
Abstract
‘Is the rich world aware of how four billion of the six billion live? If we were aware, we would want to help out; we'd want to get involved.’ Bill Gates
Safeguarding good health is not simply the province of individual countries like the UK in today's globalized and interdependent world. 1 A healthy population is fundamental to prosperity, security and stability, and is a cornerstone of economic growth and social development. Moreover, poor health does more than damage the individuals themselves – it is a threat to the economic and political interests of all countries, determined by factors which show little respect for national boundaries – such as international trade, climate change, pollution, conflict, environmental degradation and poverty. Therefore, effective healthcare plays a key role in economic and social wellbeing, as well as the prevention and treatment of diseases.
Ameliorating global health inequalities, as discussed briefly by Sir Kenneth Stuart and Lord Soulsby of Swaffham Prior in their series, 2 is a key part of international multidisciplinary solutions, especially given the sheer scale of abject poverty throughout the world. But, as the authors explore in some detail, health is a complex issue with many stakeholders. For example, tackling the first Millennium Development Goal (eradicate extreme poverty and hunger), 3 although inextricably linked to health, only requires healthcare provision to treat its complications. Because so many sectors affect health, and so many agencies are involved in healthcare, improving health around the world, as previously set out in the UK Global Health Strategy, requires creative, joined-up partnerships within the UK, and between the UK and a host of other stakeholders, from the European Union (EU) and the United Nations (UN) to non-governmental organizations (NGOs), foundations, academia and business. 1
There has been some progress – philanthropic global NGOs such as the Gates Foundation 4 should be lauded for their efforts in tackling a wide range of causes in conjunction with the work done by official bodies like the World Health Organization (WHO). However, as well as focusing solely on infectious diseases and the increasing burden of non-communicable diseases, 5 there is a parallel need for broad-based health programmes. For example, the rapidly urbanizing environment and perhaps even most important of all, climate change, with its resultant effects on health, 6 can only truly be tackled by global cooperation. As with most health issues, the burden falls unequally on and in low- and middle-income economies. Hence, prevention as well as cure will have the greatest impact on these countries.
The WHO, along with academic and other stakeholders from the UK, EU and the rest of the world, has accomplished some success stories, for example, the WHO Framework Convention on Tobacco Control, 7 and the previous UNAIDs summit in 2001 to highlight the effect of HIV. 8 Nevertheless, the forthcoming UN Summit on non-communicable diseases needs to ensure it does not raise and then crush hopes, as the Copenhagen Summit in 2009 did for climate change. Moreover, more holistic financial planning is required to ensure that resources are not moved to non-communicable diseases at the expense of other key areas (e.g. infectious diseases in many settings). 9
In the UK, we can take for granted the strong, fair and accountable healthcare systems that are absent in many countries, increasing health inequalities, and slowing progress in achieving goals slow. The National Health Service (NHS) is also a markedly different financial health system model to that of the USA or India. 10 To remedy this, there are continuing calls for universal healthcare coverage, similar to the NHS, in other places, 11 but it should be remembered that such endeavours will require a considered step-wise approach. Novel technologies and innovations are often cited as a quick alternative, but they can shift the focus from equally challenging issues of the global shortage of healthcare workers and the brain drain from poorer countries. 12
Where does all this talk of utopian global health collaboration leave the bread and butter of the UK economy? Trade in health services, pharmaceuticals and medical devices greatly contributes to both the UK and global economies, and will benefit from the opportunities of a more equitable and ethical global marketplace. Improved access to essential medicines will require a paradigm shift in the current unequal framework of public–private partnerships and intellectual property rights legislation, which does little to benefit the poorest 90% of the world's population. 13
In fact, economic, rather than healthcare, arguments may actually be the strongest driver for addressing global health inequalities: the world is a rapidly changing place, particularly with the relative change in the global economic order (Figure 1). As international healthcare partnerships become more equal, money may actually start flowing in the opposite direction.
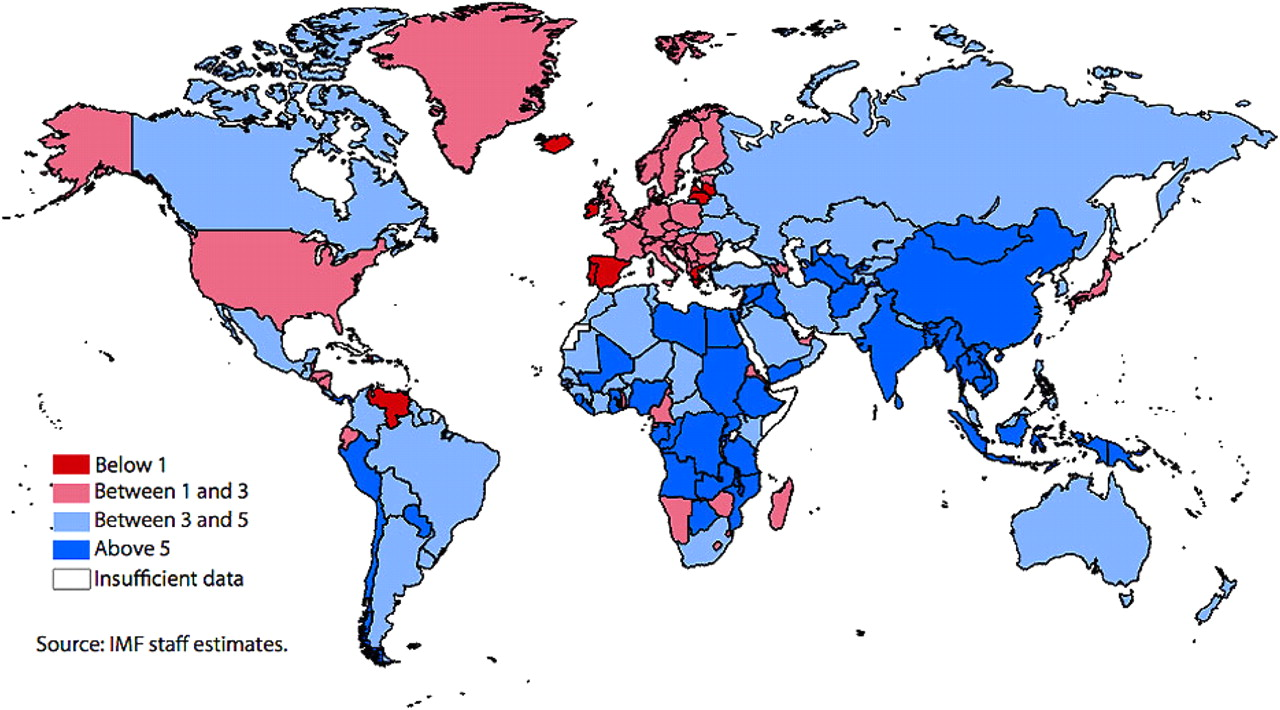
Average real gross domestic product (GDP, %) growth during 2011. IMF = International Monetary Fund. Source: IMF staff estimates (in colour online)
The UK has a strong historical tradition of education and innovation, based on reliable evidence drawn from high quality research, and can pass on the results of its experiences to ensure mistakes are not repeated. Furthermore, UK organizations, such as the Wellcome Trust, have played an important international role in capacity-building to improve infrastructure (and reduce inequalities) in global health education and research. 14 However, in the current financial climate the UK conversely has as much to learn from other countries in global collaborations, for example in how to provide high quality healthcare despite resource constraints, i.e. how to do more for less. 15 In strengthening global research and education, 16 the UK still has a key role to play in helping the world move from a colonial past to a more equal global multicultural future.
DECLARATIONS
Competing interests
NB is funded by a UK Medical Research Council (MRC) Health Services & Health of the Public Fellowship, but the views expressed in this article are his own
Funding
None
Ethical approval
Not applicable
Guarantor
NB
Contributorship
All authors contributed equally
Acknowledgements
None