
Abstract

When a stable chronic condition unaccountably changes its nature or symptoms, new pathology should be urgently considered and actively sought.
Background
Superior vena cava obstruction occurs in 10% of patients with right-sided intrathoracic malignancy, the majority of which are related to bronchogenic malignancy. 1 Early symptoms are often mild, non-specific and overlooked. The classical symptoms and signs of dyspnoea, facial swelling, venous distension and plethora are usually late presentations. Here, we describe the case of an elderly woman who demonstrated unusual presenting symptoms in a pre-existing benign condition that eventually led to the diagnosis of superior vena cava obstruction from a lung malignancy.
Case report
A 79-year-old woman, an ‘occasional smoker’, was referred by her general practitioner with a history of increasing headaches and confusion. She described four months of left temporal swellings, very tender to touch with discolouration, and left-sided headaches described as being aching/throbbing, aggravated by standing from a lying position, bending, coughing and straining. The patient recalled suffering an injury to the same region as a child, with subsequent recurrent episodes of headaches and facial swelling very similar to, but less severe than, this current presentation. Previous investigations (30 years ago) identified a left intra-orbital abnormality, thought to be a haemangioma, but it remained unchanged and asymptomatic. She denied other neurological symptoms but did report an unexplained weight loss of approximately 25 kg over a few months.
Her previous medical history included triple coronary artery bypass grafts, type 2 diabetes mellitus, hypertension, myocardial infarction, rheumatoid arthritis and right total hip joint replacement.
On examination, she had an obvious swelling around the left orbit, with some mild proptosis. She had multiple small swellings and discolouration on her left temporal region, which were very tender, but a temporal artery pulse was felt. All other aspects of the physical examination, including chest examination, were unremarkable (Figure 1).

Clinical photograph showing the unusual temporal swelling and discolouration
The initial investigation results were relatively unremarkable, except for a microcytic anaemia (Hb = 8.2 g/dl, MCV = 74 fl), with raised CRP (103 mg/L) and ESR (62 mm/h). The chest X-ray report read: ‘As before, there is coarsening of the bronchovascular markings in keeping with longstanding COPD with an unfolded thoracic aorta and evidence of previous CABG. In addition, there are new findings of ill-defined patchy consolidation since scattered throughout the right lung in all three zones. The differential diagnosis includes atypical infection or post-inflammatory change rather than malignancy although I will advise for a repeat film following treatment if this is clinically indicated to check for resolution. If this has not resolved despite treatment, then an urgent CT scan would be warranted.’ Figure 2 shows the chest X-ray showing ill-defined changes in the right lung field.
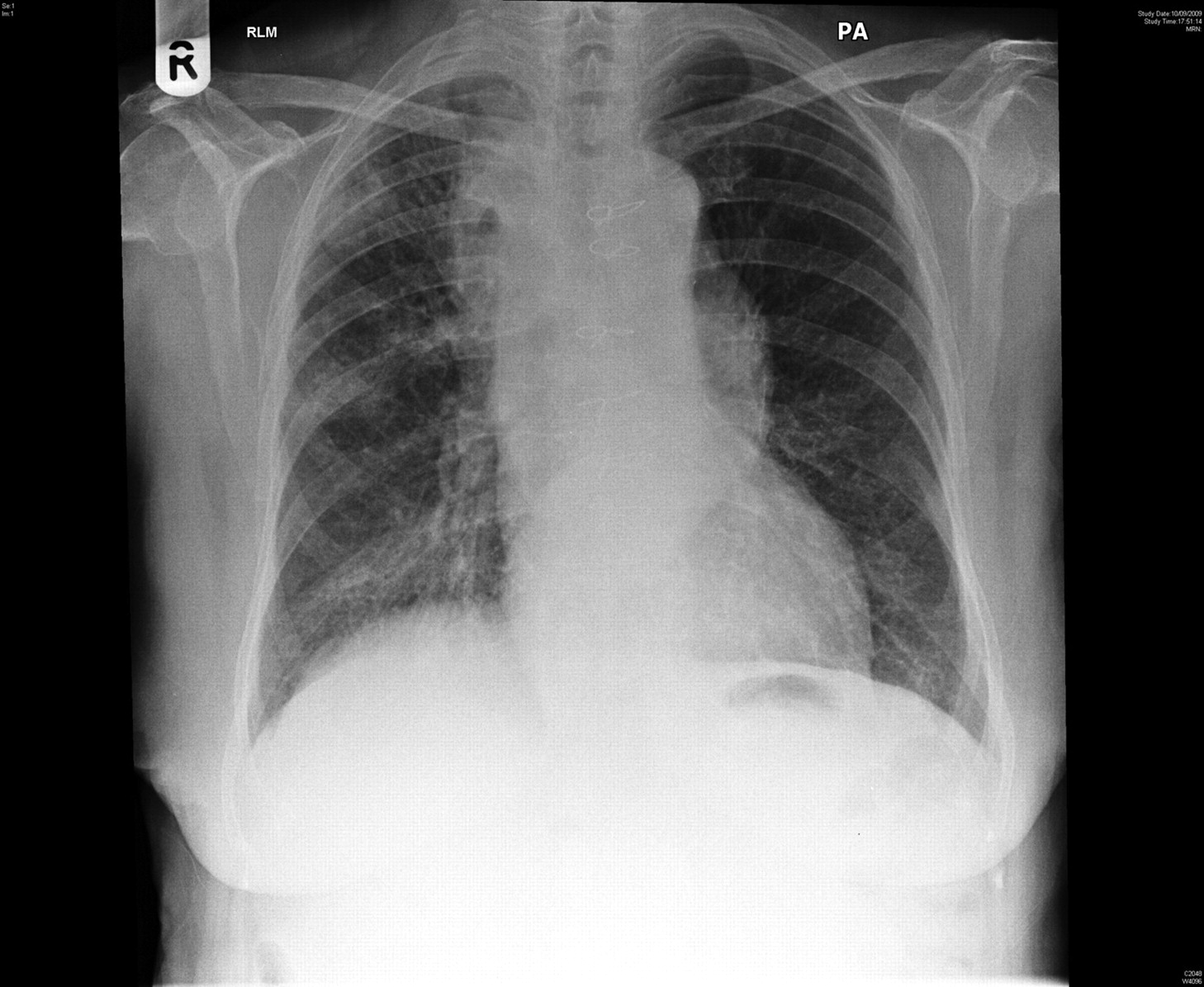
Chest X-ray showing ill-defined changes in the right lung field
Subsequent CT and MR scan of the head revealed the haemangioma in the left orbital region surrounding the optic nerve (Figure 3).
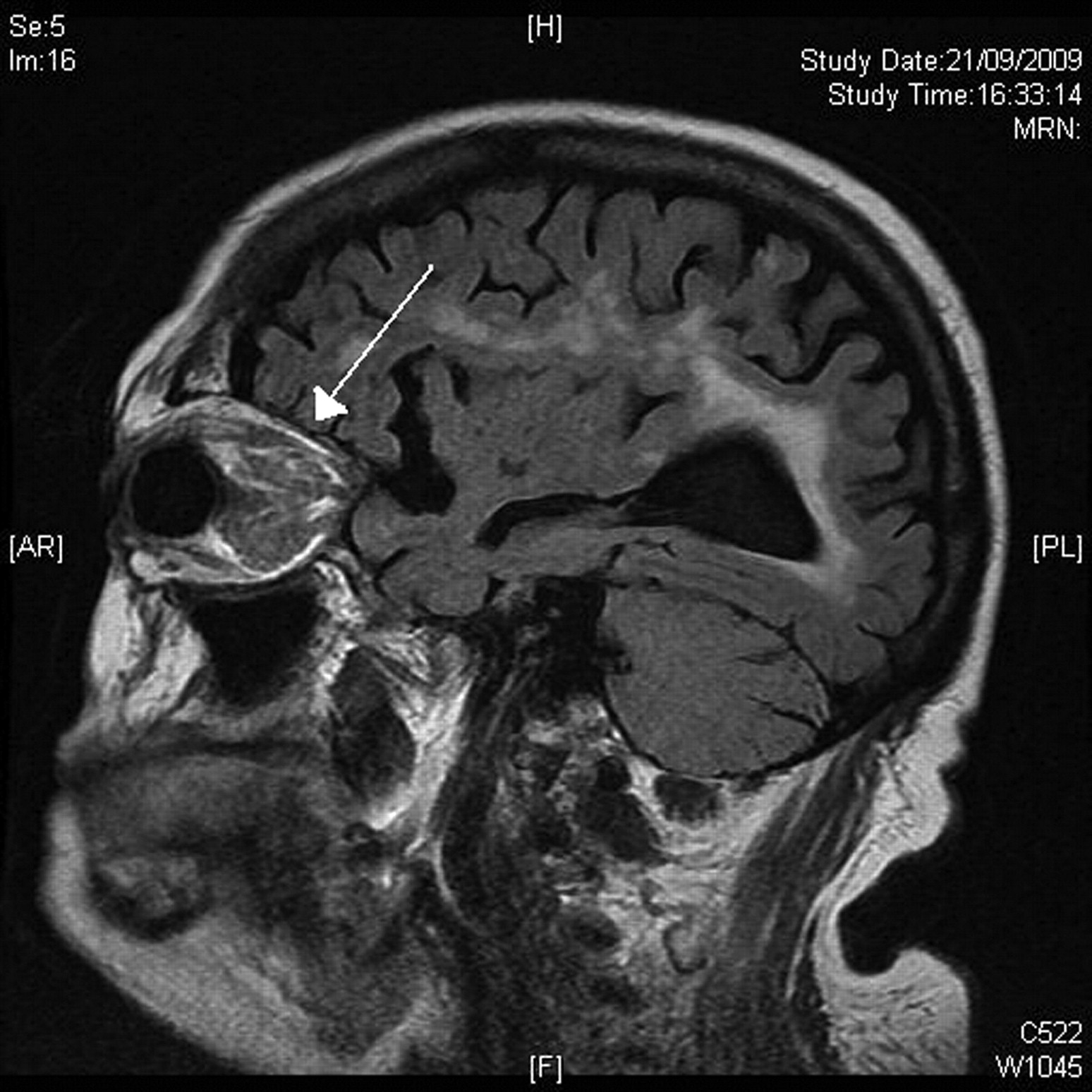
Sagittal MR image showing the retro orbital haemangioma (indicated by white arrow)
Her cranial symptoms were thought to arise from this arterio-venous malformation, but why it should become so abruptly symptomatic was unclear.
Considering her concurrent clinical history of weight loss and anaemia, as well as the recent change in her chronic cranial symptoms and signs, CT scanning was arranged to search for possible underlying pathology. CT (thorax/abdomen/pelvis) revealed a 7 cm right upper lobe bronchogenic carcinoma invading the mediastinum, trachea, right main bronchus and superior vena cava (T4, N1, Mx). Bronchoscopy confirmed a tumour almost completely occluding the right main bronchus, and histology showed high-grade squamous dysplasia and areas of complex architecture, which were suspicious but not diagnostic of malignancy (Figure 4).
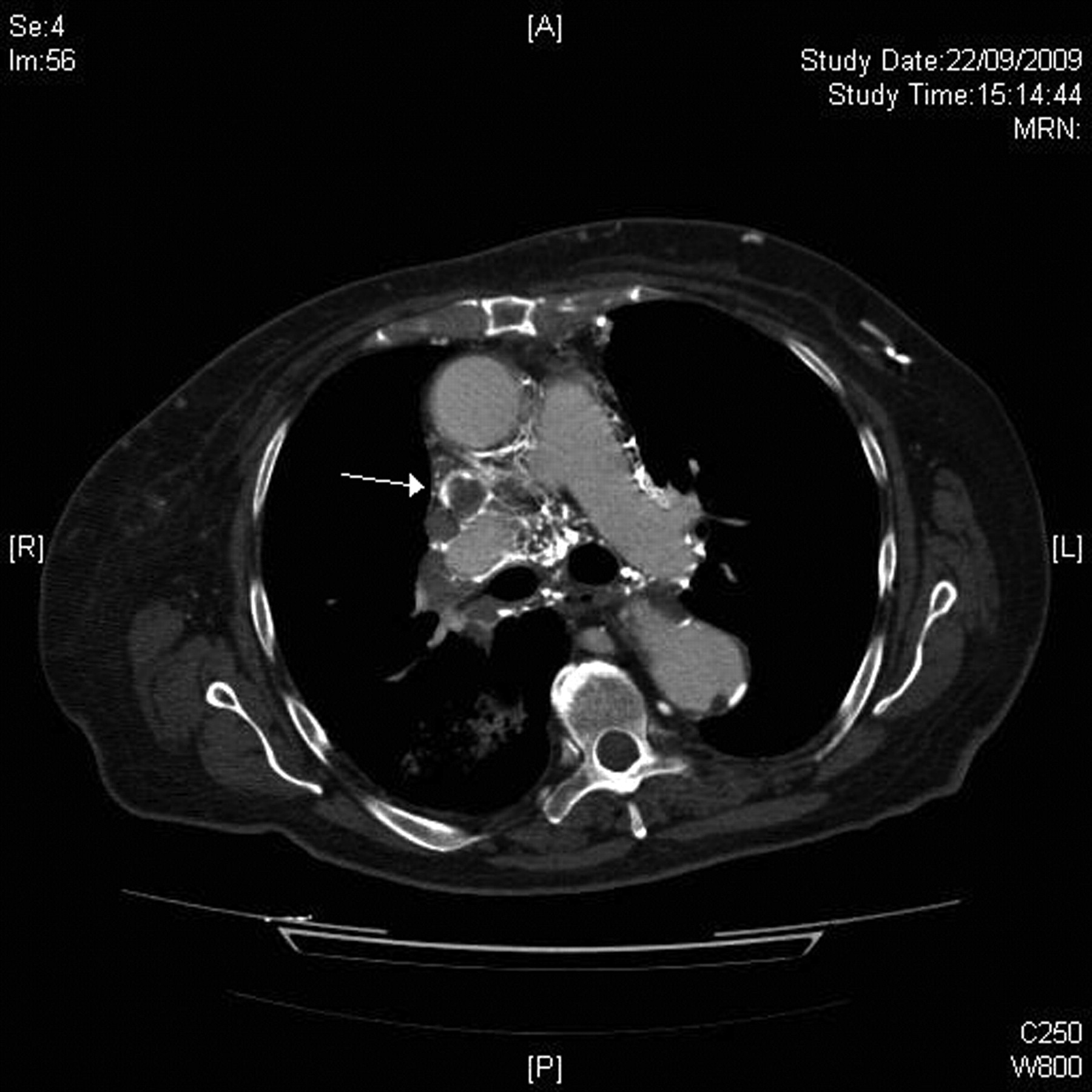
Near-complete SVC obstruction (indicated by white arrow) is seen in this image of the CT thorax
Assuming that this woman's initial presentation of left-sided headaches and swelling associated with an orbital haemangioma was an unusual presentation of superior vena cava obstruction, further specific questioning revealed her to have experienced morning ‘puffiness’ of her face and hands which would spontaneously resolve through the day. She had microcytic anaemia for nearly a year, and subsequent outpatient haematology review a few days before admission had indeed advised investigation for an underlying secondary cause for the anaemia. The multidisciplinary team accepted the diagnosis as likely non-small cell lung carcinoma and had planned to refer without biopsy for palliative radiotherapy. Initial treatment was with dexamethasone 16 mg once daily with some benefit but, unfortunately, she died shortly before she could receive radiotherapy.
Treatment of superior vena cava obstruction
Where superior vena cava obstruction is suspected, and where there are no contraindications, initial urgent treatment is with high dose dexamethasone (16 mg po/i.v. o.d. or 8 mg po/i.v. b.d. – doses never later than 13:00 to avoid sleep disturbance). Steroids help to decrease inflammation and oedema surrounding the tumour, while diuretics are sometimes used to reduce venous return and thereby relieve venous pressures. 2
Subsequent treatment, as a matter of urgency, requires liaison with local surgery and oncology specialists. Choice of treatment depends on stage of disease, prognosis, general state of health and local availability of therapies. Rapid and sustained relief of symptoms can be obtained through endovascular and percutaneous stenting of the superior vena cava. 3 Several studies confirm stent insertion in superior vena cava obstruction provides better results than radiation therapy and recommends them as first-line treatment. 4,5 Decompressive superior vena cava surgical bypass is mostly used in patients with advanced disease with severe cerebral or laryngeal oedema and in those with extensive thrombosis of the superior vena cava. 1 Chemotherapy can be considered in patients with chemosensitive tumours. 3
Discussion
This case demonstrates the often unusual nature of presentation of oncological/palliative care emergencies, of which superior vena cava obstruction is one. Sudden exacerbation of a quiescent intra- or extra-cranial arteriovenous malformation is a novel and unreported manifestation of superior vena cava obstruction. When an underlying chronic condition changes its nature or when symptoms become dramatically more severe, a new pathology may be the cause and needs to be sought. This patient was not known to have a malignant disease and the presentation itself was somewhat obscure. Her initial mild symptoms had been overlooked. Her unexplained dramatic weight loss and anaemia subsequently raised suspicions of an underlying serious or malignant process requiring urgent investigation.
Clinicians need to be aware of the common oncological/palliative care emergencies such as superior vena cava obstruction, malignant spinal cord compression, hypercalcaemia of malignancy, clinically significant neutropenia. If signs or symptoms suggestive of such conditions are evident, or even suspected, appropriate further investigation and management must be instigated as a matter of urgency.
The importance of such diagnoses should not be understated. Even when purely palliative, prompt identification, investigation and management can reduce suffering, extend periods of good quality of life and help patients and their families more than simple survival statistics may show.
DECLARATIONS
Competing interests
None declared
Funding
None
Ethical approval
Written informed consent to publication was obtained from the patient or next of kin
Guarantor
PGW
Contributorship
All authors contributed equally
Acknowledgements
None
Reviewer
Howard Branley