EBM has its challenge to expert opinion which has, historically, been inextricably linked with pathophysiological rationale.
Interpretations of the probability calculus
RCT = randomized controlled trial
The separation between evidence and pathophysiology has no logical basis. Pathophysiology can provide justification for a belief and reduce uncertainty in the context of decision-making; it therefore fits the definition of evidence, and is evidence. From a practical perspective, an understanding of mechanism (i.e. of the latest models) is important at two stages in the current EBM approach (Table 2). First, when assessing the validity of a finding, it is important to ask whether it is biologically feasible. This was illustrated in a trial of remote intercessory prayer in bloodstream infections which demonstrated effectiveness of the intervention even though it was delivered 4–10 years after the patient's illness! 3 It was published as a cautionary example that a good quality trial can yield erroneous results because a single randomization may not balance out all confounders. The argument raised is that the establishment of causality requires an explanatory mechanism. Second, evidence needs to be integrated with the patient's unique biology. However, EBM is silent about how to identify the best models of biology with which to integrate the evidence (as EBM currently defines it); this task has, ironically, been directed back to expert opinion and has been fraught with difficulties. We argue that the adoption of the best disease model, continuously underscored by evidence to inform the reassessment and development of the model, could provide an evidence base for extrapolating quantitative information about benefits and harms.
The current EBM methodology
A further unintended consequence of the division between evidence, as it is currently defined, and pathophysiology, is that the former has been prioritized in continuing medical education, evidence databases and clinical decision support tools. In addition, many undergraduate curriculums no longer include a pathology course. A potential consequence of this is that clinicians may be kept up to date about what the latest treatments are, but not about current understanding of their mechanisms or the underlying disease process. Unless doctors seek out and remain up to date about this information on their own (only feasible for a small subset of conditions in which the clinician has a particular interest), this could have two practical implications. First, doctors would not have the latest information to anticipate benefits or harms when deciding whether a treatment recommendation is applicable to their patient. Second, doctors would be unable to provide their patients with the very latest understanding of their disease and treatment. These problems are compounded by the exponential growth of the medical and scientific literature.
The evolution of EBM
It is worth tracing the history of how RCTs and the evidence-based movement came into being, as this history illustrates that the subordination of the pathophysiological perspective was unintentional. The history is summarized in Figure 1. 4–8
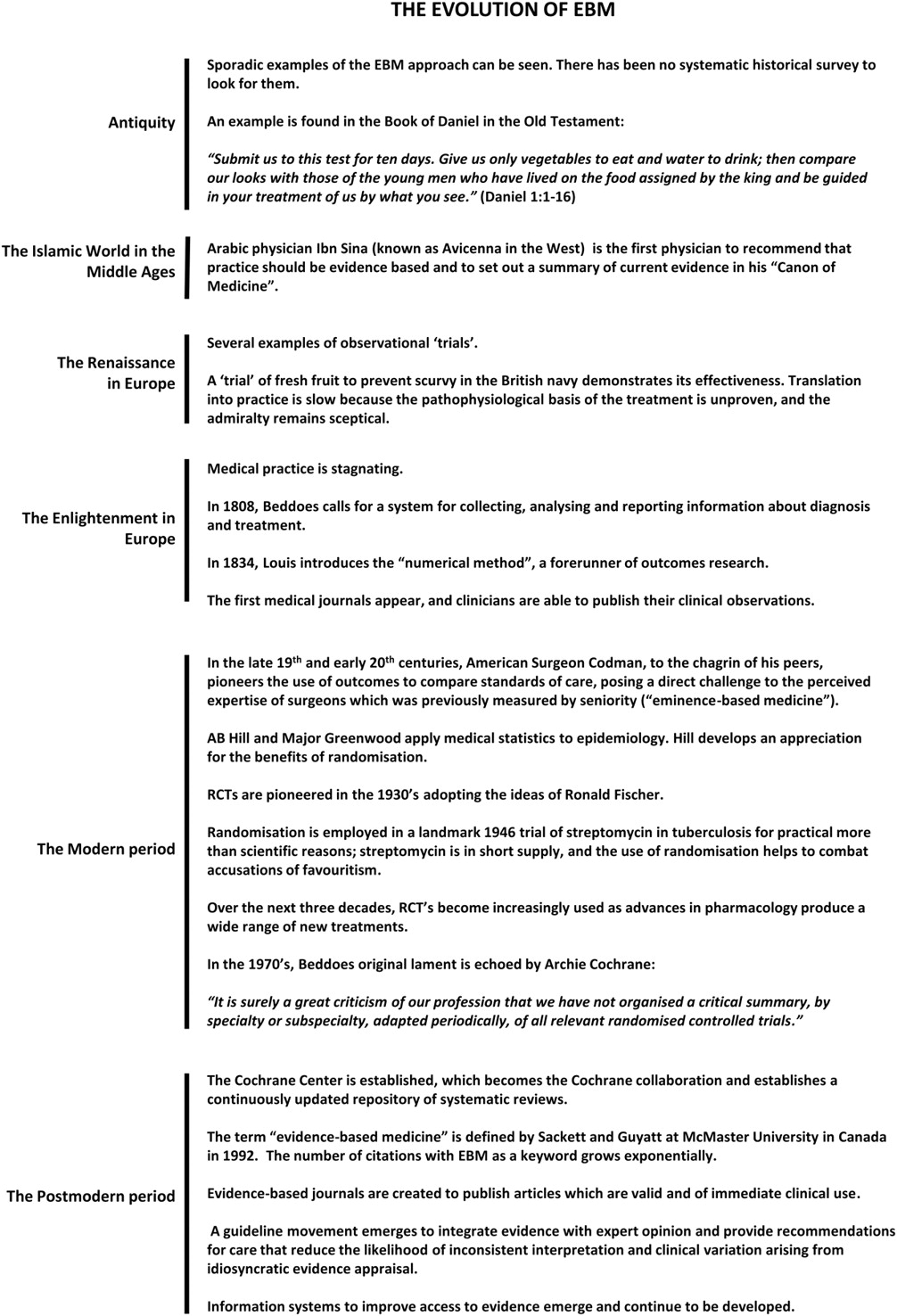
Historical milestones in the evolution of EBM
RCTs emerged by applying the ideas of Ronald A Fisher, who postulated that randomization, control and repeatability are sufficient conditions to establish causality. These conditions for causality have since been superseded by the more robust Bradford-Hill criteria (Table 3), but EBM methodology continues to rely on Fisher's postulates. The originators of RCTs needed to choose the appropriate statistics, and since these all relied on probability, the best interpretation of the probability calculus had to be chosen. Four interpretations of the probability calculus are possible (Table 1), but RCTs from their inception adopted the frequency interpretation. This was mostly a practical decision; the interpretation allows events to be related to each other and is therefore well-suited to the study of outcomes and the quantification of the harms and benefits of different clinical management approaches. The frequency interpretation implies a hierarchy of evidence which places RCTs as the gold standard (Table 4). The logical and subjective theories, by contrast, relate theory to evidence, and, if used, would have implied a hierarchy which placed the best explanatory theory as the gold standard. 9 The frequency interpretation had the limitation that there was no robust way to extrapolate RCT findings to another population (because there is no model with which to do so) or to an individual (because this is impossible in the frequency interpretation); clinicians could only inform their patients about probabilities of outcomes. The adoption of Fisher's postulates and the frequency interpretation made the methodology of EBM the only one in the scientific world to give the lowest rather than the highest priority to the development of a good explanatory theory. The extent to which this has been a strength or a weakness has been much debated. The appeal of the double-blind RCT was that it promised to put clinical decision-making on an objective, more scientific basis by replacing clinical judgement with statistics and standardized methodology. The primary concern motivating this change was the need to establish standards of practice. Its methodology offered the promise of an accepted standard to which treatments could be held, and the need for this became increasingly apparent as more and more treatments started to appear. Its ability to address problems of bias was also very appealing.
The Bradford-Hill criteria for the establishment of causality, using insulin as an example
An example of an evidence hierarchy. Many hierarchies have been defined, and none are universally accepted, but all rank evidence in the same general order
As the system for developing drugs evolved, regulatory agencies came to require RCT evidence of a drug's effectiveness. At the same time, the pharmaceutical industry recognized the persuasive power of positive RCT evidence in their marketing, and the threat, as they perceived it, of negative evidence. This development meant that many RCTs were designed and conducted to bring a drug to market; while some of these also answered clinically important questions, some did not, and opportunities to study clinically important questions were lost. More worryingly, the need to accurately and comprehensively report all trial data, positive or negative, came into conflict with the financial interests of the industry, posing a threat to the balance and reliability of the knowledge base. Finally, the use of RCT data for advertising contributed to the trapping of many new therapies into a cycle of hype and disillusionment which precluded a rational consideration of the evidence. RCTs are not exclusively run by industry, but the contribution of industry to RCT evidence has been substantial, as running good-quality trials is resource-intensive. Other biases which emerged included technological (methodological), gender, cultural and publication biases. 10–13 The dream of an unbiased evidence base, envisaged by its early pioneers, remains to be fully realized.
The adoption of the methodology of randomization and control brought the consequence that the pathophysiological perspective was subordinated. There are some celebrated and often-cited justifications for this. A cautionary tale of the effect of confounding factors is provided by the use of HRT to prevent coronary artery disease. This intervention had a solid pathophysiological rationale, and showed benefit in observational studies. However, RCT evidence established that HRT has no impact on cardiovascular risk. 14 Pharmacologic suppression of arrhythmias after myocardial infarction was found to increase the risk of death. 15 In acute lung injury, improvements in oxygenation with inhaled nitric oxide did not improve survival. 16 These examples show that pathophysiological rationale, when acting alone, does not always get it right, and RCT evidence can establish what the actual benefits and harms are. However, these examples provide a case for testing pathophysiological rationale (the basis of all good science), not abandoning it.
The pharmaceutical industry first adopted and then abandoned the approaches of experimental pharmacology and pathology, instead deciding to create high-throughput pipelines to develop compounds which bind to receptors of interest. As a result, disease models were abandoned both at the conception of the treatment (by the pharmaceutical industry) and at its final test (by the EBM movement), being consigned to the phases in between. This approach has yielded few new treatments, and we have learned the hard way that translational medicine requires the use of models if it is to succeed. This fact has now been recognized and there is a concerted effort underway to ground translational medicine in pathophysiological and pharmacological approaches. However, the same has not happened in the EBM movement, even though it faces an analogous challenge: to extrapolate and integrate the information it generates about benefits and harms.
There is no doubt that the EBM movement has had notable successes. The death rate from cardiovascular disease in the US almost halved between 1980 and 2000; half of this reduction was attributed to evidence-based therapies. 17 Guidelines based on EBM have helped to achieve a large and sustained decrease in the morbidity and mortality produced by anaesthetics. 18 Conversely, groups who are under-represented in clinical research experience worse outcomes. EBM has also increased the uptake of new therapies. It is worth commenting, as an aside, that EBM is curiously unsuited to examination by its own methods, because it would be hard, if not impossible, to do an RCT with EBM as the intervention. The success of EBM is, ironically, an argument against the rigidity of its evidence hierarchy. All of the evidence in favour of it would be rated in the hierarchy as ‘poor-quality’, and yet proponents of EBM would not believe that the significance of their achievements is diminished by the manner in which those achievements have been measured. We do not deny the successes of EBM and do not propose that the methods of EBM need to be abandoned. Rather, we propose that they need to evolve to be more inclusive and nuanced. To illustrate why, it is worth considering some lessons from history about how knowledge is generated.
Knowledge generation: vignettes from history
The practice of medicine has traditionally relied upon the construction of a model that explains how the human body functions, how that function is disturbed and how it can be restored. The model is articulated and advanced by a combination of inspired insights, experiment and the slow accumulation of experience. Ever since the Zhou dynasty in China and the teachings of Plato and Aristotle in Ancient Greece, questions of how to assess and affirm medical and scientific aims have been addressed to expert opinion, and so it is that expert opinion has had a profound influence on the development of the knowledge base. Throughout the history of medicine its influence has been mixed, capable of producing great advances but also of resisting advances and creating setbacks. We have chosen the historical example of essential hypertension as an illustration that ‘best evidence’ can come from a myriad of sources which we ignore at our peril. 19 Figures 1, 2 and 3 summarize the key historical milestones. 20–38
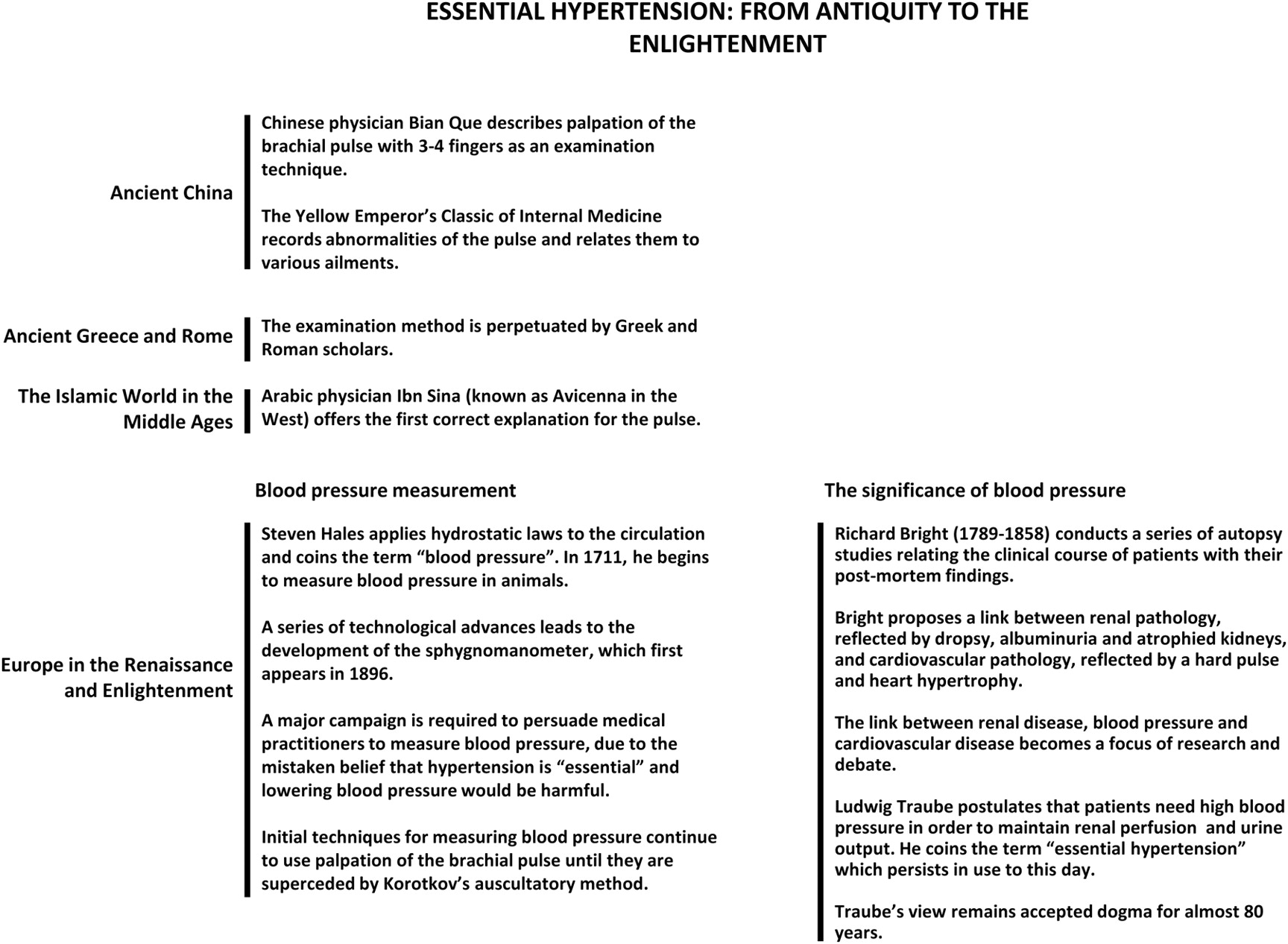
Historical milestones in the early evolution of concepts relating to essential hypertension, covering the period from the early concepts developed in antiquity to the Enlightenment
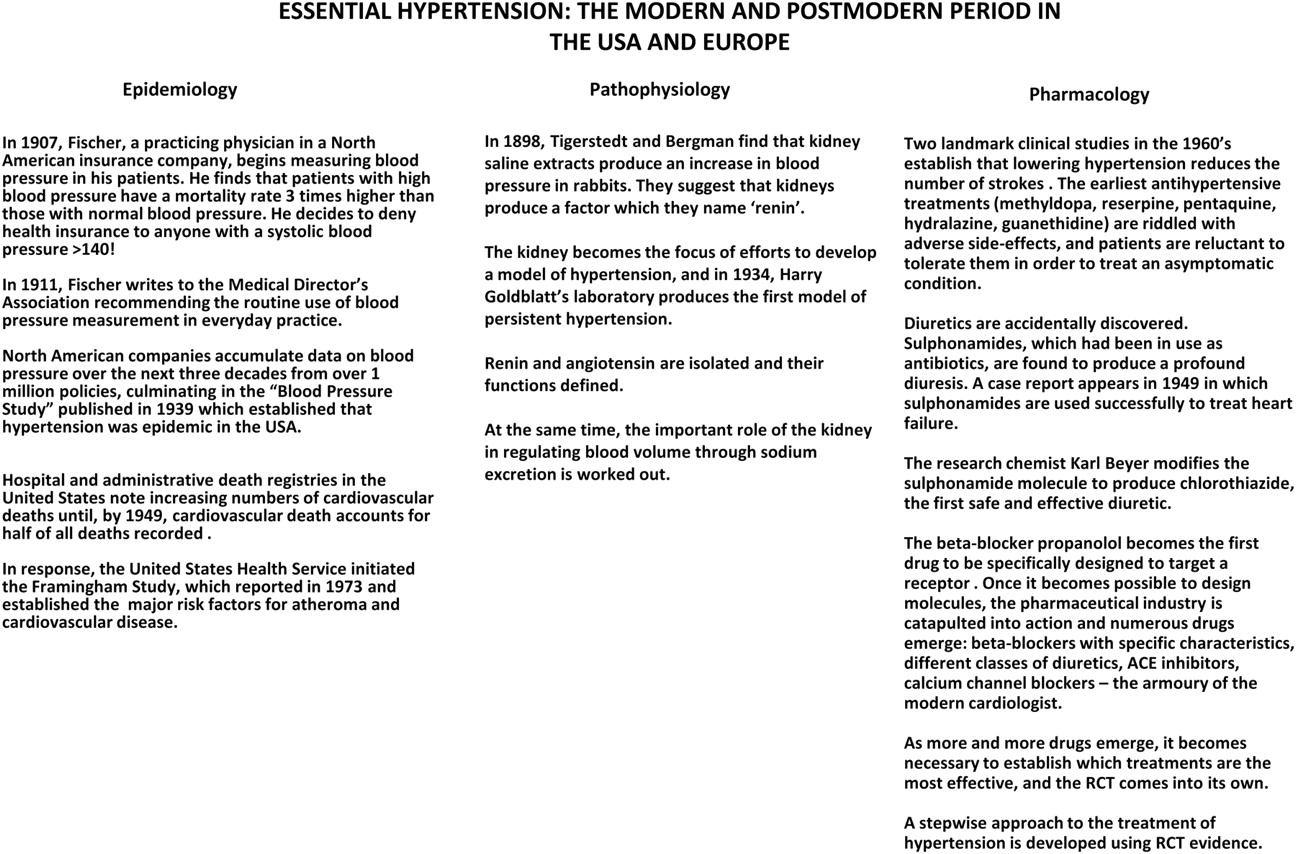
Historical milestones in the development of a treatment strategy for essential hypertension in the modern and postmodern periods. Parallel advances in epidemiology, pathophysiology and pharmacology are laid out
The Philosopher of Science Thomas Kuhn first coined the terms ‘paradigm’ and ‘paradigm shift’ to describe how scientific advances occur, 39 and the history of science shows that it is easier to articulate or advance a paradigm than to challenge it. As Max Planck once put it, ‘a new scientific truth does not triumph by convincing its opponents and making them see the light, but rather because its opponents eventually die, and a new generation grows up that is familiar with it’. This dynamic can be clearly seen in the paradigm shift that occurred from ‘hypertension the essential adaptation’ to ‘hypertension the risk factor’ which took almost 100 years to complete. The challenge to the old paradigm came from many different sources: expert opinion, non-expert opinion (Korotkov was a trainee when he published his landmark paper, and he never published again), science that relied on the development of models, RCTs that abandoned models and, every now and then, serendipity. Patient preference played its part in creating the demand for new treatments; commercial interest played its part in financing them. No one source could claim to be the supreme source of evidence. No single group could claim to be the sole mover of progress. The most important lesson about this history is that the development of the correct explanatory mechanism was crucial not only to develop effective treatments for hypertension, but to make the case for treating hypertension in the first place.
Explanatory models underscored by evidence: an evidence base for extrapolation
A major disadvantage of RCTs is that, by abandoning the use of models, extrapolation of their findings to other populations and situations becomes challenging, as does the anticipation of unexpected or unintended effects. This is the problem of ‘external validity’, or of establishing the capacity of the treatment to have an effect in a dose, formulation and context other than those tested by the trial. 40 Extrapolation of findings may relate to differences in dose, timing, duration or a wide range of patient factors including age, co-morbidities and polypharmacy.
Thompson has proposed that evidence should be used to continuously inform and develop the best explanatory model. 9 Mathematically this can be done by employing Bayesian statistics. This is a statistical approach which relates theory to evidence. We propose that this approach can be used to provide an objective basis for integrating information from RCTs and observational studies with the patient's unique biology. In this approach, the gold standard would be the best explanatory model of the disease and the mechanism of action of the treatment. Evidence underscoring this model, drawn from the full spectrum of basic, translational and clinical research, would be used to continuously update, refine and challenge the model. The model would be available for practitioners of EBM to use in deciding when and how to extrapolate evidence to other populations. The existing evidence base of systematic reviews, RCTs and observational studies would exist alongside explanatory models. Nuanced decisions would need to be made about when to rely on the model to extrapolate information derived from another population, and when to repeat studies in the target population. The development of the best explanatory model would be applicable to any condition and would not be limited by how common the condition is. It could therefore act as a source of evidence where none currently exists. The development of the best explanatory model is the focus of biological research; the systematic use of Bayesian methods would provide a method of testing the best explanatory theory which is independent of expert opinion, thereby preserving this perceived benefit of EBM while broadening its conception of evidence. The potential benefit of this approach in a range of different situations is illustrated in Tables 5–7. 41–52
Benefits of the use of disease models in three clinical settings
Benefits of the use of disease models in the practice of EBM
Benefits of the use of disease models for patient education and new knowledge generation
Conclusion
Evidence is, and should be, viewed as anything which provides justification for a belief (its philosophical definition), or which reduces uncertainty in the context of decision-making (its practical definition). The examples discussed in this review show that the artificial separation between pathophysiology and evidence has no logical basis. In addition, pathophysiology has a practical benefit to offer by informing the integration of evidence, as it is currently defined, with the patient's unique biology. The adoption of Bayesian approaches to inform pathophysiological rationale would help to place it on an objective basis, thereby preserving the independence from expert opinion of the EBM approach. We do not expect that this approach will be a panacea for the limitations of EBM, and the ultimate test will be whether the approach improves patient outcomes. There is probably no single answer to the question of whether the benefits of EBM seen so far would have been greater or lesser if EBM had used an alternative approach or defined its hierarchy differently. Nevertheless, from a practical perspective, information cannot be integrated with the patient's unique biology without knowledge of that biology; this is why EBM is currently so silent on how to carry out its fourth stage. It is also clear that, regardless of whether a philosophical or practical definition of evidence is used, pathophysiology is evidence and should be regarded as such.
DECLARATIONS
Competing interests
None declared
Funding
None
Ethical approval
Not applicable
Guarantor
RM
Contributorship
Both authors contributed equally
Acknowledgements
None