
Abstract

The idea of thyroid replacement therapy
At a meeting of the Clinical Society of London in November 1883, Felix Semon drew attention to Kocher's presentation at the German Surgical Society the previous April, and proposed that myxoedema, cachexia strumipriva and cretinism were all due to the same cause, namely, absence or degeneration of the thyroid. 1 At the time, Semon was a 34-year-old assistant physician for Diseases of the Throat at St Thomas's Hospital, London (he would later be knighted as the doyen of British laryngology). According to Rolleston2 and Medvei 3 his remarks ‘excited ridicule’. There is no suggestion of this in the British Medical Journal's detailed transcription of the proceedings, 1 nor in the exceedingly brief original written minutes of the meeting (an extended account must have been written up at some later point for the BMJ). Ridicule may not, of course, have been minuted. Semon in his autobiography 4 says only that his ‘extremely bold assertion was received with polite scepticism’, though he writes of antagonism towards him in his early career. Nonetheless, his very astute idea of the commonality of these conditions caught on, one senior member at the meeting suggesting that British surgeons be canvassed for their experience of thyroidectomy. The following month the Society set up a committee, which included Semon, to investigate the whole matter. He had already advised Ord to write to Kocher, as mentioned in Part 2 of this paper. Indeed, Semon's role in the unfolding thyroid story deserves much better recognition.
The Society's survey was a remarkable project, enlisting Europe-wide – including Russian – surgical evidence. One hundred and fifteen surgeons were contacted, including two in Australia. Sixty-nine replies were received, 64 of which were usable though to a variable extent. The Committee's very detailed findings and influential conclusions were published five years later, in 1888, as a supplement volume to the Society's Transactions. 5 The report fully endorsed Semon's view, drawing particularly on animal work carried out by Victor Horsley, one of the committee's members. Horsley had separately reported the effects of total thyroidectomy on monkeys, 6 concluding that myxoedema was almost certainly due to loss of thyroid function and not to ‘chronic asphyxia’, as the Clinical Society's report summarized Kocher's explanation. He also observed initial tetanic manifestations postoperatively, no doubt due to unwitting removal or operative ischaemia of the parathyroid glands, whose separate identity and function were still unrecognized. The report's section on treatment, however, had very little to say, surprisingly making no mention of the possibility of any kind of thyroid replacement therapy despite acknowledging that, four years earlier, Moritz Schiff in Geneva had reported some success in transplanting canine thyroid in thyroidectomised dogs. 7 Kocher, too, had by then tried thyroid transplantation in one of his patients and would continue experimenting with this till the end of his life. 8, 9
Horsley went on to advocate a trial of grafting, specifically sheep's, thyroid to treat myxoedema and cretinism. 10 In June 1890, Bettencourt and Serrano of Lisbon did the experiment, inserting half of a sheep's thyroid subcutaneously into the inframammary region on each side of one of their patients. 11, 12 They found that the graft worked immediately, before it could have vascularized, and concluded that its effect was likely to have been due to simple absorption of juice from the grafted gland, a conclusion of extraordinary importance. They had observed a rise in temperature within 24 hours – not associated with any features suggesting a postoperative febrile reaction – and, over the course of the one month's follow-up, the patient's bloating and weight had decreased, bodily movement and speech had improved, sweating had resumed and there was an almost complete resolution of a preoperative anaemia. These findings, and others describing the benefits, albeit transient, of intravenous injection of thyroid extract in thyroidectomised dogs,13,14 added to the growing recognition of the thyroid's endocrine function (although the word ‘endocrine’ was not used until 1904 3 ).
In Britain, at a meeting of the Northumberland and Durham Medical Society on 12 February 1891, George Murray, 3 years qualified, having taken advice from Horsley, who had been one of his undergraduate teachers, 15 presented his idea to treat a case of myxoedema with an extract of sheep's thyroid given subcutaneously.16 He, too, Medvei tells us, 3 was ridiculed. While the typed minutes of the meeting contain no trace of ridicule; indeed, to the contrary, what could be interpreted as cautious support, Medvei has sourced a reliable account of one senior member of the Society saying: ‘It would be just as sensible to treat a case of locomotor ataxia with an emulsion of spinal cord’. The medical college at Newcastle refused to help.
The likely reason for this dismissive outburst lay at the feet of that medical colossus, Charles Édouard Brown-Séquard, the French neurologist and physiologist. A kind of scientific Ulysses, he had held university chairs in Richmond, Virginia and in Harvard, Paris, Geneva and Paris again.2 He declined the chair of physiology in Glasgow because of the weather! The story goes that he once refused a colossal fee of £10,000 to see a wealthy American patient in Italy because he did not think he was the best person to advise and, besides, private practice interfered with research!2,17 In 1889, two years before Murray's address, Brown-Séquard, aged 72, published a paper on the likely rejuvenating effects on man of injections of animal testicular extracts 18 and then presented a paper to the Society of Biology in Paris on the positive effects upon himself of subcutaneous injections of liquid extracts of dog or guinea pig testicles. 19 His promotion of such ‘organotherapy’, as it came to be called, brought him and his ideas into disrepute, for it spawned every sort of charlatanism and provoked much suspicion among ‘respectable’ practitioners. While Brown-Séquard's research was of the highest order – he had, for example, proven that the adrenals were essential to life – the sensational nature of these later experiments blinded many to the general principle of replacement therapy that was trying to shine through.
George Murray and sheep's thyroid
Undeterred, Murray obtained fresh sheep's thyroid from a slaughterhouse and described carefully his method of preparing and administering the extract. Beginning on 13 April 1891, he injected a 46-year-old woman with most of the characteristic features of myxoedema, with 1.5 mL of thyroid extract subcutaneously, twice weekly (one thyroid lobe's worth). 20 After three months his patient was dramatically better, even though (for reasons he did not explain) her treatment had been discontinuous, just 2.5 thyroid glands' – five lobes' – worth of injections having been given. This led Murray to consider that injections every 2–3 weeks would suffice to maintain improvement. Horsley urged him to publish ‘at once’, 15 probably because he was aware that others were on the verge of doing the same experiment. Indeed, the 10 October 1891 issue of the BMJ containing Murray's report also contains a brief report by Fenwick on the diuretic effect of a hypodermic injection of thyroid extract in a case of myxoedema, but Fenwick considered that the primary pathology lay in the kidneys. 21
Although the BMJ gave no special placement to Murray's initial paper, a follow-up report published the following August, which included three other treated cases, occupied pride of place on page 1, under proceedings of the 60th annual meeting of the British Medical Association (BMA) held the previous month. 22 It included photographs before and after treatment and a temperature chart showing an increase in temperature within days of starting treatment. The particular importance of this second paper lies in the fact that cases 3 and 4, while also showing marked improvement, died suddenly from ‘cardiac failure’ (probably myocardial infarction). Murray writes: ‘[these deaths] show that patients with weak or degenerated hearts may die suddenly after the improvement has taken place, from cardiac failure after exertion to which they have for long been unaccustomed’. This was a telling early alert for the need for caution. Other cases were presented at that BMA meeting, including two who failed to respond to thyroid injections. 23 Horsley, who was at the meeting, expressed the hope that cases of non-response would be recorded and that ‘these might be as fully published as the successful cases’, an early plea against publication bias! Years later, Murray learned that the lack of success in these two cases had been because thymus, not thyroid, had been supplied by the butcher! 24
The Portuguese contribution
But Murray, contrary to general understanding, was not the first to try subcutaneous injections of thyroid extract in myxoedema. A Portuguese researcher had already done so.
Bettencourt and Serrano's thyroid graft experiment in the summer of 1890, mentioned above, was initially the subject of a very short communication. 11 Murray had been aware of this and referred to their results in detail in his first BMJ paper. Indeed, he spoke about them when he originally presented his plan of treatment in February, 1891, and it seems very likely they had informed his thinking. But what neither he nor Horsley appear to have been aware of was Bettencourt and Serrano's full report. This was initially presented at a meeting of L'Association Française pour L'Avancement des Sciences in Limoges in August 1890 and subsequently published the following year. 12 In it, they intimated their intention to try hypodermic injections of thyroid juice in another myxoedematous patient under their care. And on 15 November, 1890, three months before Murray presented his identical plan to the Northumberland and Durham Medical Society, and almost a year before his first paper in the BMJ, Antonio-Maria Bettencourt-Rodrigues reported beneficial effects from these thyroid injections at a meeting of the Lisbon Society of Medical Sciences. 25
Previously sharing in the widely held belief in Murray's priority, the author is indebted for this information to Clark Sawin whose paper has set the record straight. 26 Bettencourt's important results appear to have been published only as a note in the Lisbon Society's proceedings, so it is perhaps not surprising that they have been overshadowed by Murray's more accessible papers in the BMJ.
Oral thyroid replacement therapy
Soon after Murray's 1892 paper, there were reports from others of success with whole
sheep thyroid or thyroid extract taken orally. It has a disgusting taste, so attempts
were made to disguise this in a sandwich or lightly fried with anchovy paste on toast or
taken with current jelly. How reminiscent of the Chinese, centuries earlier – steeping
the gland in wine or taking it in jujubes sounds better! One early report is worth
quoting in extenso because of the modernity of its language, the
appreciation of the importance of controlled conditions, and the finding of a direct
correlation between whole thyroid dose and pulse and temperature rise. Hector Mackenzie,
a London physician, referring to Murray's injection method, pointed out its
disadvantages:
27
First, it requires the most scrupulous care in the preparation of the
extract, the demand for which is never likely to be so great as to enable it to
be supplied when manufactured under the ideal conditions at less than an almost
prohibitive price, and few medical men have the time to devote to its
preparation themselves. Secondly, the application of the remedy sometimes
produces alarming immediate symptoms, such as loss of consciousness and tonic
spasm; and remoter effects, such as indurated swellings and abscesses at the
seat of injection, have followed the use of even the most carefully prepared
extract. When it is remembered that these injections have to be personally
administered for the remainder of the patient's life by the medical attendant,
these risks, however slight in regard to a single application they may appear,
become immensely magnified when a long series has to be taken into
account.
After these reports, Murray changed to oral administration, although he preferred to use an extract whose potency he considered would be more constant, as he was by then preparing it from a pool of sheep's thyroids. Nearly 30 years later, in a retrospective commentary on his first treated case, he calculated that over the 28 years of her treatment till her death, age 74, his patient had consumed around 5 litres of thyroid extract – initially by injection then orally – derived from some 870 sheep. 24 In this paper, he also mentions that, back in 1891, he had sought her consent to treatment: ‘The experimental nature of the treatment was explained, and the patient, realizing the otherwise hopeless outlook, promptly consented to its trial’.
Following Murray's first paper, reviews of larger numbers of treated patients were
remarkably quickly assembled, notably by Cecil Beadles and Byrom Bramwell, and the
principles of treatment, to which we still adhere, were equally quickly
established.
28,
29
There was clearly no shortage of cases of myxoedema, underlining how astonishing
it is that the condition should have escaped identification as a discrete and
homogeneous pathological entity for so long. As the Clinical Society of London's report
put it: An advanced case of myxoedema, age 73, before treatment in 1893. Note the
swollen face, eyelids and lower lip, the almost bald scalp and the rough skin.
Three months after the commencement of treatment the myxoedematous swelling had
almost disappeared and the whole scalp was covered with dark hair, half an inch
in length (from Bramwell 1895) Sporadic cretinism in a 4-year-old girl, before (left) and 2 months after
starting treatment with thyroid extract. Note the myxoedematous swelling of the
whole body has almost entirely disappeared with treatment, the tongue is no
longer protruberant, the expression is much brighter and the child is taller.
The photographs have been reproduced exactly to scale so that the relative
increase in height and diminution in girth before and after treatment are
reliably shown (from Bramwell 1895)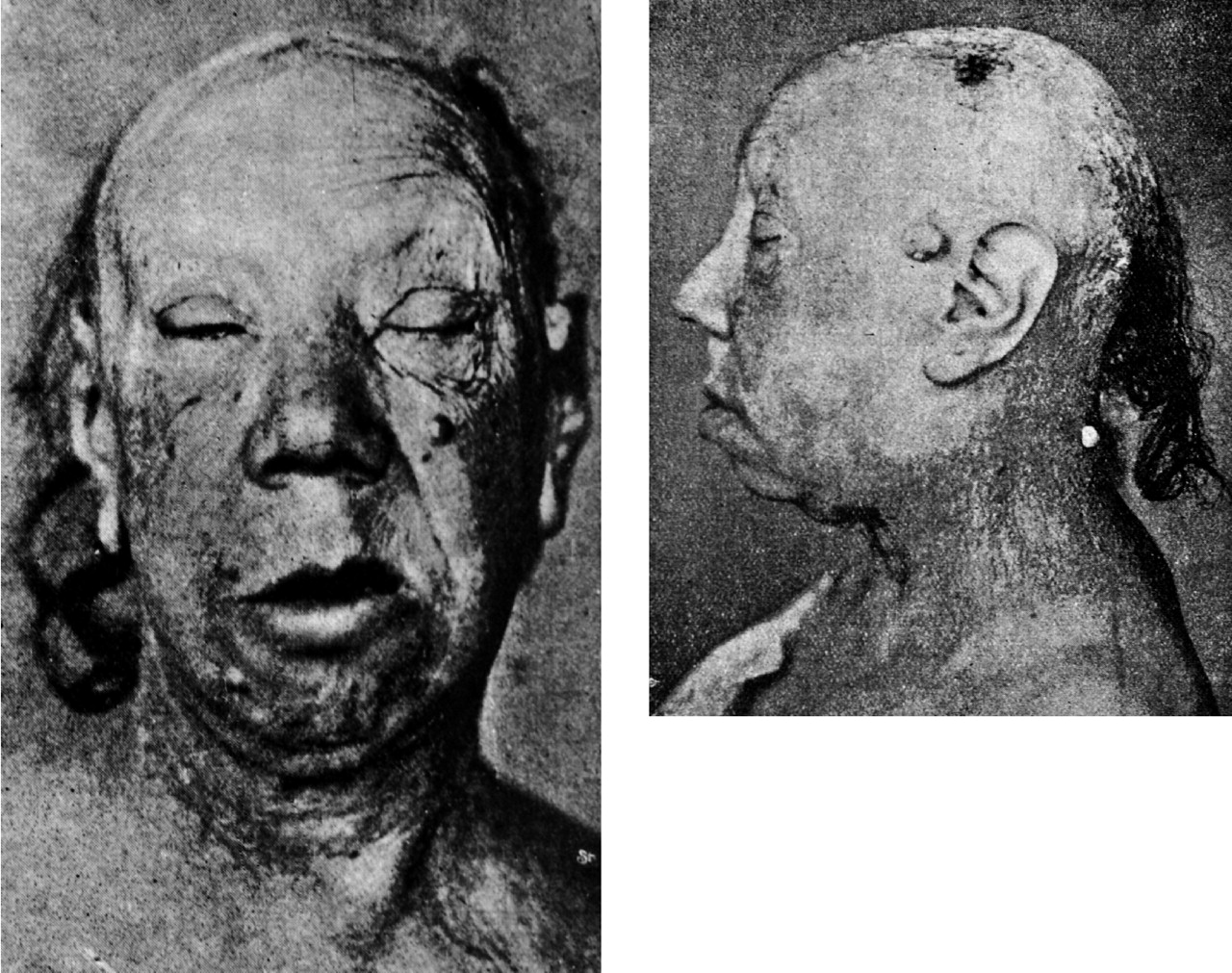

Bramwell advised that treatment should start with a small dose and, if necessary, be gradually and carefully increased; that too large a dose may be dangerous in the elderly and in patients with heart or arterial disease; and that treatment must be life-long, although he presciently commented that ‘… future observation may show that in some cases …the function of the thyroid gland may be temporarily arrested’. He emphasized that early diagnosis was of great importance in cretinism.
The advent of thyroxine and modern times
Thyroxine was isolated in 1915 by Kendall 30 (actually, on Christmas Day, 1914), its chemical structure determined in 1926 by Harington, 31 and it was synthesized by Harington and Barger in 1927. 32 However, it took a long time before it was synthesized on a commercial basis. At first, 3 tons of pigs' thyroids were needed to isolate just 33 grams of pure thyroxine. Even when thyroxine became commercially available from Glaxo in 1949, tablets of desiccated thyroid extract remained the principle source of treatment for many years.
Tri-iodothyronine (T3) was then identified, isolated and synthesized in 1952/53 by Gross and Pitt-Rivers, 33, 34 but, until relatively recently, used only in the management of myxoedema coma. This life-threatening complication of untreated hypothyroidism is now rarely encountered, but T3 has been advocated for use alongside thyroxine in the routine management of myxoedema. This is, however, controversial, as is the optimum dose of thyroxine and its place in so-called ‘subclinical’ or ‘compensated’ hypothyroidism.
One wonders what Murray and Bettencourt and their colleagues would have made of these nuances in treatment which have arisen since it became possible to assay serum thyroid-stimulating hormone levels in 1965 and with ever-increasing sensitivity since then. In Murray's day – he died in 1939 – the diagnosis of thyroid deficiency was made on purely clinical grounds and very mild cases will have been missed. All these developments since those days merit a more detailed account than lies within the scope of this series of papers.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
I would like to acknowledge the indispensable and tireless help of Estela Dukan, library
assistant at the Royal College of Physicians of Edinburgh, and Valerie McClure,
assistant librarian at the Royal College of Physicians and Surgeons of Glasgow. I am
grateful to Mira Gogova, archivist/conservator at the Royal Society of Medicine,
forarranging access to the 1883 manuscript minute books of the Clinical Society of
London. I am similarly grateful to Jackie Dunn, liaison assistant at the Robinson
Library, Newcastle University, for supplying a copy of the minutes of the meeting of the
Northumberland and Durham Medical Society on 12 February 1891. I very much appreciate
the advice given on the Chinese contribution by Vivienne Lo, senior lecturer, and Penny
Barrett, specialist translator and honorary research associate, at the Wellcome Trust
Centre for the History of Medicine. Gesa Walker kindly translated German texts and
Janice Webster was a great help with the French material. I warmly thank them both. I am
grateful to Iain Milne, librarian of the Royal College of Physicians of Edinburgh, who
photographed the illustrative material. Finally, I would like to thank Ulrich Tröhler
for hisTröhler for his helpfully detailed critique.This is the third part of an article
previously published in the James Lind Library (