
Abstract
Objectives
Changes in the contractual responsibilities of primary care practitioners and health boards have resulted in a plethora of arrangements relating to out-of-hours healthcare services. Rather than being guaranteed access to a GP (usually either their own or another through a local GP co-operative), patients have a number of alternative routes to services. Our objective was to identify and assess the availability and adequacy of relevant standards, responsibilities and information systems in Scotland to monitor the impact of contractual changes to out-of-hours healthcare services on equity of access.
Design
Cross-sectional study.
Setting
All providers of primary care out-of-hours services in Scotland.
Participants
Not applicable.
Main outcome measures
First, identification and policy review of current standards and performance monitoring systems, data and information, primarily through directly contacting national and local organizations responsible for monitoring out-of-hours care, supplemented by literature searches to highlight specific issues arising from the review; and second, mapping of data items by out-of-hours provider type to identify overlap and significant gaps.
Results
In Scotland, data monitoring systems have not kept pace with changes in the organization of out-of-hours care, so the impact on access to services for different population groups is unknown. There are significant gaps in information collected with respect to workforce, distribution of services, service utilisation and clinical outcomes.
Conclusions
Since 2004 there have been major changes to the way patients access out-of-hours healthcare in the UK. In Scotland, none of the current systems provide information on whether the new services satisfy the key NHS principle of equity of access. There is an urgent need for a comprehensive review of data standards and systems relating to out-of-hours care in order to monitor and evaluate inputs, processes and outcomes of care not least in respect of access and fairness of distribution of resources.
Introduction
Until April 2004, general practitioners (GPs) in the UK were responsible for either directly providing primary healthcare services or for arranging 24-hour cover for their registered patients. The new General Medical Services contract (nGMS) transferred this responsibility to health authorities, allowing GP practices to opt out of the provision of out-of-hours services. 1 As a result, by the end of 2004, 95% of GP practices in Scotland had done so as had most in the rest of the UK. As a result, rather than patients being guaranteed access to a GP (usually either their own or another through a local GP co-operative), they can choose a range of routes into care. The out-of-hours period is defined as 18:30 to 08:00 weekdays and all day at weekends and bank holidays, though in practice in many parts of the country the service starts at 18:00 through local agreements.
The Primary Medical Services (Scotland) Act 2004 placed a duty on NHS boards to provide primary medical services to their resident population. 2 NHS provision for out-of-hours care is the responsibility of the 14 territorial health boards, and two special health boards – namely the Scottish Ambulance Service (SAS) and NHS 24 service which provides 24-hour telephone access to trained nurses. Patients can access services through NHS 24, out-of-hours centres, Accident and Emergency (A&E) departments and the SAS. Figure 1 shows a typical model of out-of-hours care before and after the contract.
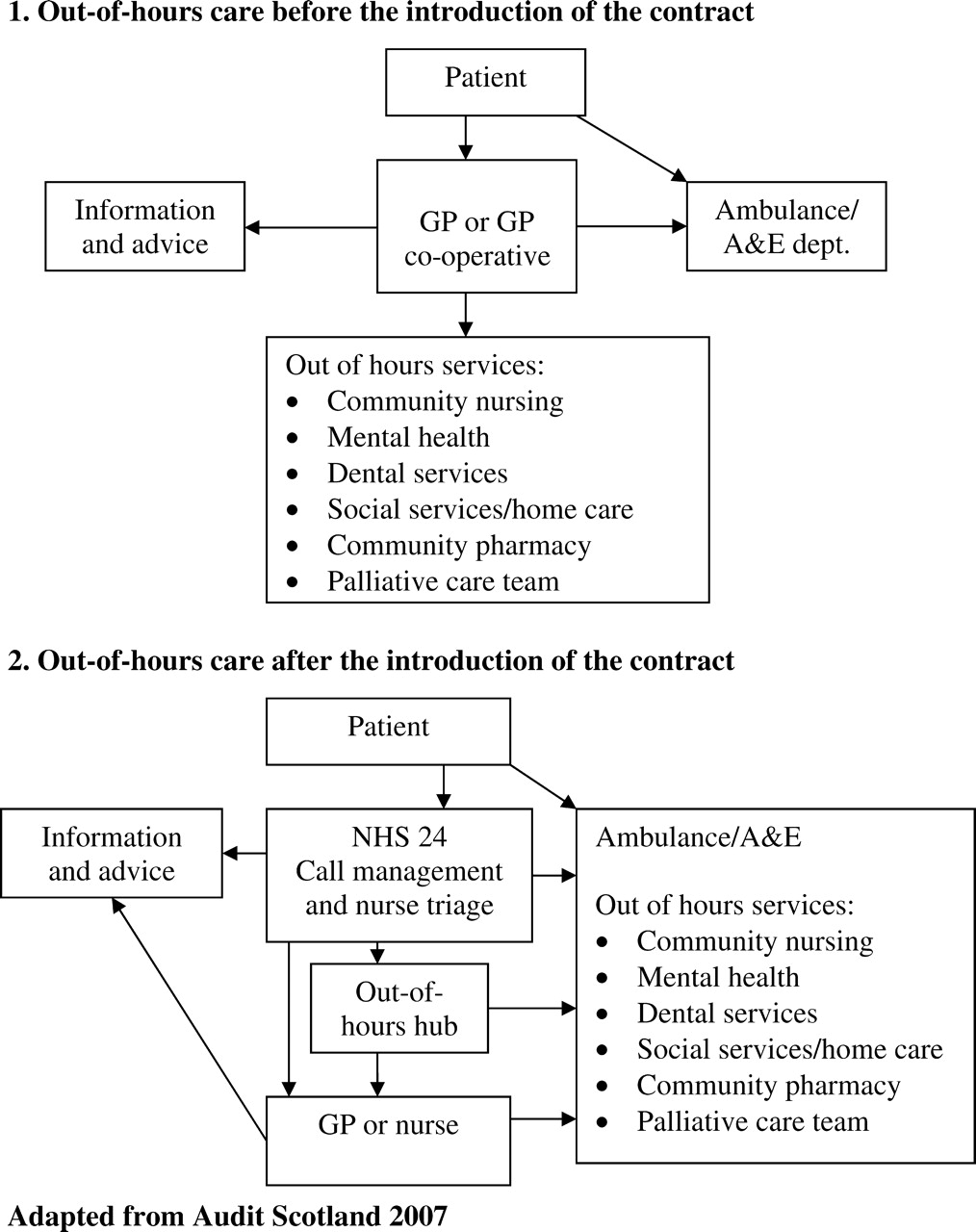
Out-of-hours care in Scotland before and after the nGMS contract
NHS 24 was introduced in 2001, and was intended as supplementary to and not a substitute for GP out-of-hours services. However, the new contract gave health authorities the freedom to provide services through a variety of routes that increasingly moved away from traditional GP-led care to ‘exploit a number of models for delivering out-of-hours care using various providers and professions… Different models of care will be developed in different areas shaped around local needs and circumstances.’ 1
There is public concern about the lack of access to out-of-hours GP cover particularly in remote and rural areas, while high profile media tragedies have raised questions about the effectiveness of NHS 24. 3 The implications for access and quality (use of locum doctors, NHS 24, etc.) may not be monitored through current data systems. In England the Care Quality Commission enquiry into out-of-hours care by the independent healthcare provider Take Care Now highlighted deficiencies in the national monitoring of out-of-hours services. 4 The loss of a standard GP-led model of care and the introduction of a variety of services which may not have the GP as the first point of contact, may create differences in access to out-of-hours healthcare. This is at odds with the central NHS principle of equitable access, an objective that depends on the ability to plan services for the whole population.
Measures of access are vitally important as the time and distance it takes to reach unscheduled services can impact on survival and clinical outcome. 5 For example, faster ambulance response times can improve survival from cardiac arrests, 6 while basic life support and early pre-hospital thrombolysis can reduce mortality. 7,8
A lack of out-of-hours GP services can act as a barrier to access. Findings from a study by Turnbull et al. found that patients from urban areas had higher call rates, while Campbell found those in rural areas often delayed seeking help until their own GP was available. 9,10 In England, Knowles et al. found less use of the telephone service NHS Direct by certain groups within the population; men, older people, those without car or telephone, lower education levels, communication difficulties, and non-home owners in relation to their needs. 11 A study of data from the British General Household Study found higher A&E use by poorer individuals, while NHS Direct use was higher in more affluent populations. 12 Therefore, changes in provision and investment in either service impact on population subgroups differently.
The importance of good data to monitor access to out-of-hours services has been documented. In an evaluation of NHS Direct in England, Lattimer et al. had difficulty obtaining adequate and appropriate data and recommended the need for a minimum common data-set for unscheduled care. In the meantime they called for guidance on how to make the best use of routinely collected data. 13 Similarly, in an assessment of the impact of NHS Direct on demand for out-of-hours care, Munro et al. noted that a lack of complete data limited their study. 14 Heaney evaluated NHS 24 activity and its impact on other unscheduled care services and also noted difficulty monitoring services due to the quality of routine data collected citing inconsistencies in data, its inadequacy for application beyond immediate patient care, and frequent coding changes. 15
Lack of data is echoed in the 2007 Audit Scotland review of the impact of changes on the delivery of out-of-hours services which identified variable practices by health boards with little monitoring of the effect on related services. They recommended making improvements to national performance monitoring and benchmarking, though provided no detailed guidance on data to be collected for this purpose. 16
For the purpose of this review we set out to describe the current standards, performance systems and data in use in out-of-hours care in Scotland and the potential use of these to monitor access.
Methods
For this study, all relevant standards and performance monitoring systems, responsibilities, and data and information systems relating to out-of-hours care were identified, primarily through directly contacting appropriate individuals from national and local organizations and those with a role in a policy group with responsibilities for monitoring out-of-hours care. The list of organizations contacted is detailed in the Appendix. In addition, we searched the literature to highlight specific issues arising from the review.
Further, we identified the data items collected by each type of out-of-hours provider and mapped these to assess areas of overlap and to identify significant gaps. This was in order to assess the extent that data are available to monitor access to care since the introduction of the new contract.
Results
An evaluation of standards and performance systems to monitor access to out-of-hours services in NHS Scotland
Standards
NHS Quality Improvement Scotland (QIS) was established as a Special Health Board in 2003 to improve the quality of healthcare by setting standards and monitoring performance, and by providing support to NHS Scotland on effective clinical practice and service improvements. One way it approaches these objectives is by producing standards of care against which health board performance is monitored. Following the nGMS contract, QIS published standards for ‘The Provision of Safe and Effective Primary Medical Services Out-of-Hours’ in 2004 17 which are a statutory requirement for all providers. 18
Initially health boards self-assessed their performance against the standards which were appraised by QIS; then boards produced action plans to address areas of non-compliance which were subsequently reassessed. Since 2007 health boards have been responsible for compliance with the standards which aim to make services ‘accessible, available and acceptable to patients’. 17,19
There are three core QIS standards for out-of-hours care, each with a number of subordinate statements, underpinned by criteria that must be met to achieve the standard (Table 1). We reviewed the standards to evaluate their capacity to monitor access to care.
NHS Quality Improvement Scotland (QIS) Standards for the Provision of Safe and Effective Primary Medical Services Out-of-Hours
Standard 1 – Accessibility and availability at first point of contact
Health boards are required to undertake an assessment of population needs and patient satisfaction and to ensure population service planning is based on needs. However, the QIS process does not review the data that boards collect to undertake planning. Further, although guidance suggests public health needs assessments should include a variety of population groups such as people from ethnic minorities, migrant workers and travellers and those living in rural areas, 20 QIS reports do not require monitoring of these groups, though in practice some of the boards’ reports do refer to these.
The self-assessment documentation contains little practical guidance about how to meet criteria and as a result health boards’ reports do not refer to the use of data from non-GP out-of-hours providers, i.e. NHS 24, SAS and A&E.
Standard 2 – Safe and effective care
Criteria 2(a)1 and 2 relate to patient involvement in both service development and their own care, but apply only to those patients who are receiving services rather than those who have not accessed care. Criterion 2(a)5 requires that boards have clear lines of accountability to monitor out-of-hours care provision but provides no guidance on how to demonstrate this.
Standard 3 – Audit, monitoring and reporting
Criterion 3(a)4 requires an annual report to be published on performance and services but gives no guidance on content or the inclusion of population data on access with the result that detailed data is not collected.
In summary, the standards fall short of providing a framework for ensuring equity and fairness of access to and provision of services within and between groups.
Performance systems
The Scottish Government manages and monitors health board services through compliance with the HEAT (Health Efficiency Access and Treatment) performance management system which sets targets and measures against which NHS Boards are publicly monitored and evaluated. All 14 territorial boards are assessed against this set of 30 objectives while NHS 24 and SAS have their own targets.
As Table 2 shows, in 2008–2009 data and targets relevant to accessing out-of-hours care are mainly limited to measuring waiting/response times for A&E, SAS and NHS 24. There are no measures of access relating to need, utilization of health services (which depends not only on availability and supply but also affordability, accessibility and acceptability to users), or outcome. Therefore, the priority of data collection appears to be to monitor waiting times rather than equity of access. Further, the lack of connection between the different organization's data-sets means it cannot be assessed the extent to which patients might access more than one service, e.g. by visiting A&E if the complaint was not addressed by NHS 24.
HEAT Targets for 2008-09 relevant to access to out-of-hours care
The ability of data and information systems in use by providers to monitor access
The systems used by main providers to collect data are as follows:
Primary care out-of-hours centres: Each board has a single out-of-hours hub to coordinate services for its area through which it can receive information electronically from NHS 24 for its patients and pass on to the GP. Currently data from out-of-hours primary care centres are not collated nationally. All use either the Adastra and Taycare systems which allow access to the Emergency Care Summary (a shared record enabling all NHS clinicians to access basic health information for an individual). Because systems are linked, data collected by NHS 24 are available for all patients who access via this route and GPs can pass patient information to the hubs, which is then available to NHS 24; NHS 24: Patient information is collected using the Patient Relational Management System. Staff can also access the Knowledge Management System tool which provides clinical information to aid decision-making during a consultation, and the Emergency Care Summary. This information is stored centrally with the Community Health Index (CHI) database and imported by NHS 24 and out-of-hours primary care centres for use in consultations. The CHI population register used in healthcare in Scotland uniquely identifies an individual, but is not yet available from all systems; SAS: This currently operates two data systems for out-of-hours contacts. The ‘Command and Control’ system collects data relating to the daily operation of the service. Each call is allocated an incident number which can be used to link data to the ‘Clinical’ system (and to NHS 24) which records data such as diagnosis and interventions; A&E departments: These use a variety of electronic information systems, and most boards use the nationally procured Emergency Department Information System. Data are collected from all departments through the Information Services Division (ISD) A&E data mart whose purpose is primarily to monitor performance against waiting time targets, with all other data items optional rather than mandatory. The National Clinical Dataset Development Programme produced data standards for A&E ‘core’ data and waiting times which apply to these items. A&E information is also collected by ISD via Hospital Activity Statistics routine data.
Overview of data items and systems in use by providers
There is no central coordination of the development of out-of-hours data systems nor an agreed common data-set of items for each organization. Data collections are largely determined individually. Table 3 provides an extract of some of the key data items collected by each provider and indicates some overlap between them. Meaningful comparisons between providers may not be possible however due to the use of different data standards and accuracy of coding. For example, where more than one organization collects an item, this may be collected/coded differently. Some items in the table are not mutually exclusive, e.g. clinical information items may be separate in some sets, but part of a free text item in another. An example of issues that arise from collecting data differently is a patient who calls an ambulance and is taken to A&E. A review of the key data items collected by each organization from Table 3 indicates that the information collected between the two services does not really enable a full picture to be built up of the patient and their use of the out-of-ours service, impacting on the ability to monitor the overall system.
Key data items collected by out-of-hours providers in Scotland
*ISD(S)1 data (Hospital Activity Statistics)
C = collected, M = mandatory, O = optional
Discussion
Key findings
Despite the standards, targets and data systems, there are no data or measures to facilitate detailed monitoring of access to out-of-hours care, for example distribution of services, staff, patient utilization and clinical outcomes.
With regard to staffing, health boards’ responsibility for planning their out-of-hours services includes producing workforce plans as part of their Local Delivery Plan, but while it was previously possible to use the number of GPs needed for a given population as a basis for population planning prior to the nGMS contract, this is no longer possible given the range of different providers, making it impossible to measure the impact of the changes. As SAS HEAT targets are monitored nationally rather than locally, they provide no direct incentive to ensure equitable geographical distribution. For example the shift of ambulances to urban areas may make response time targets more achievable but at the expense of rural populations. 21 In any case, data collected are not adequate for planning services appropriately according to the needs of the population.
Standards produced by NHS QIS are monitored by health boards through self-assessment and not reported nationally. HEAT performance targets facilitate routine monitoring of data from organizations providing the majority of out-of-hours healthcare but currently enable little beyond assessing waiting and response times. The data items and systems used by providers are not centrally coordinated and differences between them impact on the ability to make comparisons or track patients. Although all major providers collect some useful data, there is only the potential to measure access if they can be combined across agencies. This would require a system of collecting consistent, standardized data, with clear standards of coding. To date we are not aware of any work being undertaken to integrate data-sets and systems. There is also a need for an overall planning framework which includes data on resources, workforce, process and outcome measures for assessing population needs. Without this it is not possible to monitor the effectiveness, efficiency and overall quality and coverage of out-of-hours care. In addition, health boards need clear guidance about their requirements to monitor out-of-hours care.
Implications for policymakers
Changes to out-of-hours services are likely to affect patient groups differentially, potentially leading to significant inequalities, for example geographical inequity for rural populations if services are re-organized around the achievement of performance targets. Monitoring of the whole system is required to include patient use and flows between providers in order to assess whether total provision meets population needs. It is only possible to make comparisons between geographical areas and population groups if the complete system is monitored and measured consistently. Although this study relates to Scotland, the findings are likely to apply across the UK as the new GMS contract is UK wide.
Conclusion
Recent developments have radically changed the way patients access out-of-hours healthcare services in Scotland. The introduction of providers has fragmented provision of services and surveillance and monitoring mechanisms. No single body has responsibility for data collection and information has not kept pace with changes in policy. There is now an urgent need for a comprehensive review of the data standards and systems so as to be able to monitor and evaluate inputs, processes and outcomes with respect to access, fairness and equity.
A benefit of the NHS is the ability to plan services for whole geographical populations and to ensure equitable access. Despite changes in responsibilities, this objective remains central. It is therefore incumbent on health boards, NHS Scotland and the Scottish Government to ensure that mechanisms are in place to collect adequate data and use these to monitor access to out-of-hours care, and take action where access is insufficient. Our findings indicate that none of the current monitoring mechanisms and data collections provide information on whether the new services satisfy the key NHS principle of equity of access.
In conclusion, it is impossible to adequately assess the impact of these changes on the quality of care provided to the population as the data and information required to do so is either insufficient, fragmented between the various organizations providing out-of-hours care, or simply not collected. It is not possible to measure differences in access to or quality of care for different subgroups using out-of-hours services in Scotland.
DECLARATIONS
Competing interests
None declared
Funding
None
Ethical approval
Not applicable
Guarantor
SG
Contributorship
SH and SG collected and analysed the data, and contributed to the analysis; SG drafted the first manuscript; SH and AP reviewed the article and contributed to re-writing
Acknowledgements
This article is based on a comprehensive report about the monitoring and surveillance of access to out-of-hours healthcare produced by the Centre for International Public Health Policy, University of Edinburgh. We highlight the main conclusions and their significance for future policy. Arrangements described in this article were as at the time of compilation (end 2008)
Reviewer
Brian McKinstry