
Abstract

Introduction
We describe a 5-month-old female Caucasian infant who presented with corneal perforation and crystalline lens extrusion secondary to Pseudomonas aeruginosa endophthalmitis and was later diagnosed with cystic fibrosis (CF). To our knowledge, this is the first report of CF presenting with P. aeruginosa endophthalmitis.
DECLARATIONS
None declared
None
Not applicable
DSH
Both authors contributed equally
Case report
A female infant was born by spontaneous vaginal delivery at 33 weeks gestation, with Apgar scores of 9 at 1 minute and 10 at 5 minutes, 10 days after rupture of membranes. Her birth weight was on 50th centile for gestation. Maternal high vaginal swab grew Chlamydia trachomatis. She was admitted to the neonatal intensive care unit and commenced on prophylactic intravenous benzylpenicillin (50 mg/kg twice daily) and gentamicin (5 mg/kg once daily), but did not require respiratory support. On day 9 of life she developed respiratory distress requiring intubation and ventilation for 5 days and subsequent nasal CPAP for a further 4 days. She developed bilateral conjunctival discharge and a conjunctival scrape was positive for Chlamydia trachomatis. She was treated with intravenous amphotericin 1 mg/kg once daily plus enteral erythromycin 62.5 mg twice daily and was given one dose of pulmonary surfactant. A chest X-ray revealed an interstitial pneumonia, but all cultures including bronchoalveolar lavage were negative. She made a full recovery and was discharged home on day 27 of life. Repeat conjunctival swabs were persistently negative for Chlamydia trachomatis and her eye discharge resolved.
She represented at 5 months of age, 3 months corrected gestational age, to the A&E Department with poor feeding and lethargy and was admitted for treatment of presumed sepsis. She was found to be failing to thrive, with a weight below the 0.4th centile. There were no focal signs of sepsis except erythema and oedema of the eyelids with a mucopurulent conjunctival discharge. As the left eye was being gently cleaned a crystalline lens slipped out (Figure 1). Ophthalmic examination confirmed left corneal perforation and extrusion of the crystalline lens (Figure 2). A conjunctival swab from the left eye grew Pseudomonas aeruginosa, sensitive to cefotaxime, ceftazidime, tobramycin and gentamicin. She was treated with 21 days of intravenous cefotaxime 50 mg/kg 6-hourly and gentamicin 7 mg/kg once daily plus hourly topical ciprofloxacin eye drops. Urine cultures also grew P. aeruginosa. CSF and blood cultures were sterile and laryngeal aspirates did not grow any significant organisms. Unfortunately, despite aggressive antibiotic treatment, the disruption to the intraocular structures was so severe that the eye required enucleation.

Extruded crystalline lens from left eye
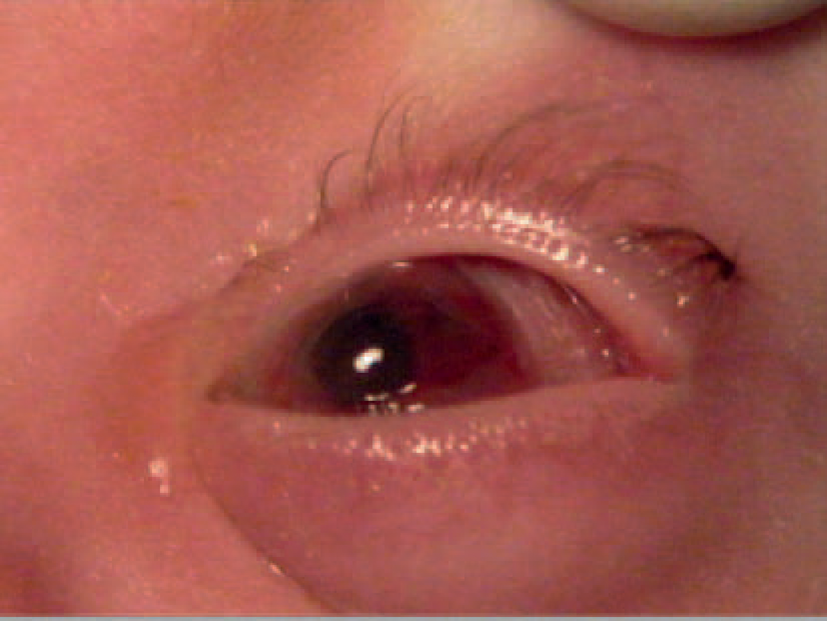
Left eye with large corneal perforation plugged with vitreous fluid
A stool sample was sent for faecal elastase estimation as part of investigation of her failure to thrive. Faecal elastase was found to be <15 mcg/L (reference range 200-600 mcg/L) indicating severe pancreatic insufficiency. DNA was tested for known CF mutations and she was found to be homozygous for delta F508. Immunoglobulin levels were measured during her admission and did not reveal any indication of immunodeficiency (IgG 8.5 g/L, normal range 2-11.2 g/L; IgA 2.15 g/L, normal range 0.08-0.90 g/L; IgM 3.49 g/L, normal range 0.1-0.8 g/L with no abnormal bands on electrophoresis). An HIV test was negative.
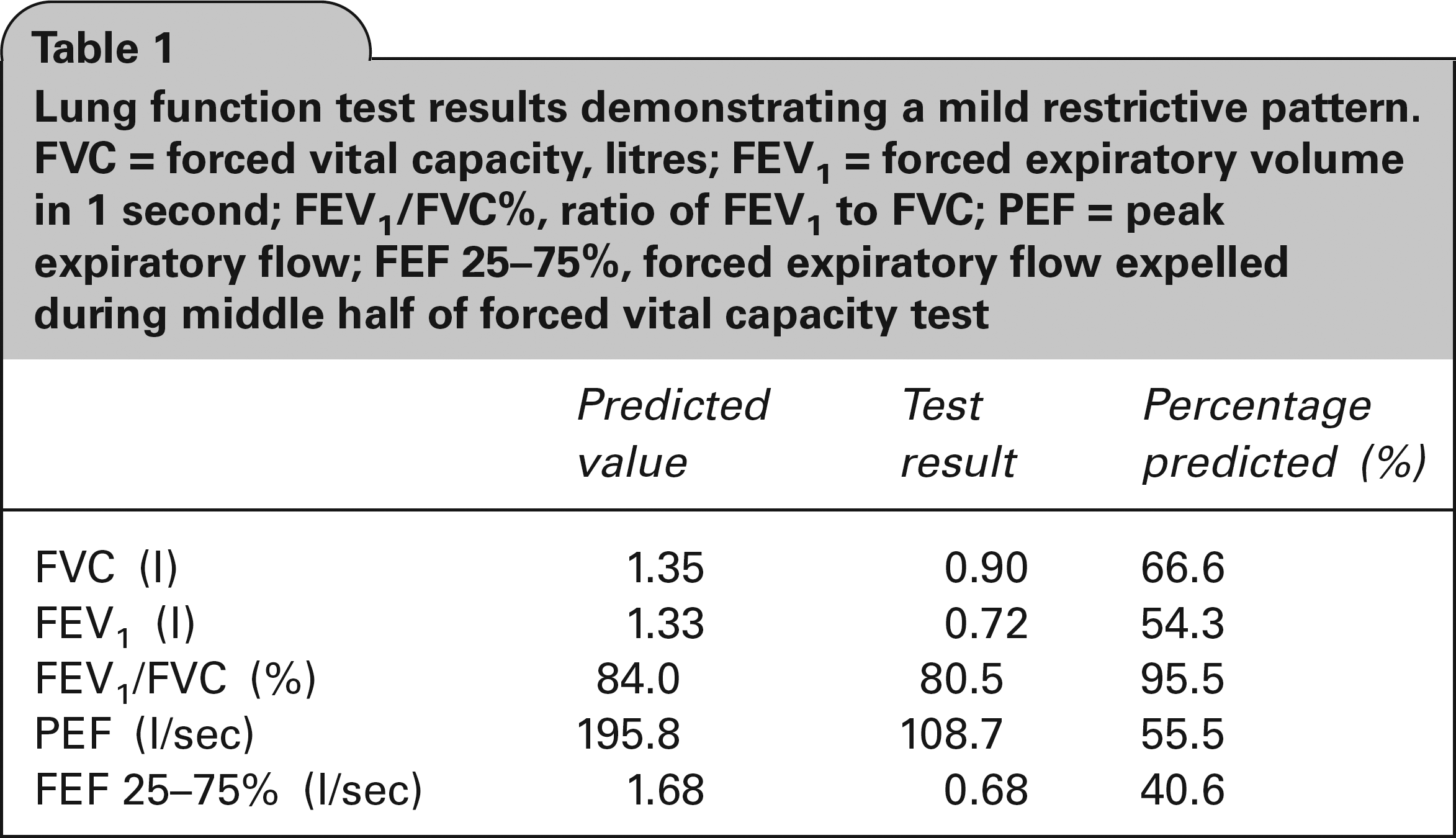
Two months later a cough swab came back positive for P. aeruginosa and she was started on regular home nebulized Colomycin. Since then her cough swabs have been persistently negative for P. aeruginosa and pseudomonal antibodies are not elevated. With a CF regimen of treatment, including pancreatic enzyme supplements, vitamin E, multivitamins and prophylactic flucloxacillin, she has remained well, thriving along the 9th centile for weight and 25th centile for height. Her lung function tests show a mild restrictive pattern (Table 1). She has mild reactive airways disease, responsive to inhaled salbutamol, and chest X-rays show enlargement of the right hilum. She has since been fitted with a prosthetic left eye.
Lung function test results demonstrating a mild restrictive pattern. FVC = forced vital capacity, litres; FEV1 = forced expiratory volume in 1 second; FEV1/FVC%, ratio of FEV1 to FVC; PEF = peak expiratory flow; FEF 25-75%, forced expiratory flow expelled during middle half of forced vital capacity test
Discussion
It has been well-documented that mutations in the cystic fibrosis transmembrane regulator (CFTR), a plasma membrane protein involved in chloride ion secretion, 1 cause a reduced ability to clear thick pulmonary secretions as a result of excessive salt and water absorption from airway lumens. 2 In CF, a mutation in the CFTR gene results in dysfunctional or absent CFTR protein in the lung epithelium. 3 There have been many theories linking CFTR mutations to P. aeruginosa lung infections. One such theory is that defective chloride ion transport results in increased sodium chloride content and subsequently thickened pulmonary secretions, which harbour bacteria such as P. aeruginosa, which cannot be cleared from the airways by cilia. 4 Another theory is that the increased sodium chloride content in airway secretions interferes with antimicrobial factors. 5 However, there is an increasing wealth of evidence to suggest that the CFTR protein itself is directly responsible for immunity towards P. aeruginosa in healthy individuals.6–9 Lung epithelial cells forming the membranous surface to the airway lumens express CFTR proteins. 10 These cells bind to, and internalize, P. aeruginosa. 11 Pier et al. demonstrated ingestion of P. aeruginosa by airway epithelial cells was higher in cells expressing wild-type CFTR than in cells lacking wild-type CFTR. 11 Evidence suggests that it is the CFTR itself that is the ligand for P. aeruginosa allowing ingestion of the pathogen into the cell, with a binding point for P. aeruginosa on the first extracellular loop of the CFTR protein.11,12 Once P. aeruginosa has entered the cell, a host innate immune response ensues 6 and a chain of cellular events ultimately leads to cellular desquamation, followed by apoptosis of the infected cells, which are then thought to be engulfed by phagocytes and destroyed. 13
Cells expressing defective CFTR proteins in CF are unable to effectively eliminate P. aeruginosa, resulting in increased bacterial loads and subsequent infection. 6 Kowalski et al. 6 took human lung cells from a patient with CF homozygous for delta F508 and demonstrated fluorescently stained P. aeruginosa did not enter the cells. The cells were then retrovirally infected with wild-type CFTR or mutated CFTR; the cells expressing wild-type CFTR then ingested P. aeruginosa, while those with mutated CFTR did not. Different CFTR mutations result in varying levels of susceptibility to P. aeruginosa.14,15 Ultimately the patient is rendered susceptible to chronic pseudomonal infection.16,17
Bacterial endogenous endophthalmitis results from haematogenous spread of bacteria from distant sources of infection to the highly vascularised retina and choroid, and then to the vitreous body. 18 It is considered a medical emergency as vision is often lost. Symptoms of endophthalmitis include eyelid swelling and erythema, injected conjunctiva and sclera, purulent discharge, visual disturbance and reduced or absent red reflex. Individuals at risk of developing endogenous endophthalmitis usually have a predisposing chronic condition such as diabetes mellitus. 18 Usual organisms are Staphylococcus aureus and Streptococcus pneumoniae, 19 although secondary seeding by gram negative organisms such as P. aeruginosa is well-documented. 20 Common sources for endophthalmitis include meningitis, endocarditis, urinary tract infection and wound infection.20,21 Lens extrusion is a serious complication of a perforated cornea and suggests disruption of the intraocular contents.
There have been eight previously reported cases of patients with CF developing P. aeruginosa endogenous endophthalmitis.22–25 All described patients had P. aeruginosa colonization in the lung. Four of these patients required enucleation of the globe and one died of sepsis four weeks after developing visual symptoms. All had been treated with a combination of intravenous and intravitreal or subconjunctival antibiotics, combinations of which included ceftazidime, tobramycin and vancomycin, plus pans-vitrectomy to drain purulent fluid from the eye. Of these eight previously reported cases, six of the patients had undergone bilateral lung transplant and were receiving post-transplant immunosuppressive therapy. One of the other patients had been treated with a course of antibiotics and oral prednisolone, for exacerbation of CF with deteriorating lung function immediately prior to developing endophthalmitis. Immunosuppression was implicated in the translocation of P. aeruginosa from the lung in those seven patients.22,24 Our patient had neither been on immunosuppressive chemotherapy nor had she received a course of prednisolone or other anti-inflammatory drugs. A literature review published in 2000 found that 25% of patients with P. aeruginosa endogenous endophthalmitis, both with and without CF, were neonates. 26 We postulate that our patient's immature immune system was implicated in the pathophysiology of this disease process.
Seeding from the lungs was thought to be the cause of P. aeruginosa endogenous endophthalmitis in all eight previously reported cases in CF, as all had P. aeruginosa colonization of the lung. Our patient had negative bronchoalveolar lavage for P. aeruginosa, but positive P. aeruginosa urine cultures, suggesting the source of endophthalmitis was a urinary tract infection rather than lung colonization. A mechanism similar to the pulmonary CFTR-mediated pseudomonal ingestion and cell desquamation model, has been described in clearing uropathic Escherichia coli from infected mouse bladders. 27 There is some evidence that CFTR may be present in toad bladders, 28 but more research is required to investigate whether it is also present in human bladder cells.
Although CF has been known to present with xerophthalmia secondary to vitamin A deficiency,29–31 there are no previously documented cases in the literature of CF presenting with pseudomonal endophthalmitis.
P. aeruginosa endophthalmitis is a devastating ocular disease with high morbidity. P. aeruginosa is an especially virulent organism that may result in an accelerated presentation with rapid loss of vision. 23 There is some controversy as to the most appropriate initial management. Some schools of thought believe that ocular inflammation in endophthalmitis increases the permeability of the ocular-vascular barrier, improving antibiotic penetration 32 and, therefore, intravenous antibiotics are the treatment of choice. Other centres recommend early enucleation in unilateral disease to reduce the risk of the emergence of multidrug-resistant strains of P. aeruginosa with long-term antibiotic therapy. 22 This debate highlights the destructive nature of the disease and the necessity for prompt treatment to limit loss of vision. Our case report illustrates the importance of prompt investigation and treatment of ocular complaints both in children with failure to thrive and patients known to have CF, even if they are not known to be immunosuppressed.
Footnotes
Acknowledgements
The authors would like to thank: Charlotte Daman-Willems, Consultant Paediatrician; Anu Shankar, Consultant Paediatrician; and Wagih Aclimandos, Consultant Ophthalmologist, all from University Hospital Lewisham, for their helpful comments on the manuscript