
Abstract
Recent gynaecological studies show that childbirth, constipation, trauma and surgery cause injuries to autonomic nerves at different anatomical sites in the female pelvis resulting in endometriosis, adenomyosis and fibroids. Re-growth of abnormal nerves causes allodynic symptoms (‘light touch causing pain or discomfort’) some years later including vulvodynia, dyspareunia, dysmenorrhea, irritative bladder and bowel symptoms. Further consequences of autonomic denervation include tissue hypoplasia and hyperplasia, visceral dysfunction, susceptibility to infection, alcohol, tobacco and drugs, as well as pain with sensitization of the central nervous system. The ‘autonomic denervation’ view extrapolates these observations from the female pelvis to the varied anatomy of branches of the cardiac and coeliac plexi to provide primary mechanisms for many forms of Western disease. This account sets out the autonomic denervation view, identifies features of autonomic denervation in extrapelvic organs, and, contrasts it with prior accounts of chronic Western diseases including those of DP Burkitt, PRJ Burch and DP Barker.
Leading global risk factors for mortality and disability are unsafe water, unsafe sex, alcohol use, being underweight as a child, and high blood pressure. 1 Together they account for 25% of deaths worldwide and 20% of disease. 2 Ageing populations in Western countries face increasing risks of chronic diseases from their diets, patterns of physical activity, alcohol and tobacco use. 2 Low and middle income countries face the double burdens of infectious diseases and chronic diseases typical of affluent, Western communities (Table 1). Migrating populations from low-income countries suffer the chronic diseases of host Western populations within a (very) few years. 3,4 It is clear that Western diets and lifestyles play an important role in chronic diseases, yet, we have little insight into their precise mechanisms. Three MRC Professors – DP Burkitt, PRJ Burch, DJP Barker – set out their views of the aetiology of Western diseases in the second half of the 20th century. 5–7 Each set of studies carries empirical observations that overlap with contemporary, WHO risk factors for global disease and disability. This account reviews the ‘autonomic denervation’ view of Western diseases in relation to these prior hypotheses. 8
DP Burkitt's original diseases of Western civilization (BMJ 1973;1:274–8) along with diseases with more recent evidence of autonomic denervation and reinnervation (in italics)
DP Burkitt and the ‘dietary fibre’ hypothesis
DP Burkitt found that Africans eating low calorie, plant-based diets had short intestinal transit times (14 h vs. 40 h), increased stool weights (464 g vs. 110 g per day), and reduced rates of ‘constipation’ compared to Europeans. 5 ‘Constipation’ may mean small or hard stools, delayed passage of stools, or straining during defaecation. 9 It is more prevalent in women than men, children than adults, and, it is particularly common in preterm infants and postmenopausal women. 10,11 Burkitt also viewed squatting as an advantageous method of defaecation (and childbirth) compared to Western methods, though he did not identify the adverse neuropathic consequences. In recent years, KW Heaton found that physical efforts complicated 20–30% of Western bowel movements. One percent of adults opened their bowels less than once each week, and, 0.3% less than once each month. 12 Recent studies confirm that persistent straining during defaecation causes neuropathic pelvic injuries in every organ in the nulliparous female pelvis. 13 Unexplained features of autonomic denervation and reinnervation occur in many extrapelvic diseases on Burkitt's list of Western diseases (Table 1). 5
PR Burch and the ‘stochastic’ hypothesis
PRJ Burch posed the question 6 ‘why does the same disease have the same age of onset in well-defined and widely-separated populations?’ For example, myasthenia gravis, duodenal ulcer and ulcerative colitis have similar, biphasic age distributions in New York, New Zealand and Norway. Each disease also has a similar ‘latent period’ that precedes the onset of clinical manifestations by some years. Before the present enthusiasm for genes and genomics, Burch adopted a genetic explanation though conceded there was ‘no logical necessity for the specific interpretation’. He argued that it was ‘simply not credible that sequential, deterministic biological clocks are distributed among individuals in many different populations so that they always “go off” according to a general stochastic equation’. The limited benefits of recent genomic research tend to reinforce this view.
DJ Barker and the ‘fetal origins hypothesis’
DJP Barker discussed observations in 31 of his papers in Fetal and Infant Origins of Adult Disease. 7 Historical observations of birthweight and infant weight at one year in the first half of the 20th century correlated with the later onset of cardiovascular and metabolic disease in the second half of the 20th century. Typical observations show that low birthweight infants with increased placental weights born in Preston between 1935 and 1943, had higher blood pressures at ages 46–54 than those adults with normal birth and placental weights. Observations of 370 Hertfordshire men, low birthweight and infant weight at 1 year, had an increased incidence of impaired glucose tolerance in later life. In both sets of observations, low birthweight and infant weight at 1 year provided biological markers for disease phenotypes presenting several decades later in the same individuals. Similar risk factors appear in recent WHO reports on the global burdens of disease. 1,2
The ‘autonomic denervation’ view
Autonomic nerves supply our organs through sympathetic and parasympathetic divisions (Figure 1). The three, great autonomic plexi – the cardiac (thorax), coeliac (abdomen) and hypogastric (pelvis) supply extrinsic innervation to their respective viscera (Figures 1 and 2). Intrinsic visceral innervation varies from the complex interactions of Auerbach's, Meissner's and Henle's plexi in small bowel to the subserosal and submucosal plexi in solid organs such as uterus and prostate (Figure 3). Many neurotransmitters contribute to conduction in preganglionic and postganglionic neurons, at varying distances from the end-organ.
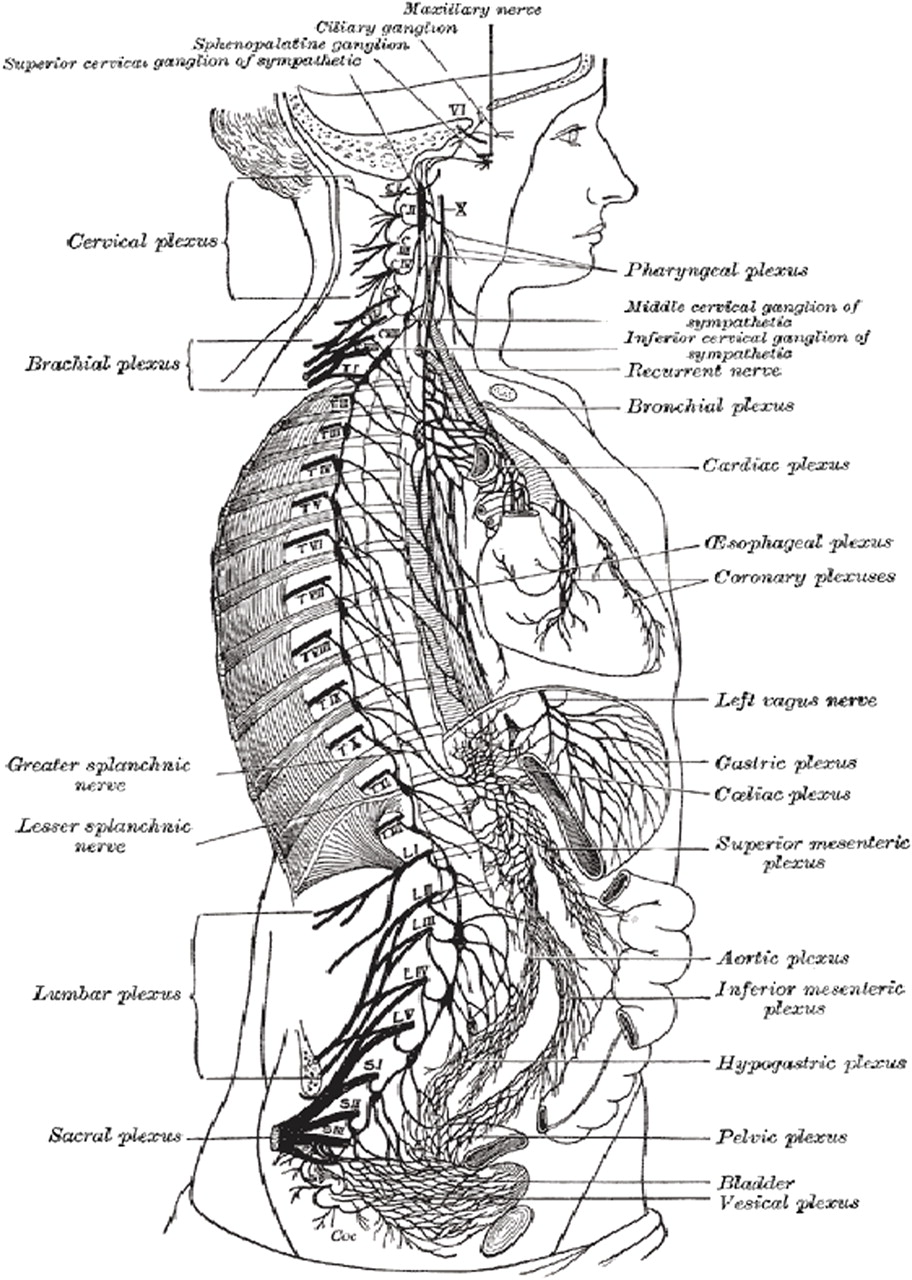
The right sympathetic chain and its connections with the thoracic, abdominal and pelvic plexuses (after Schwalbe, from Gray's Anatomy Fig 838). Note the concentrations of nerves in the cardiac (thorax), coeliac (abdomen) and hypogastric (pelvic) plexi, and the apparent ‘suspension’ of different viscera by branches of the sympathetic chain
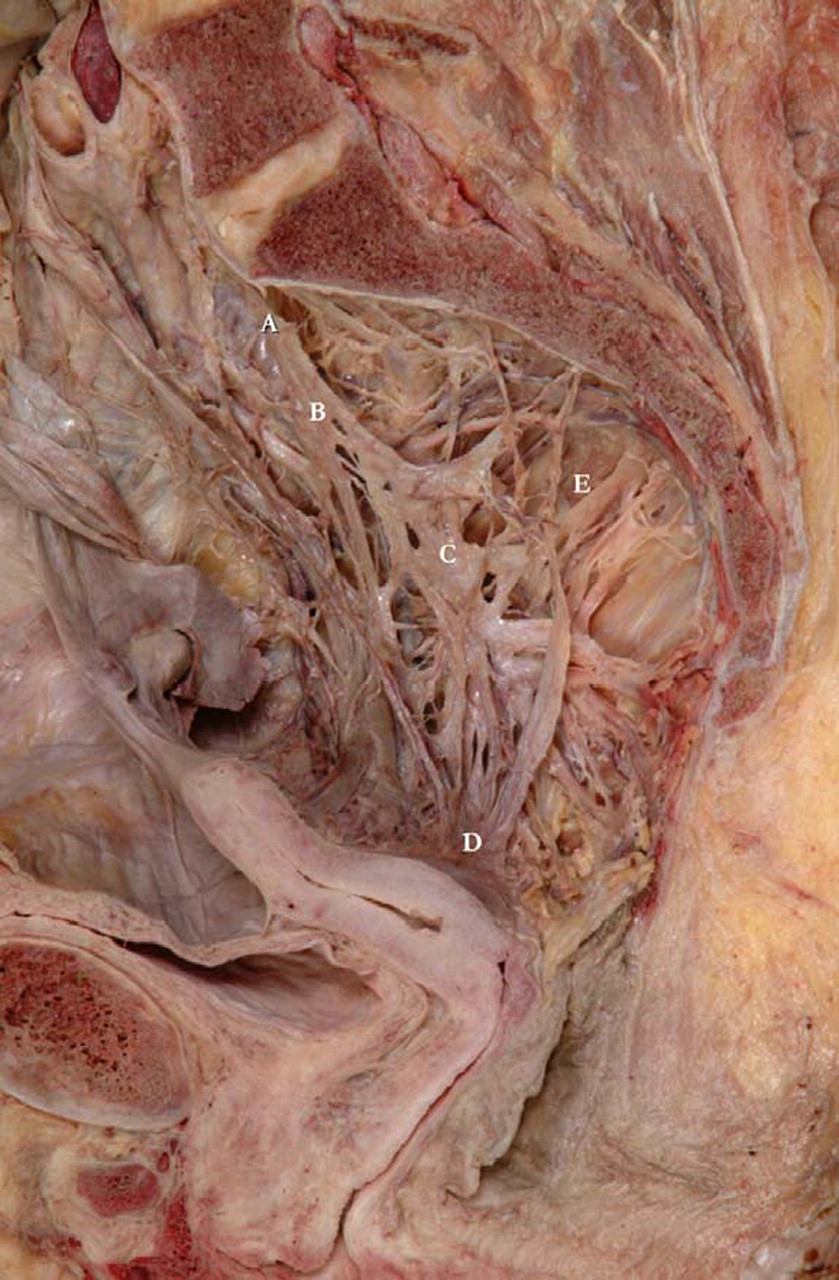
The pelvic plexi dissected in methanol demonstrating the superior hypogastric plexus (a), (b) the hypogastric nerve, (c) the inferior hypogastric plexus, (d) the uterovaginal plexus of Frankenhauser and (e) pelvic parasympathetic nerves from S2–4 (University Department of Anatomy, Bristol)
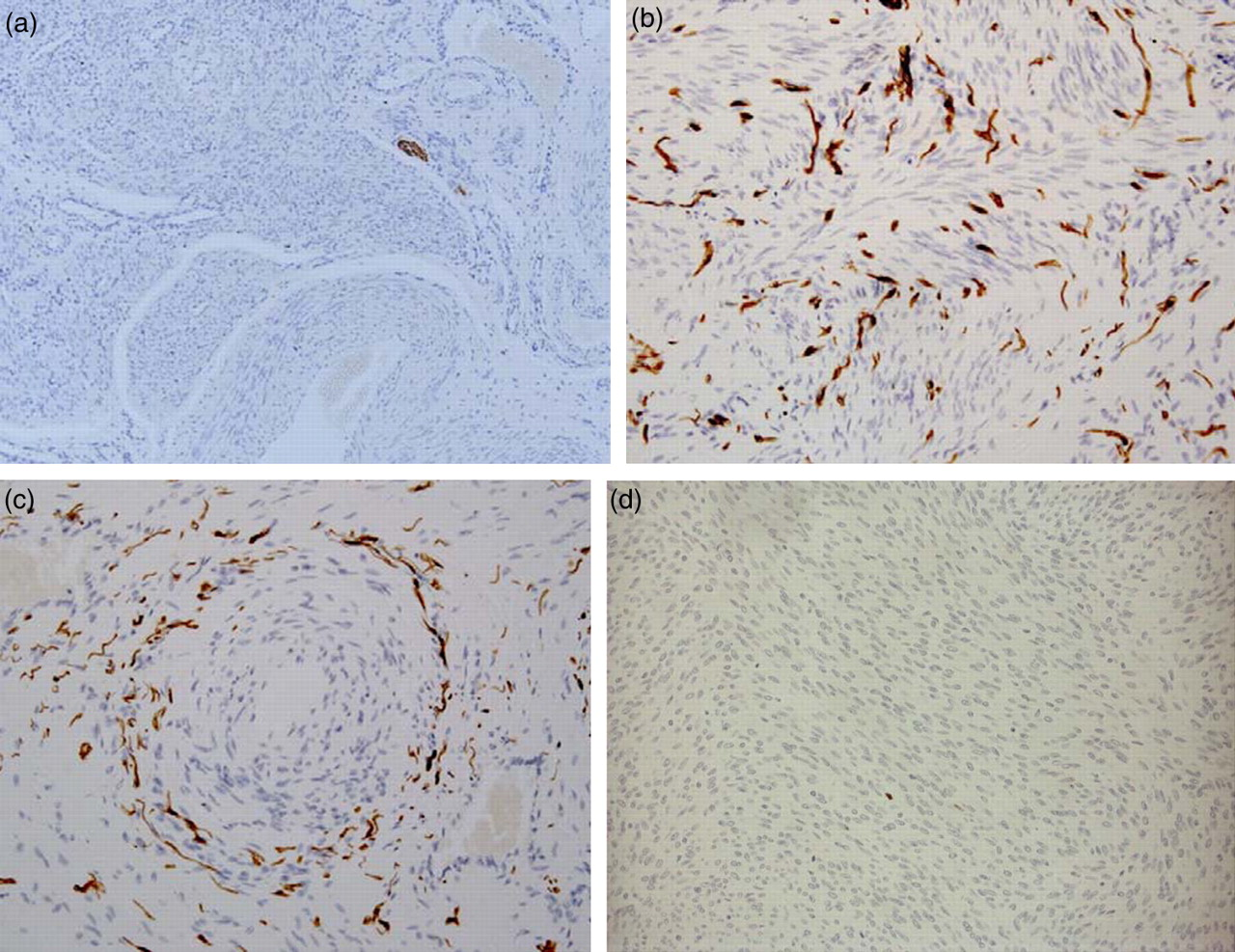
Clinical denervation and reinnervation in the female pelvis produces the three benign pathologies of endometriosis (3b, c), adenomyosis and leiomyomas (3d), as well as many clinical presentations including some forms of vulvodynia, dyspareunia, dysmenorrhea, chronic pelvic pain, irritative bladder and bowel syndromes some years after the primary injury (3b). a. Normal myometrium is sparsely innervated (×100); b. Aberrant reinnervation in the myometrium in chronic pelvic pain with “endometriosis” (×200); c. Aberrant reinnervation. Perivascular nerve fibre proliferation after prolonged constipation (×200); d. Denervation in the myometrium in leiomyoma (×200)
The ‘autonomic denervation’ view proposes that injuries to autonomic nerves at different anatomical sites have diverse and cumulative, biological consequences (Table 2). They result in varied, clinical presentations of Western diseases at different ages. 6 Causes of injuries to autonomic nerves include straining during defaecation, childbirth, trauma and surgery among others. Immunohistochemical studies of injuries to branches of the hypogastric plexus in different gynaecological conditions provide primary evidence of these causes and the diverse consequences (Figures 3a–d, Table 2). 14–16 Extrapolating these observations to branches of the cardiac and coeliac plexi offers explanations for unexplained denervation and reinnervation in thoracic and abdominal organs. 8
Diverse and cumulative consequences of autonomic denervation in the lower genital tract. Analogous consequences may occur at extra-pelvic sites in association with injuries to branches of other autonomic plexi. These injuries may result from persistent straining, trauma and surgery
The hypogastric plexus and gynaecological disease
Large bundles of autonomic nerves converge on the junction of the uterus and vagina with the uterine arteries, and, in the uterosacral ligaments (Figure 2). Both are susceptible to injury during primigravid childbirth. 16 Traumatic injuries to nerve bundles result in haphazard patterns of aberrant reinnervation. 16 Some years later light touch causes pain or discomfort (allodynia) (Figure 3b). Typical ‘allodynic’ symptoms include some forms of chronic pelvic pain, 14,16 dysmenorrhea, 16 vulvodynia, 17 rectal hypersensitivity 18 and irritative bladder symptoms. 19
Consequences of autonomic injury at different sites in the lower genital tract result in different forms of gynaecological pathology. Focal injuries to nerves in the myometrium and endometrium, result in localized hyperplasia including some patterns of leiomyoma and adenomyosis (Figure 3d). 14,15 Injuries to nerves as they enter the organ result in chronic pelvic pain and endometriosis. 16 Such injuries to peripheral autonomic nerves produce persistent, maladaptive plasticity in both peripheral and central nervous systems with recurrent, post-hysterectomy pain occurring in 10–50% of patients at five years. 20 Similar patterns of chronic, disabling pain occurs following amputation (5–10%), mastectomy (5–10%), thoracotomy (10%), coronary bypass surgery (5–10%), inguinal hernia repair (5%), and Caesarean section (5%). 19 Denervation of epithelial surfaces also results in increased rates of opportunist and recurrent infections. 21 The combined effects of complicated childbirth and hysterectomy condemn many women to increasing rates of ‘constipation’ in their later years. 22
The cardiac plexus and cardiovascular disease
Images of extrinsic cardiac innervation are rare and patterns of intrinsic myocardial innervation are complex. Aberrant myocardial reinnervation occurs with ventricular arrhythmias, cardiomyopathies and following myocardial infarction. 23–25 Co-localization of Schwann cells, sympathetic nerves, and nerve axons suggests a relationship between ventricular reinnervation following myocardial injury and subsequent ventricular arrhythmias. 23 Nerve sprouting may contribute to ventricular arrhythmia and sudden cardiac death, where myocardial infarction results in nerve injury that is followed by sympathetic nerve sprouting and aberrant myocardial reinnervation. Histological changes similar to those in uterine vessels with perivascular nerve fiber proliferation around coronary vessels, suggests the possibility that these lesions may contribute to some forms of angina. 26
Hypertension and thrombosis are key determinants of chronic cardiovascular disease. Over-activity of renal sympathetic nerves in and around the wall of the renal artery is important in some forms of systemic hypertension. 27,28 Recent reports demonstrate sustained reductions in blood pressure after catheter-based renal denervation in patients with refractory hypertension. 27,28 There has been little research into the possible thrombogenic effects of denervation in the walls of varying diameters of blood vessel.
The coeliac plexus and abdominal disease
The coeliac plexus is part of the expanded plexus of autonomic nerves behind the stomach extending on to the crura of the diaphragm and along the anterior surface of the aorta. The three, splanchnic nerves connect with all the thoracic ganglia, and supply most of the organs in the abdominal cavity. Both have prolonged anatomical courses to their visceral targets (Figure 1).
Type 1 diabetes mellitus (T1DM) has characteristic epidemiologic features of a Western disease with incidences varying from 0.1/100,000 per year in some Chinese provinces to more than 40/100,000 per year in Finland. 29 Recent studies show evidence of pancreatic denervation in both rats and human. 30,31 Weaning before three months of age is associated with increased rates of constipation resulting in persistent physical efforts by the infant in the supine position that may lead to early, selective loss of sympathetic nerves in the islets of Langerhans. 31 Other patterns of late-onset, organ-specific, ‘autoimmune’ disease (OSAID) including thyroiditis, gastritis, pancreatitis, adrenalitis co-exist in women and demonstrate similar histological features with infiltrates of CD4 and CD8 lymphocytes. Typically OSAIDs co-exist with similar diseases in adjacent organs in first-degree relatives suggesting related aetiology. Autonomic denervation secondary to persistent, physical efforts during defecation or childbirth may cause primary visceral denervation rather than an ‘autoimmune attack’. 22
The mesenteric plexus receives nerves through the coeliac plexus as well as its own direct supply. Nerves originate from the oblique origin of the root of the mesentery to three intrinsic bowel plexi (Auerbach, Meissner and Henle) as far as the splenic flexure. Ascending branches from the hypogastric plexi deliver similar patterns of innervation to the descending colon and rectum. Aberrant reinnervation occurs in some forms of oesophagitis, cholecystitis, chronic pancreatitis, inflammatory bowel disease, appendicitis, benign rectal disease, irritable bowel syndrome and anal fissures. 8 Loss of autonomic nerves to the bowel occurs in Hirschsprungs disease, Crohns disease, ulcerative colitis colonic adenoma and some forms of diverticulosis in association with abnormal forms of visceral motility. 8
Additional sources of morbidity
Persistent increases in intra-abdominal pressure contribute directly to herniae, hemorrhoids and varicose veins though may also contribute, indirectly, to disease at other sites. 5 Contemporary rates of obesity compound their effects. Aberrant reinnervation occurs in many other miscellaneous conditions including allergic rhinitis, 32 intervertebral disc pain, 33 erosive lichen planus, 34 Dupuytrens contracture, 35 anal fissures 36 prostate cancer 37 and pancreatic cancer. 38 Many cancers qualify as Western diseases and autonomic denervation may play a role in their pathogenesis though evidence remains limited at present.
Conclusions
Injuries to complex and varied pathways of autonomic nerves, contribute to different phenotypes of gynaecological disease. Causes of pelvic autonomic injury include straining during defaecation, trauma, surgery and difficult vaginal delivery. Different patterns of straining in different body shapes and sizes may also contribute to autonomic injuries in the thorax and abdomen. Straining during defaecation is one direct mechanism where refined diets may contribute to chronic diseases. Contemporary levels of obesity amplify the direct effects of increased intrathoracic and intra-abdominal pressures contributing further swathes of morbidity. The autonomic denervation view is a direct development of Burkitt's seminal observations, offers answers to Burch's questions, and connects Barker's low birthweight, and underweight infants with chronic diseases in later life. Further studies of the causes and consequences of autonomic injury, will improve our understanding of the aetiology and pathogenesis of the growing global burden of chronic disease.
DECLARATIONS
Competing interests
None declared
Funding
None
Ethical approval
Not applicable
Guarantor
MJQ
Contributorship
MJQ is the sole contributor
Acknowledgements
Alice Roberts, Ross Spackman and Bill Wrigley contributed to the cadaveric studies at the University of Bristol (Figure 2); Gordon Armstrong, Daniel Duplessis, Gurprit Atwal and Deborah Jones contributed to neuro-immunohistochemical studies (Figure 3)