
Abstract

This case highlights an unusual presentation of cerebral tuberculosis (TB) and the associated radiological findings on MRI, including diffusion-weighted imaging.
Case report
A 17-year-old Indian man presented with a two-month history of left-sided headache, morning vomiting, visual disturbance and bilateral papilloedema. On direct questioning the patient noted 6 kg of weight loss in the prior six months. On referral to the acute neurosurgical service MR imaging was carried out. Following the injection of gadolinium the lesions enhanced peripherally on T1-weighted image (T1WI) with multiple smaller enhancing lesions associated with the main lesions (Figure 1a–d). Two well-defined (3.5 cm) low signal lesions were demonstrated on T2-weighted image (T2WI), in the left fronto-parietal and right occipital regions, with marked surrounding oedema (Figure 1e). The diffusion-weighted MR sequence did not demonstrate restricted diffusion (Figure 1f), as would be expected of a liquid abscess. 1 Chest X-ray was normal and laboratory findings were as follows: haemoglobin 12.7 g/dl, white cell count 5.9 × 109/L, C-reactive protein 20 mg/L. There was no laboratory or clinical evidence of an immunocompromised state.
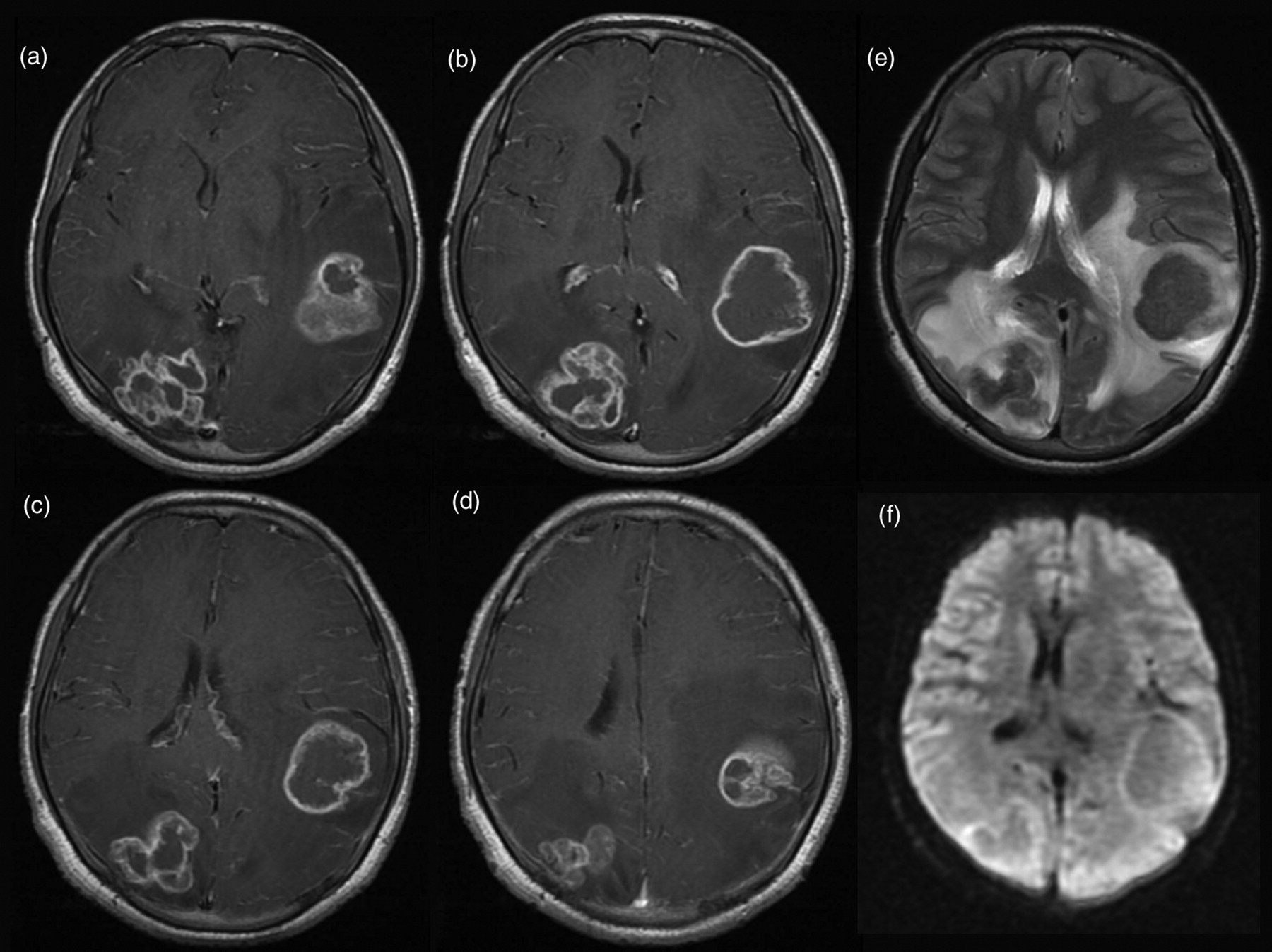
Preoperative MR imaging.
In view of the mass effect caused by the left fronto-parietal lesion and the uncertain diagnosis the patient underwent an emergent image-guided craniotomy and excision of the left-sided lesion. At craniotomy a hard, well-circumscribed lesion was identified with a similar colour to normal white matter. Histology confirmed cerebral tuberculoma, as evidenced by granuloma formation and a single acid-fast bacillus. Subsequent chest CT identified pulmonary TB. The patient commenced anti-tuberculous triple therapy with Rifater, moxifloxacin, pyridoxine and dexamethasone. 2 At three-month follow-up his presenting symptoms and papilloedema had resolved and he was gaining weight. Repeat MR imaging at this point demonstrated complete surgical excision of the parietal lesion and a reduction in the size of the occipital lesion with reduced oedema suggestive of a response to pharmacological therapy (Figure 2).
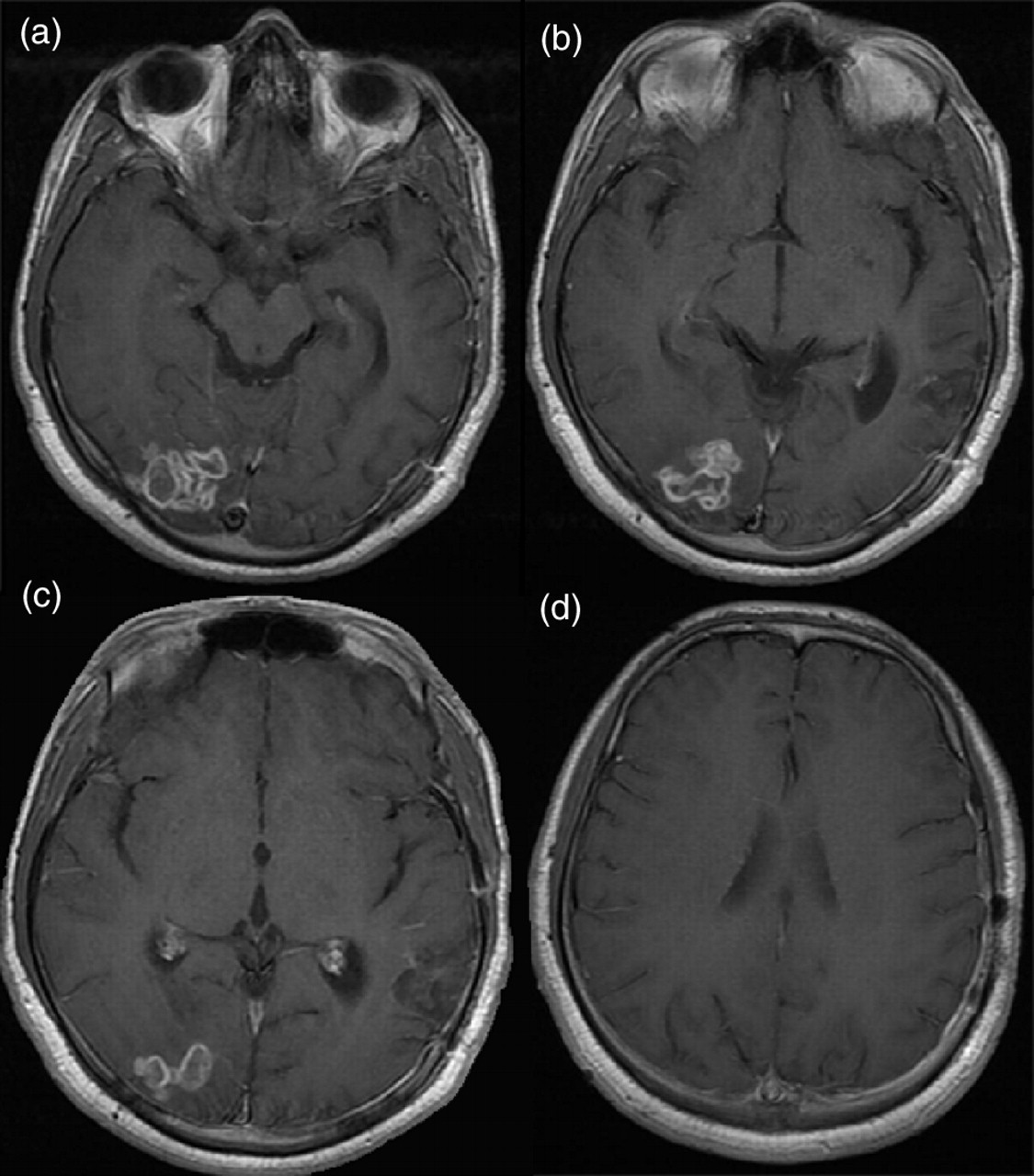
Follow-up MR imaging at three months.
Discussion
The global incidence of TB is increasing, even in the immunocompetent population. 3 Central nervous system TB is most common in those aged below 20 years (60–70% of cases), and coexistent extra-neural TB is only reported in 50% cases, as in this case. 4 Central nervous system TB most commonly takes the form of meningeal disease (leptomeningitis or more rarely pachymeningitis) as well as the parenchymal disease described here (tuberculous granuloma [‘tuberculoma’], tuberculous abscess, focal cerebritis and ‘allergic’ tuberculous encephalopathy) 5 . The most common clinical presentation of a tuberculoma is headache, signs of intracranial hypertension, focal neurological deficit and seizure.
Tuberculous meningitis is characterized radiologically by the triad of basal meningeal enhancement, hydrocephalus and cerebral infarction, though a range of other features are common. 5 Cerebral tuberculomas are most common at the cortico-medullary junction, especially in the frontal and parietal lobes, as they are often the result of haematogenous spread as part of miliary TB. 6 Diffusion-weighted MR is a useful adjunct in abscesses as the central portion of an abscess will demonstrate restricted diffusion however this is not the case in a true tuberculoma. 5
Follow-up imaging following appropriate anti-tuberculous pharmacotherapy allows the response to therapy to be gauged, with the degree of contrast enhancement and surrounding oedema related to the activity within the tuberculoma. 7 A high index of clinical suspicion is required to allow rapid diagnosis of this condition in order to institute rapid treatment and avoid potentially serious neurological sequelae.
DECLARATIONS
Competing interests
None declared
Funding
AH is supported by a joint Medical Research Council/Royal College of Surgeons of England Clinical Research Training Fellowship and a Raymond and Beverly Sackler Fellowship; PJH is supported by the Academy of Medical Sciences/Health Foundation Fellowship
Ethical approval
Written informed consent to publication has been obtained from the patient or next of kin
Guarantor
PJH
Contributorship
AH conducted the research and literature review and wrote the first draft; PJH was responsible for the clinical aspects and overseeing the paper; NMA was responsible for neuroradiology; all authors contributed to the final draft of the paper
Acknowledgements
None
Reviewer
Phillip vanHille