
Abstract

Vitamin A deficiency is increasing. Early identification of high-risk patients and rapid treatment can prevent potentially fatal and blinding complications.
Case report
A 49-year-old woman presented to the eye casualty with a 3-day history of painful blurred vision in the left eye. At presentation the visual 6/9 in the right eye and acuity was 5/60 in the left eye. She was noted to have a corneal ulcer in the left eye. Corneal scrapes were taken for culture sensitivity and the patient was treated with topical antibiotics as per local protocol. Culture from the scrape revealed Haemophilus influenza and the ulcer responded well to treatment. As the patient came for frequent follow-up for the left eye, the vision in the right eye deteriorated progressively and within two months the vision in that eye was 1/60. The worsening of vision was attributed to dry eye and the patient was referred to the cornea team for follow-up in the cornea clinic.
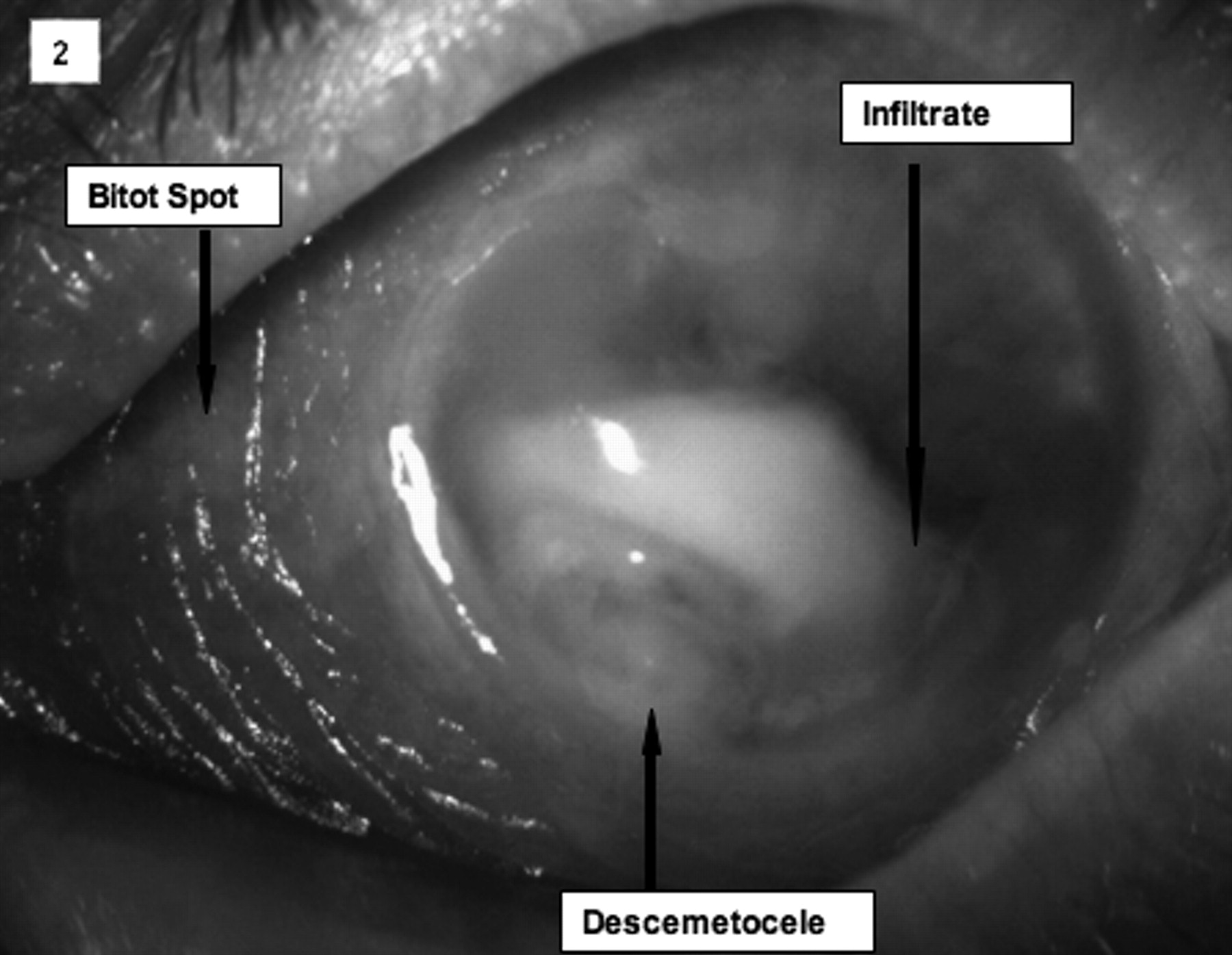
Two weeks later the patient presented to the eye casualty again, now with severe painful visual loss in both eyes. She had bilateral Bitot spots (superficial build up of keratin on the conjunctiva), severe keratinisation of her conjunctiva, bilateral severe corneal ulcers with perforation of the cornea and a descemetocele in the left eye (herniation of an inner corneal layer due to deep corneal ulceration which had eroded the overlying cornea stroma) ( Right eye shows a ‘ground-glass’ appearance, nasal Bitot's spot (foamy grey/white patch), a hazy cornea and an inferior infiltrate Left eye with a large Bitot's spot, inferior corneal thinning, infiltrate and an inferior desmetocele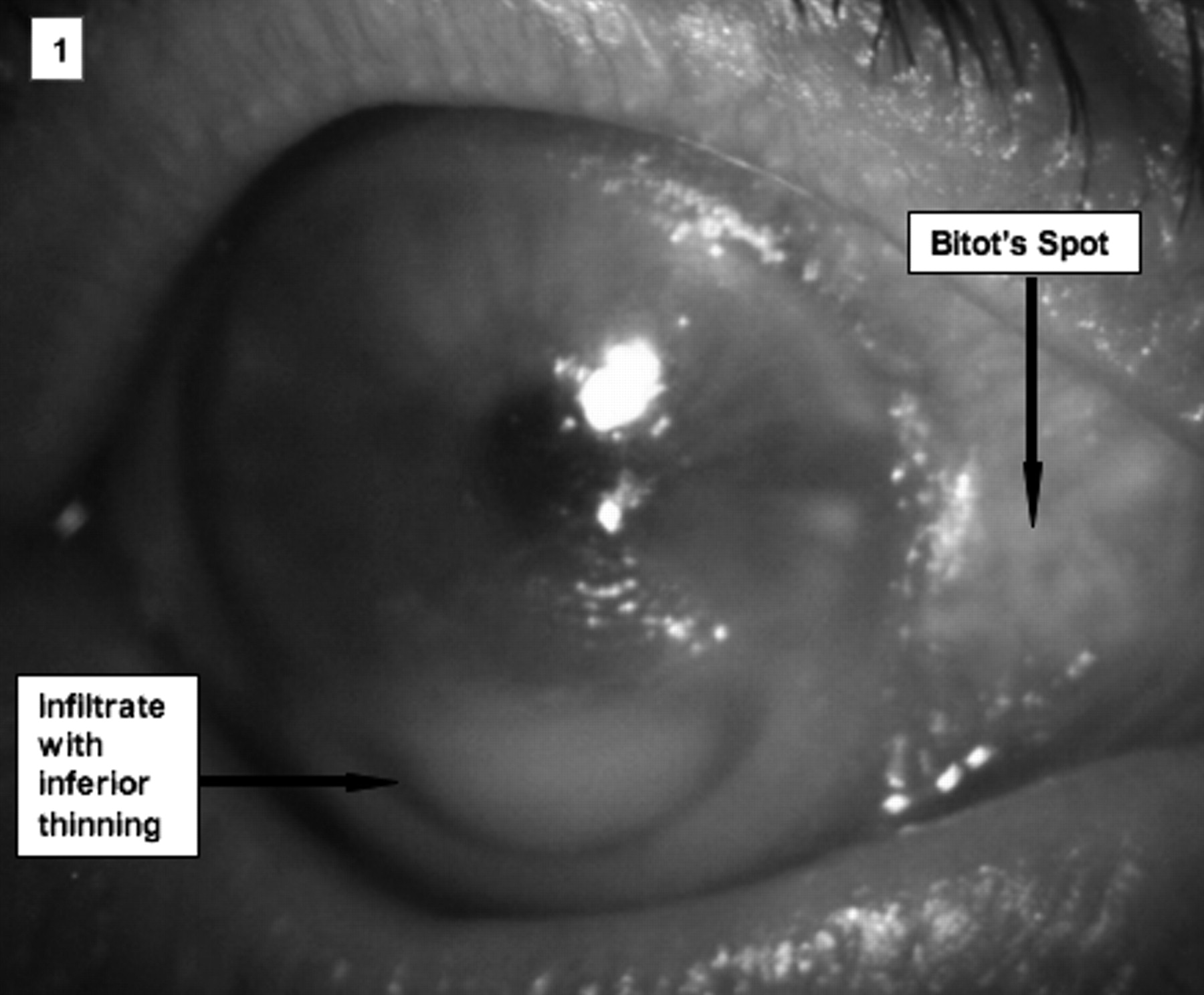
The patient was admitted under the cornea team and investigations revealed severe malnutrition with multiple vitamin and electrolyte deficiency. A detailed history revealed that the lady had small bowel resection 18 months ago following acute intestinal infarction. She was a chronic alcoholic and was on a poor diet. At presentation, her weight was 39 kilograms. Vitamin A deficiency was confirmed by a serum concentration of <0.10 Umol/L (normal range 0.70–2.8 Umol/L). The patient also had an acute electrolyte imbalance, hypoalbuminaemia, vitamin D, zinc, iron, calcium and magnesium deficiency and alcoholic liver disease.
She was treated by a multidisciplinary team, which included the ophthalmologists, gastroenterologists and dieticians. The initial treatment was with intensive multivitamins and oral vitamin A along with topical gentamicin and cefuroxime eye drops.
The corneal ulcers responded well to treatment and three months later, the patient's vision improved to 6/18 right eye and counting fingers left eye. The poor vision in the left eye was due to residual significant corneal scarring. By six months, the vitamin A levels had risen to 0.68 Umol/L together with a marked improvement in her electrolyte imbalance. She had gained weight and was physically significantly better off with treatment.
Discussion
In 1933, vitamin A was isolated from the retina by Geord Wald and his co-workers. Vitamin A is an essential fat soluble vitamin, required for appropriate functioning of the skin, retina and ocular surface. 1
Prevalence of xerophthalmia, the ocular manifestation of vitamin A deficiency, has been considered as the primary reference standard for the assessment and determination of vitamin A deficiency as a public health problem. 2 Xeropthalmia results from inadequate function of the lacrimal glands which produce tears. When xerophthalmia is due to vitamin A deficiency, the condition begins with night blindness and conjunctival xerosis (dryness of the eye membranes) and progresses to corneal xerosis (dryness of the cornea), and in the late stages, to keratomalacia (softening of the cornea). 3 Bitot's spots are a heaping of desquamated, keratinised epithelial cells, which form a slightly raised area on the conjuctiva. 3 This is a sign of longstanding deficiency, which respond well to treatment.
Worldwide the major cause of hypovitaminosis A is malnutrition. It is a leading cause of childhood blindness in developing countries. 4 In developed countries, there have been increasing reports of vitamin A deficiency recently due to increase in obesity-related bariatric surgery and alcohol-related pancreatitis and liver disease. One study found 52% of patients to be vitamin A deficient one year after surgery, despite oral vitamin A supplementation. 5
Our patient had severe malnutrition and multivitamin deficiency (vitamin A, zinc, iron) secondary to anorexia, small bowel ischemia and alcoholic liver disease. All these factors contributed to her clinical state.
The small intestine and liver play key roles in the metabolism and conversion of retinylester derived from the diet to the stored retinyl esters transported to the conjunctival goblet cells and retina. Zinc facilitates this process. Zinc deficiency results in impaired synthesis of proteins with rapid turnover such as retinal binding protein. This impairment affects retinol transport by retinal binding protein from the liver to the circulation and other tissues. Excess alcohol consumption also results in increased competition for alcohol dehydrogenase, required to convert retinol to retinaldehyde. Iron deficiency has also been thought to contribute to vitamin A deficiency, by mechanisms, which are still not completely understood.
It is very important to consider a diagnosis of xerophthalmia when presented with severe dry eyes, as it is a preventable cause of blindness. Monitoring patients with risk factors of hypovitaminosis A in a multidisciplinary team can help detect early signs and provide a rapid diagnosis of a potentially fatal and blinding condition. Our case demonstrates that hypovitaminosis A, even in a severely advanced stage, responds well to prompt diagnosis and appropriate treatment.
Footnotes
DECLARATIONS
Footnotes
Acknowledgements
None